


Yale Just Proved COVID Vaccine Injury Exists and Spike Production Persists for Years Inside The Body
Reviewing the consequences of the reckless steps used to make the vaccines and the immunological damage which followed

Last year, I learned of a Yale study which had discovered the COVID vaccine persisted in the body and caused long term immunological impairments—something I believe relates to the egregious production process that characterized the COVID-19 vaccines.
Since I did not want to interfere with the publication process, I held off from disclosing anything within the study which had not already been leaked by someone else. Today the study was pre-published, so I can now discuss what they found (in a heavily revised version of the previous article). The first half of this article provides the context for that study, while the second half discusses it (e.g., that the vaccine spike protein can persist in the body for at least 709 days and cause at least two years of chronic immunological suppression and autoimmunity that directly correlate to the presence of chronic illnesses).
Note: as this study was conducted by a team of immunologists, they primarily focused on immunologic changes (and as a result many of the other chronic consequences of vaccination were not discussed). Additionally, it should be noted that they originally strongly endorsed the vaccination (both to prevent COVID and to treat long COVID—which is often disastrous) and came from a very pro-vaccine institution. As such, the fact they were willing to change their stance on this should be acknowledged (and indicates a lot of work went into verifying the accuracy of their data).
Upsides and Downsides
A lot of things in life are trade-offs, and as I’ve gotten older, more and more I’ve come to appreciate how many things in our society boil down to the fact that the options for addressing them (at least within the existing paradigm) all have significant downsides, so in many cases no solution exists which is satisfactory to all parties involved.
As such, this dilemma is typically managed by some combination of the following:
•Having a biased focus which emphasizes the benefits of an approach a side supports and downplays its downsides (or conversely disproportionately focuses on the downsides of an opposing position). To this point, I’ve had countless issues I’ve debated both sides of and been able to effectively persuade audiences of each one—which highlights how subjective many of the entrenched beliefs we hold actually are (and, in turn, is why I put so much work here into fairly presenting both sides of each controversial topic I cover).
•Sweeping the downsides under the rug and gaslighting the populace into believing they don’t exist.
•Blitzing the public into supporting a questionable policy before they have time to recognize its downsides, and if that fails, overtly forcing them to go along with it.
Note: I believe one of the reasons why governments frequently do horrible things to their people is because they are put in the position of having to “solve” a problem (but with no truly satisfactory way to do it), so they become habituated to using the three previous strategies to push their chosen policies along and simultaneously develop a collective mentality that those questionable approaches are necessary for the “greater good.”
There are many different manifestations of this dilemma, many of which I believe are essentially reflective of a foundational concept in medicine—sensitivity and specificity.
An ideal diagnostic test would catch every instance of a disease (100% sensitivity) and simultaneously never have a false positive (100% specificity). Unfortunately, in almost all cases, this is impossible to do, and instead a trade-off exists where you can either prioritize sensitivity (which leads to a significant number of false positives) or prioritize specificity (which leads to a significant number of false negatives). During COVID for example, a decision was made to prioritize sensitivity with the PCR tests (by having a high replication cycle thresholds) so no cases of COVID would be missed, but this resulted in such poor specificity that the PCR tests effectively became worthless (except for drumming up fear) since they produced so many false positives.
As such, when tests are designed, attempts are made to ensure there is a good balance between sensitivity and specificity. In some cases this is successful (e.g., there are many lab results we will take at face value), but in many other cases, given the technology involved, it’s not really possible to do so (or it is, but lobbying led to over-diagnosis so a medical product could be sold).
Similarly:
•Many policies in the justice system aims to enact fall into this same situation. For example, an ideal death penalty is robust enough to deter murder (and keep violent criminals away from the public), but simultaneously lenient enough that it doesn’t accidentally execute innocent individuals. Since there is no way to have both perfect sensitivity and specificity on this, different states take radically different approaches to how they enforce the death penalty (lying all along the spectrum between sensitivity and specificity). Likewise, our judicial system was founded under the principle “innocent until proven guilty” whereas many other countries have judicial systems that are the exact opposite.
•In medicine, one of the greatest challenges is finding the appropriate dose, as people differ, so what might be a safe and therapeutic dose for one person could be toxic for another. As such, standardized doses are typically chosen by finding the best overall balance between efficacy (a sufficient dose) and safety (avoiding a toxic dose), but for many drugs, the standardized dose leads to many more sensitive patients becoming severely injured by the drugs (which is then commonly “addressed” by gaslighting those injured patients).
Note: a much more detailed discussion on the art of dosing can be found here.
•Every medical intervention has its risks and benefits, and ideally, the job of a physician should be to accurately weigh those to determine the best treatment for a patient (while simultaneously conveying what they are to the patient). Unfortunately, in many cases, they don’t (which is a large part of why patients are so dissatisfied with the medical system).
Overall, there are three key takeaways from this paradigm I wish to focus on in this article:
1. It is often incredibly difficult to find an acceptable balance between sensitivity and specificity, and many of the conventions our society now follows were the result of years of debate and protest from both sides to find a palatable middle ground between the two.
2. In almost any sphere I frequently find rushed attempts to find an acceptable balance between two conflicting positions to be immensely flawed and prone to creating significant issues in the future.
3. Many of the issues with the vaccine program are encapsulated by this framework.
How Vaccines “Work”
Note: many believe the immune system is one of the least understood parts of physiology, something I would argue is a result of immunological research being focused on making profitable pharmaceuticals (e.g., vaccines) rather than understanding how it works.
In the classical conception of immunity, there are two types, innate immunity and adaptive immunity, with the innate response being relatively nonspecific (so it can work against a wide variety of infectious threats, including those the body has never seen before) and the adaptive one, which is uniquely suited to eliminating the specific invading organism.
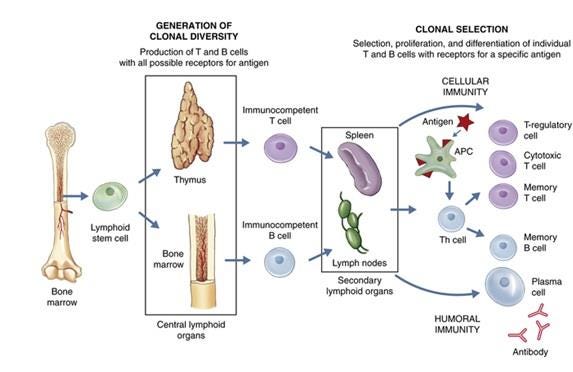
The most widely accepted explanation for how the adaptive immune system works is “clonal selection theory” which states that the immune system:
1. Uses a random generation process to create a vast pool of potential antigen matching sequences.
2. Has vast number of different immune cells that each have those sequences attached to them circulate the blood stream.
3. Waits for one of those immune cells to contact an invading pathogen that the sequence it carries matches.
4. Have each of the immune cells be programmed to start rapidly reproducing once they get a sequence match.
5. Through the previous 4 steps, make it possible to produce a large number of immune cells which are specific to an invading organism (because they can bind to their antigens and alert the rest of the immune system to the organism’s presence), and thus effectively neutralize the infection.
6. Once the process is complete, to leave behind memory B cells, which match the invading pathogen and are able to stimulate the immune response in a much more rapid fashion (thereby shortening the time that steps 3 and 4 take).
The theory behind vaccination is that if the specific immune response and memory B cells can be created before the body encounters a dangerous microbe, this can:
•Allow the body to mount a robust immune response before a harmful invading organism has time to multiply within the body and cause significant damage.
•Cause individuals to rapidly clear infections (rather than needing to wait for the adaptive response to kick in), thereby reducing or eliminating the amount of time they can spread the disease into the population.
•Cause individuals to develop an immune response at the site of infection (e.g., the membranes of the nose and throat), thereby preventing the organism from being able to colonize those areas and thus preventing its transmission.
Being able to do this is hence immensely appealing to governments, as it allows a single intervention (the vaccine) which can easily be distributed to everyone in a top-down manner (which is what governments are good at doing) to address a longstanding problem (infectious disease outbreaks) and more importantly, to allow the government to present the appearance of working in earnest to safeguard the public’s health. Because of this appeal, throughout history, governments will get deeply invested in vaccine programs, and then once issues arise with those programs, double-down on the vaccine (e.g., with mandates) rather than reconsider the wisdom of the vaccine program.
Note: in a previous article, I showed how this misguided and tyrannical conduct has existed ever since the first vaccine (smallpox).
Vaccine Production
To “work” vaccines aim to mass produce a dangerous organism’s antigen without the organism itself being present and then administer that antigen into the body. By doing so, the intermediate stage of an infection (where the organism has already reproduced enough inside its host to have a large number of antigens be available to match a circulating immune cell) can be achieved without the individual being in danger of being damaged or overwhelmed by the infection.
Unfortunately, unlike chemicals which can be rapidly synthesized, antigens are complex enough that they can only be produced by biological systems. As such, to produce the antigen, one of the following is typically done.
•Mass produce the infectious organism, then “kill” it so that its antigens can be collected, but the organism itself is not able to cause infections.
•Genetically modify another organism to mass produce a desired antigen, then kill it and extract the antigen (e.g. the HPV vaccine does this with modified yeasts).
•Modify the live pathogen (typically a virus) so that it can still cause the infection and reproduce inside the recipient but simultaneously is “weakened” so that it is less likely to cause illness.
•Genetically modify a “benign” virus to contain the antigen but be unable to replicate in the human body, then mass produce it outside the body, and have the body develop an immune response to the virus and the antigen on it once it is injected.
•Introduce mRNA into cells so human cells can produce large amounts of the desired antigen, which the immune system then sees (e.g., on the surface of the cells) and develops an immune response to.
The basic problem is that none of these approaches are perfect, and each has both its ups and downsides. For example:
•Most can create autoimmunity.
•In those where only a single antigen is used (and the virus spreads from human to human), if the vaccine actually works, it rapidly stop working because the pathogen quickly evolves a new antigen that no longer matches the vaccine.
•It contrast, the multi-antigen ones (which don’t have that issue) are typically live attenuated vaccines, which then can cause those with weakened immune systems to develop infections from the vaccine itself (e.g., this happens with the polio vaccine—which is why the primary cause of polio now is from the vaccines rather than natural infections, but also can happen with others like the shingles and measles vaccine).
Furthermore, some infectious diseases respond fairly well to vaccination, but the majority do not, so at this point, the vaccine industry has already picked all the “low-hanging fruit” and hence faces an existential struggle to develop new proprietary (patentable) vaccines it can bring to market. For example, had it not been for COVID-19 (SARS-CoV-2), a SARS vaccine would have never been brought to market as it was well recognized the SARS virus was poorly suited for vaccination (which what we then saw throughout the pandemic).
Finally. even if a vaccine “works” it still has to be manufactured, and there are numerous cases of the tradeoffs being made resulting in a disaster. For example:
•To make the inactivated polio vaccine, the live polio virus had to be exposed to formaldehyde. However, the challenge with this was that if too much formaldehyde was used, it would damage the antigens on polio to the point they no longer matched those on the poliovirus, whereas if too little was used, some of the polioviruses would remain active and could then give the vaccine recipient polio. The creator of the vaccine (Salk) opted to prioritize efficacy over safety, which the government in turn supported, even when one of their own scientists (Bernice Eddy) warned them against releasing the vaccine (as it caused polio in her lab). That 1955 vaccine then infected at least 220,000 people with live polio virus in Cutter's vaccine, of whom 70,000 developed muscle weakness, 164 were severely paralyzed, and 10 died.
Note: an identical issue had happened on a smaller scale (9000 infections, 12 severe cases, 6 deaths) in 1935 with an earlier version of the inactivated polio vaccine. Likewise, (as I showed here) there have been dozens of incidents where an insufficiently inactivated or attenuated diphtheria, rabies or yellow fever vaccines severely injured hundreds of people (as the attenuated vaccines faced a similar issue with it being easy to over or under attenuate).
•Growing viruses for vaccines requires having a cell culture to grow them in. Monkey kidney cells were chosen because they worked well for doing this, but unfortunately were contaminated with the cancer causing SV40 virus. In 1962, Eddy again warned the government about the vaccine, but they still chose to give it to the public (and retaliated against her for speaking out), which in turn led to a wave of cancer sweeping through America, which until the COVID-19 vaccines was unprecedented:
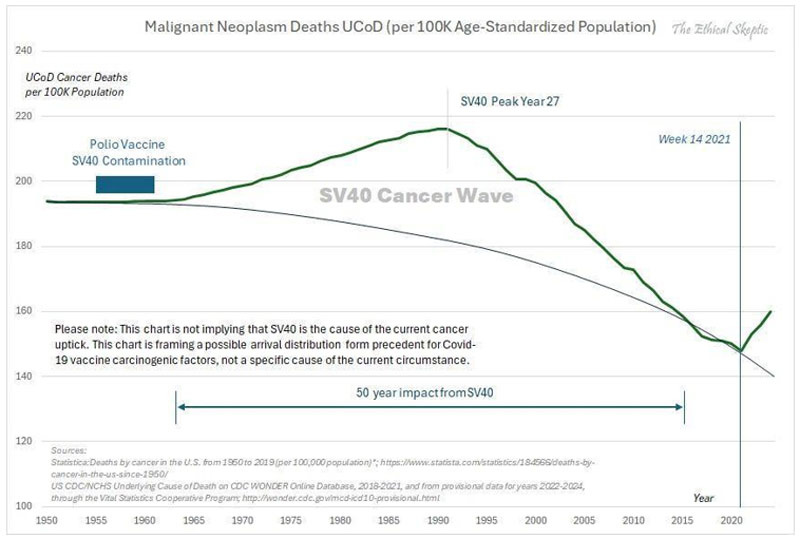
Note: many other viral vaccines (particularly the live ones) also have had harmful viral contaminants identified within them, but unlike SV40, that contamination has not been acknowledged. Most noteably, a strong case can be made that HIV emerged from virally contaminated vaccines (that had been grown in monkey tissues).
•After a potentially dangerous strain of influenza (due to it having similarities to the 1918 influenza) was identified, a rush began to make an emergency vaccine for it (despite the FDA’s chief influenza expert Morris accurately warning that strain posed no risk to America). Since it took a while to cultivate the virus for a live attenuated vaccine, in order to make the vaccine be produced fast enough to hit the market before the influenza strain disappeared, a decision was made to hybridize it with the PR8 strain, a fast growing influenza strain directly descended from the 1918 influenza. Morris warned against doing this, but was ignored (and fired). That 1976 vaccine subsequently injured a large number of people (including some of our patients) and was a publicity disaster for the US government.
•The anthrax vaccine used during (and after) the Gulf War required growing large amounts of the bacteria, killing them, and then filtering out the most toxic components from the final vaccine preparation. The issue the manufacturer ran into was that because of how dirty the vaccine was, its contaminants clogged the filters the manufacturer used, so “solve” the problem and be able to manufacture the vaccine at scale for the military, the manufacturer opted to use larger filters which did not clog, but also didn’t filter many of the toxic components out of the final products—which resulted in one of the most harmful vaccines in history being unleashed upon our military.
•Due to the challenges in producing it, the DTP vaccine (another killed bacterial vaccine) was notorious for having hot lots that killed their recipients (or left them with brain damage). In fact, one FDA pertussis specialist in 1976 stated:
Pertussis vaccine is one of the more troublesome products to produce and assay. As an example of this, pertussis vaccine has one of the highest failure rates of all products submitted to the Bureau of Biologies for testing and release. Approximately 15-20 percent of all lots which pass the manufacturer’s tests fail to pass the Bureau’s tests.
Eventually, the injuries that vaccine created led to so many lawsuits that the manufactures could not afford to continue producing the vaccine, at which point, the 1986 Vaccine Injury Act was passed. This shielded the manufactures from all future liability from it (hence allowing them to stay in business), and eventually incentivized the production of a safer but more costly pertussis vaccine.
•Frequently when an antigen is produced, it cannot solicit a sufficient immune response (unless a lot of it is used—which frequently makes the vaccine too costly to produce). To solve this problem, cheap (and toxic) adjuvants which enhance the immune response to the antigen are used, thereby allowing an affordable amount of antigen to be required for the final product. When the HPV vaccine was developed, it was discovered that its antigen (along with standard adjuvants) could not mount a sufficient immune response to get FDA approval, so a decision was made to use an experimental (but much stronger adjuvant) which worked—but also gave a large number of recipients autoimmune disorders (at least 2.3%). Nonetheless, that trade-off was also accepted to get it to market.
In short, if you look at all these cases, a consistent pattern should be clear. Whenever there is a choice between getting a dangerous vaccine to market or holding off because there isn’t a way to do it safely, the vaccine industry will always do the risky approach (especially in “emergency” situations) as they know they can unconditionally rely upon the US government to promote the product as “safe and effective” and then legally shield them from the disaster which inevitably follows.
COVID-19 Vaccine Hurdles
When COVID-19 began, the industry faced three major issues:
•Whoever was the first to develop a successful vaccine would make a lot of money, but those whose products took longer to reach the market would like miss out on the bonanza.
•There was a finite amount of time the lockdowns could be sustained (which made people want to vaccinate so they could be “free”) and it was very likely the population would rapidly develop herd immunity to COVID-19—so they was a limited window to get a vaccine to market.
•It was extraordinarily difficult to make a safe and effective vaccine for SARS (e.g., decades of work had not yielded a viable product).
Fortunately for the industry, the WHO (and Bill Gates), in 2010, had enacted their “Decade of Vaccine” plan, and with the World Economic Forum (between 2014-2016) had developed a framework for pushing through emergency vaccines that could bypass the regulatory process in the event of a health “emergency.” This framework gave lavish lavish fiscal incentives for vaccine manufacturers and positioned unaccountable organizations like the WHO, Gates foundation, or the World Economic Forum as the directors of a future pandemic response.
Shortly after that framework was finished, the FDA on January 13, 2017 released extremely detailed regulations for obtaining emergency use authorizations, and five days later, Gates publicly announced his plan to the world. This framework was endorsed by pharmaceutical companies, including Pfizer Moderna and J&J, and when Operation Warp Speed was finally conducted in 2020, it mirrored the framework Gates had previously developed.
Note: Event 201, a Gates funded “simulation” exercise modeling the release of a dangerous SARS virus from China was conducted on October 18, 2019. Reading through it in December of 2019 allowed me to accurately predict how COVID-19 would play out. Likewise, on 9/4/2019, Gates invested 55 million in the company that produced Pfizer’s mRNA vaccine—which in two years was worth 550 million.
So as you might expect, the industry chose to adopt the fastest possible production pathway, and was quickly granted the legal immunity (and lavish funding) necessary to accomplish that.
mRNA Vaccine Challenges
Note: one of the major advantages to the mRNA platform was that its production turn around time was much faster than existing alternatives (e.g., growing a virus in chicken eggs). This was a key reason why Fauci’s agency made decades of investments to develop the platform (as with the existing options, seasonal flu vaccines had to start being produced long before the circulating strain was known—which frequently led to the annual flu vaccine being for the wrong strain).
For the mRNA vaccines to “work,” the following needed to occur:
1. An antigen needed to be chosen that was highly likely to elicit a robust immune response that suggested SARS-CoV-2 immunity (and hence could win approval).
2. mRNA matching that antigen needed to be produced at scale.
3. The mRNA needed to be able to get into cells.
4. Once it got into the cells, the mRNA needed to be produce sufficient protein to create an immune response.
Many who have examined Pfizer and Moderna’s vaccines were perplexed by the design that was chosen, as many of the immensely harmful decisions that were chosen strongly imply the vaccine was deliberately designed to harm as many people as possible. While this very well might be the case, many of those issues can instead be explained by the fact each of those 4 challenges was addressed in a way that prioritized getting a vaccine to market rather than producing a safe one.
For example, the spike protein was the most reactive (immunogenic) part of the virus and necessary for SARS to infect cells, so it was an ideal vaccine target. However, it was also a terrible antigen to chose as:
•The spike protein had a significant overlap with human tissues so it was likely to trigger autoimmunity if produced throughout the body.
•The spike protein was highly toxic, so if it was mass produced within the body, it likely would injure the recipient.
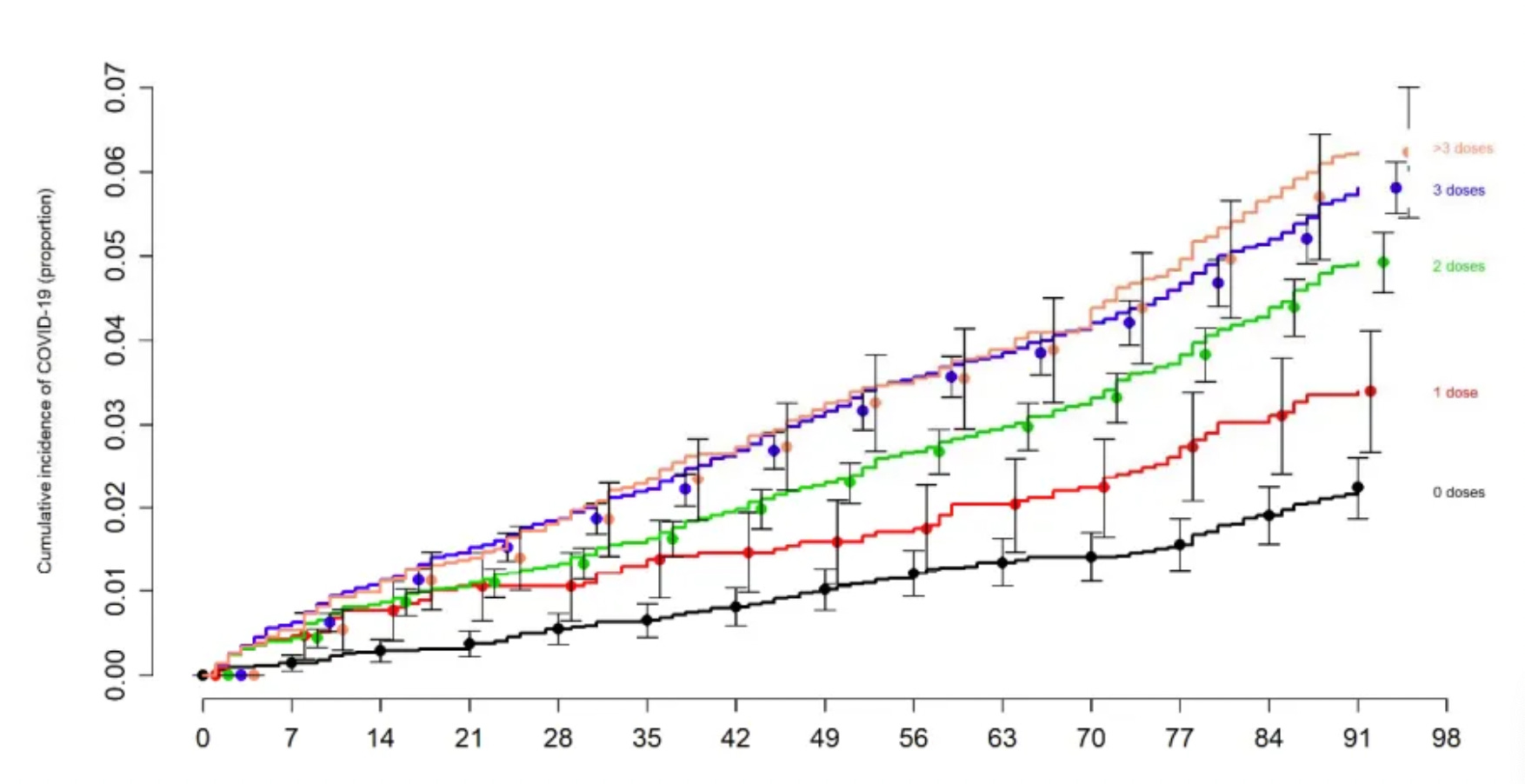
•It was a rapidly mutating part of the virus, which guaranteed the circulating spike protein would quick evolve into a variant the vaccine did not work against it—leading to the remarkable situation where we mandated a vaccine for an extinct virus (which, in turn, caused those vaccinated to become more likely to catch COVID-19 as their immune systems were continually primed to respond to a different virus from that they were exposed to)—something best demonstrated by the Cleveland Clinic’s study of 51,011 people):
Similarly, when I was trying to understand the acute toxicity of the vaccines, I suspected the lipid nanoparticles used to produce the vaccines had to be responsible for their acute toxicity (e.g., which could be seen within seconds of it being put into blood) as those effects onset far faster than it seemed possible for significant numbers of spike proteins to be produced.
After I looked into, I realized that for decades it had been deemed impossible to produce mRNA carrying lipid nanoparticles that had sufficient safety and efficacy to produce viable vaccines (to the point pioneers in the technology like Robert Malone who had invested decades of work into it abandoned it as they felt it was impossible to make a lipid nanoparticle which were not cytotoxic). In turn, when I reviewed leaked Pfizer regulatory documents, I noticed that their lipid nanoparticle had been chosen on the basis of it being the only one that had efficacy—again suggesting safety wasn’t taken into consideration.
Similarly, because of the toxicity of the mRNA lipid nanoparticle combination, it was very difficult to determine an appropriate therapeutic dose (as the vaccine was either too toxic or not effective—hence why Malone abandoned in). I thus was very curious to see how the doses would be chosen, and then was astonished that Moderna chose a dose that was 3.3X higher than Pfizer’s—something I interpreted as a reflection of the fact all of Moderna’s mRNA products had failed, the company had a sociopathic CEO, and the company was desperate to bring a viable product to market.
In turn, as I showed here, once Moderna came to market, it had a much higher rate of adverse injuries (including deaths) than Pfizer, but was completely left alone by the regulators (which is a gross violation of regulatory standards), and something I suspect was in part due to the NIH having massive investments in Moderna. Likewise, one of the curious things noticed with adverse reactions to the Pfizer vaccines was that lot toxicity seemed to directly correlate with sequential lot numbers, suggesting a large scale dose-response study was conducted after the vaccines hit the market.
Note: there were many other safety issues with mRNA technology (e.g., synthetic mRNA induced immune suppression and antigenic spike protein coating cells and causing the immune system to destroy those cells) that are beyond the scope of this article.
mRNA manufacturing
In my eyes, the two biggest production issues with the mRNA vaccines were producing them at scale and then having them produce spike protein in the body at scale.
Note: these were easy to predict as one of the greatest challenges the pharmaceutical industry, and particularly biotech faces is producing their products at scale—a process which typically takes years to work out, but for Operation Warp Speed needed to be done in a few months.
mRNA design
A major challenge with synthetic mRNA was that the immune system would rapidly break it down, which resulted in not enough of the spike protein being produced to trigger a sufficient immune response. This in turn was “solved” through pseudouridylation, a process where pseudouridine replaces uridine in mRNA molecules as pseudouridylated mRNA resists immune system degradation.
Unfortunately:
•This process occurs in a very limited and tightly regulated manner inside the body. At the time the mRNA vaccines were developed, there was limited understanding on the biological significance of pseudouridylation, however many (e.g., Robert Malone) felt the preliminary data showed this approach had serious risks (e.g., immune suppression).
•These existing technology for pseudouridylation causes it to occur in a random and haphazard way. As such, rather than being able to determine a “safe” dose of pseudouridylation, an all or nothing approach had to be adopted, which in turn led to a significant number of vaccines having “excessive” pseudouridylation (either due to how much of it happened to the mRNA or where in the mRNA the pseudouridylation occurred). In short, this approach was extremely reckless, and akin to playing Russian roulette but hoping everything worked out.
In turn, the pseudouridylation did “solve” the mRNA degradation problem (to the point it won an unscrupulous Noble Prize), but it also created a new issue—the mRNA (and spike protein production) persisting in the body for a prolonged period, and likely due to the haphazard nature of the vaccine’s production, it persisting much longer in some cases that others. Lastly, while this invention “won” the Noble Prize, there were also viable mRNA vaccines that did not utilize it (and hence did not have the risks it entailed).
Note: Codon optimization (which increases protein production from mRNA) may have also caused the vaccine to excessively produce spike protein in the cells.
mRNA preservation
One of the major issues with synthetic mRNA is that its immensely fragile, so even if it could be protected from immune degradation within the cells (e.g., via pseudouridylation) it still was highly susceptible to common environmental factors. As such, when the lots of finished vaccines were examined by regulators, they determined there was both significant degradation of the mRNA and significant variability in what mRNA was preserved.
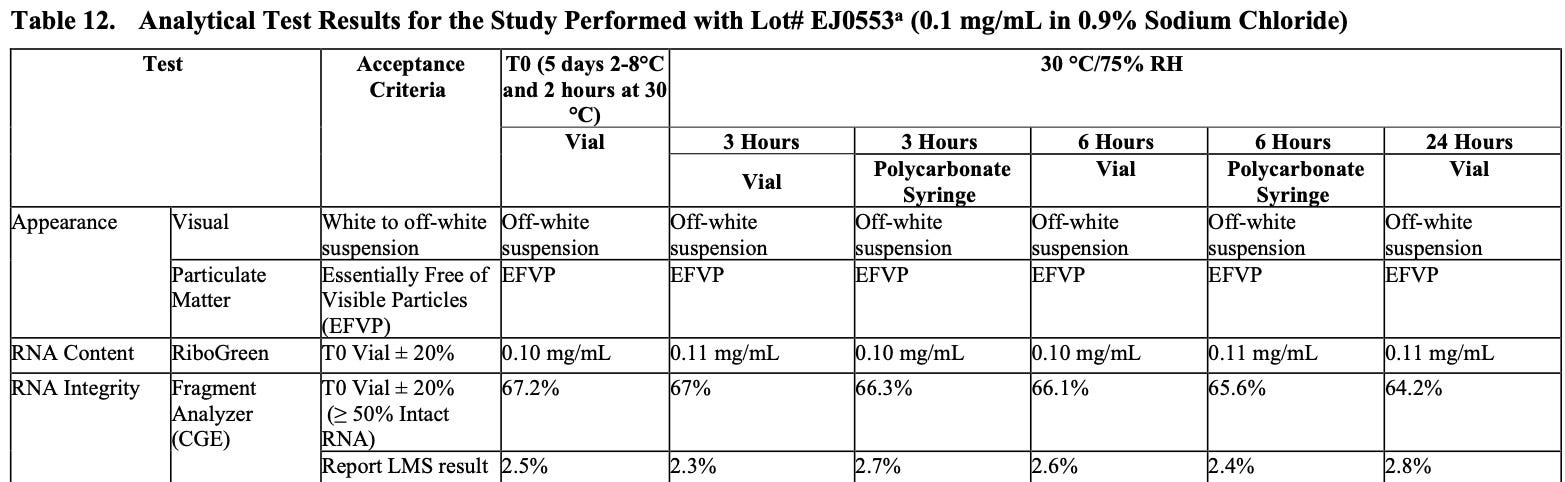
As this degradation and the resulting “truncated mRNA” was one of the primary concerns from the drug regulators Pfizer “solved” this problem by having all of their vaccines be ultra frozen (under the belief this would prevent mRNA degradation). However, this was largely for show, and before long the practice was abandoned (e.g., many vaccine sites had vials sitting outside throughout the day).
Note: at the time I learned about it, I thought that the primary issues would be broken mRNA sequences producing unintended and potentially harmful protein sequences. We now believe it’s actually the opposite, and that this breakdown process was a blessing in disguise, as evidence gradually accumulated that the older vaccines were and the further from their production site they were injected into the body, the less toxic they were—suggesting that the vaccine’s toxicity was mitigated by portions of its mRNA breaking down and hence preventing it from producing as much spike protein.
Process 1 vs. Process 2
The original process used to produce the mRNA vaccine had two ways it could be done. In the cleaner process (which was used to produce the vaccines for the trials), mRNA was produced through controlled replications with minimal contaminants present. Unfortunately, this process could not be scaled.
As such, an alternative approach was done:
•E. coli bacteria were genetically modified to have DNA that contained the spike protein, antibiotic resistance, and the SV-40 promoter.
•Those bacteria were mass produced, then doused with an antibiotic (so those without the resistance gene and thus the spike protein gene) died and did not contaminate the final product.
•The remaining bacteria are killed and their DNA is extracted.
•An mRNA polymerase is used turn that bacterial DNA into vaccine mRNA.
•Everything besides the mRNA is eliminated.
•The mRNA is packaged into lipid nanoparticles.
The essential problem with this process was that it was not feasible to remove many of the contaminants from each stage of production and there was significant room for variability at each stage (and thus in the final product). While many contaminants could be an issue, the vaccine safety community primarily focused on the plasmids as:
•They’ve repeatedly proved plasmids were present in the vaccine.
•The SV40 promoter (a key part of the cancer causing SV40 virus) was grafted onto the plasmids as this was an effective way to increase mRNA production.
•Plasmids had the potential to alter the human microbiome and genome (especially since the SV40 promoter will bring DNA into the nucleus)—which is particularly concerning since vaccine plasmids have now been shown to get into cell nuclei.
•If there was a genomic integration, it was likely creating indefinite spike protein production in the cells.
•When vaccine lots were analyzed for their plasmid levels, it was found the lots which more frequently injured their recipients had higher levels of DNA plasmids (suggesting either harmful genomic integration was occurring, that the plasmids were toxic absent genomic integration, or that they were a proxy for other harmful contaminants).
Inconsistent Manufacturing
Each of the previous points illustrates that the vaccine industry was not ready to bring the mRNA vaccines to market and that the manufacturing of them was rife with errors. Many other points also support this such as:
•Japan pulled 1.63M vials of Moderna’s vaccine after visible metal particles were found in them and when examining vaccine vials, Ryan Cole found glass shards in the vaccines. Both of these suggest the production of the vaccines was rushed to the point basic quality control steps were not taken.
•When Ryan Cole did a recorded examination of the vaccines with Del Bigtree they found:
We looked at all the different vaccines and I think one of the conclusions we came away with is that it’s just a hodgepodge..there were vaccines that seems as though there were no particles within them, almost nothing there it was almost like a saline shot and then there were Pfizer’s that were just packed with them and you just get the sense that the manufacturing of this is totally inconsistent…some were more concentrated and some were less.
Note: this suggests that there was either very poor mixing when the vaccines were packaged (leading to some having lots of the lipid nanoparticles and others none) or that the vaccine manufacturers were unable to produce enough vaccine to meet the existing orders and switched to packing placebo vials to meet their contracted orders.
•In one mass spectrometry examination of 4 vaccine vials, it was determined that the lipid nanoparticles, but not the mRNA, were present in each of the vials. This suggests that the vaccine was not prepared in a consistent manner, or that the manufacturers ran out of mRNA to fill the vaccines with.
•A large body of evidence from the adverse event reporting databases (compiled here) demonstrated that the toxicity of the vaccine lots greatly varied, which again was likely explained by inconsistencies in their manufacturing.
Note: in a previous article about the mRNA lipid nanoparticles, I showed how inconsistencies in the manufacturing of the vaccines likely explained why the vaccines tended to affect different organs in the body (as their charge was affected by how much mRNA they contained and the area they deposited in the body was influenced by their charge) and why some individuals had acute reactions to them.
Blot Gate
One method of analyzing which proteins are present is with an approach known as “Western Blot.” Periodically, individuals will fake Western Blots (which can be detected because its very easy to identify computer generated ones).
With the COVID-19 vaccines, Western Blots were meant to serve as a quality control measure which ensured the mRNA vaccine were producing their intended protein. However, when we examined the available Western Blots we discovered:
•Some of them were computer generated (and hence likely fake).
•Others showed proteins besides the intended vaccine antigen were there (possibly due to broken RNA fragments being turned into proteins).
All of this again suggested that there were serious manufacturing issues with the COVID vaccines, but a decision was made to sweep all of that under the rug to protect the vaccine manufacturers (particularly since the drug regulators willfully ignored this fraud).
Note: this is similar to how there was extensive fraud throughout the COVID-19 clinical trials to exaggerate vaccine efficacy and safety (which essentially invalidated all the data was gathered), yet even after the trial participants and trial supervisors repeatedly notified the FDA, nothing was done. Likewise, shortly before the vaccine rollout, Vanity Fair published an article highlighting the serious issues in Americas’s vaccine manufacturing plants and that the FDA essentially was unable to monitor them—hence arguing things would get even worse during Operation Warp Speed.
mRNA persistence
Once the COVID-19 vaccine hit the market and the injuries began to mount, we noticed a three curious patterns.
1. The susceptibility to vaccine injuries greatly differed, but in many cases seemed to cluster (e.g., I knew a husband and wife who got vaccinated at the same time and both have near fatal complications from the vaccine).
2. A significant number of individuals appeared to be sensitive to vaccine shedding, something that is supposed to be “impossible” but nonetheless was occurring in a fairly repeatable manner to a large number of people, with symptoms similar to COVID vaccine injuries but typically less severe.
Note: everything we know about shedding is discussed here.
3. Many individuals with vaccine injuries appeared to be suffering toxic reactions to spike proteins in their blood steam months if not years after vaccination. For example:
•Autopsy studies (conducted on individuals who died suddenly up to 6 months after the vaccine) have shown that their tissues were flooded with spike protein. Beyond the inflammatory and necrotic responses to the spike protein being their likely cause of death, it also suggested those individuals had had large amounts of spike protein being perpetually produced within their bodies.
•Both myself and Pierre Kory have come across numerous cases of individuals with vaccine injuries who, months, if not years after vaccination, respond to spike protein binders (suggesting unbound spike protein was causing their issues—particularly since their spike protein levels dropped). Additionally, those individuals either remained recovered, significantly regress, or partially regress once the binder is stopped (implying there is a sustained but possibly diminishing production of spike protein in the body in many vaccine injured patients).
•The only commercially available test for the spike protein (offered by Quest) measures existing antibodies to the spike protein receptor binding domain, and provides values anywhere from 0-25,000 (or higher than 25,000). Clinically, we’ve seen that long COVID rarely get levels above 4,000, whereas in those with vaccine injuries, it can be anywhere from 0-25,000 with many being over 25,000. In turn, a rough (but not precise) correlation exists between the antibody levels (which do not directly measure spike protein levels) and a patient’s illness (along with its levels improving or worsening generally correlating to a patient’s symptoms improving or worsening). Curiously, many patients do not have their antibody levels decline with time (which is what you typically see after a COVID infection), which again suggests spike protein is being produced within the body that then stimulates an immune response. Conversely however, some of these cases may instead have been from people who had antibody levels far above 25,000 who then had their antibody levels decline (but this cannot be detected as they are still above the 25,000 cut off).
Note: Alex Bereneson has also shared reports of vaccinated individuals who’ve had spike protein antibody levels over 25,000 for months after vaccination.
Pivotal mRNA Studies
When the COVID vaccines were pitched to the public, two of the greatest concerns were that the experimental gene therapies could change our DNA and that they would persist in the body for a prolonged period. To address these sales barriers, the media continually platformed experts like Paul Offit and Anthony Fauci) who dismissed us by continually saying things like:
The vaccines cannot enter the nucleus of the cell
mRNA from the vaccines breaks down rapidly in the cell, so it does not have time to enter the nucleus and change your DNA.
mRNA is not DNA, so believing mRNA can change DNA represents a fundamental lack of knowledge of biology.
These points raised red flags to me, as beyond their being issues with each of them, no data was ever provided to disprove genomic integration of the vaccine (which would have been quite easy to do). As such, I assumed the vaccines did integrate into the genome, and evidence would eventually emerge that they did (and likewise that at least some of the vaccines would continually produce spike protein in the recipients).
Throughout this process, two very important, but largely forgotten studies came out.
Note: due to the extreme scientific embargo on anything which challenged the COVID narrative, it is somewhat of a miracle either of these were published.
The first was a March 2022 study from Stanford which showed that both vaccine mRNA and spike protein persisted at high levels at least 2 months after vaccination. This was highly unusual for mRNA, and suggested something (e.g., the pseudouridylation) was preventing it from breaking down. Most importantly, the study did not go beyond 8 weeks, so it was likely the mRNA was persisting for a much longer time.
The second was a January 2023 study (with many Harvard authors) which found in adolescents and young adults who developed myocarditis within a few days of vaccination, that compared to controls, they had significantly higher levels of free spike protein circulating in their blood (due to them not forming antibodies which bound it). This in turn suggested that those who were reacting the worst to the vaccines lacked the ability to form antibodies which could counteract its effects in the body, which both explained why some individuals were so sensitive to the vaccine (e.g., shedding) but also that those likely to “benefit” from vaccination also would have mounted a robust response against a natural infection (hence invalidating the justification for getting vaccinated).
Note: with the smallpox vaccines, vaccination was deemed successful if there was a strong inflammatory reaction at the vaccination site, whereas if no reaction occurred, the vaccination was deemed unsuccessful and the individual was repeatedly revaccinated (as when it didn’t “take” the individuals could still get smallpox). Many early medical dissidents observed that severe reactions to the smallpox vaccine typically followed the vaccine not “taking.” They hence came to believe that the smallpox vaccine working was due to the recipient having a functional immune system that could both already fight off smallpox and create the superficial inflammatory reaction to the vaccine and that the vaccine was simply taking credit for what their immune system could already do. This study made me wonder if something similar has occurred with the COVID-19 vaccines.
Yale’s Listen Study
Most recently, Yale’s immunology team conducted a longterm study of the effects of vaccination on immune function, which represents a watershed moment in studying these injuries as there has been a longstanding embargo in the academic community of acknowledging these injuries.
Note: previously I predicted the one thing which could get the scientific establishment to begin publishing data on vaccine injuries would be Trump becoming president again as there would then be a political incentive to criticize them (as Trump endorsed the COVID vaccines).
As this represented the most pivotal data on creating longterm awareness of the harms of the COVID vaccine (e.g., beyond it being very detailed, it coming from Yale would make “long-vax” a condition) I have been in touch with participants throughout it (who’ve shared bits and pieces of the data coming out), all of which has been consistent with what we’ve been seeing in vaccine injured patients for the last four years.
Initially, in 2023, they shared some of their preliminary data as a 2023 pre-print (which has still not been formally published) which detailed the common symptoms seen in the 241 participants with post vaccination syndrome (PVS), which match what we’ve seen in clinical practice:
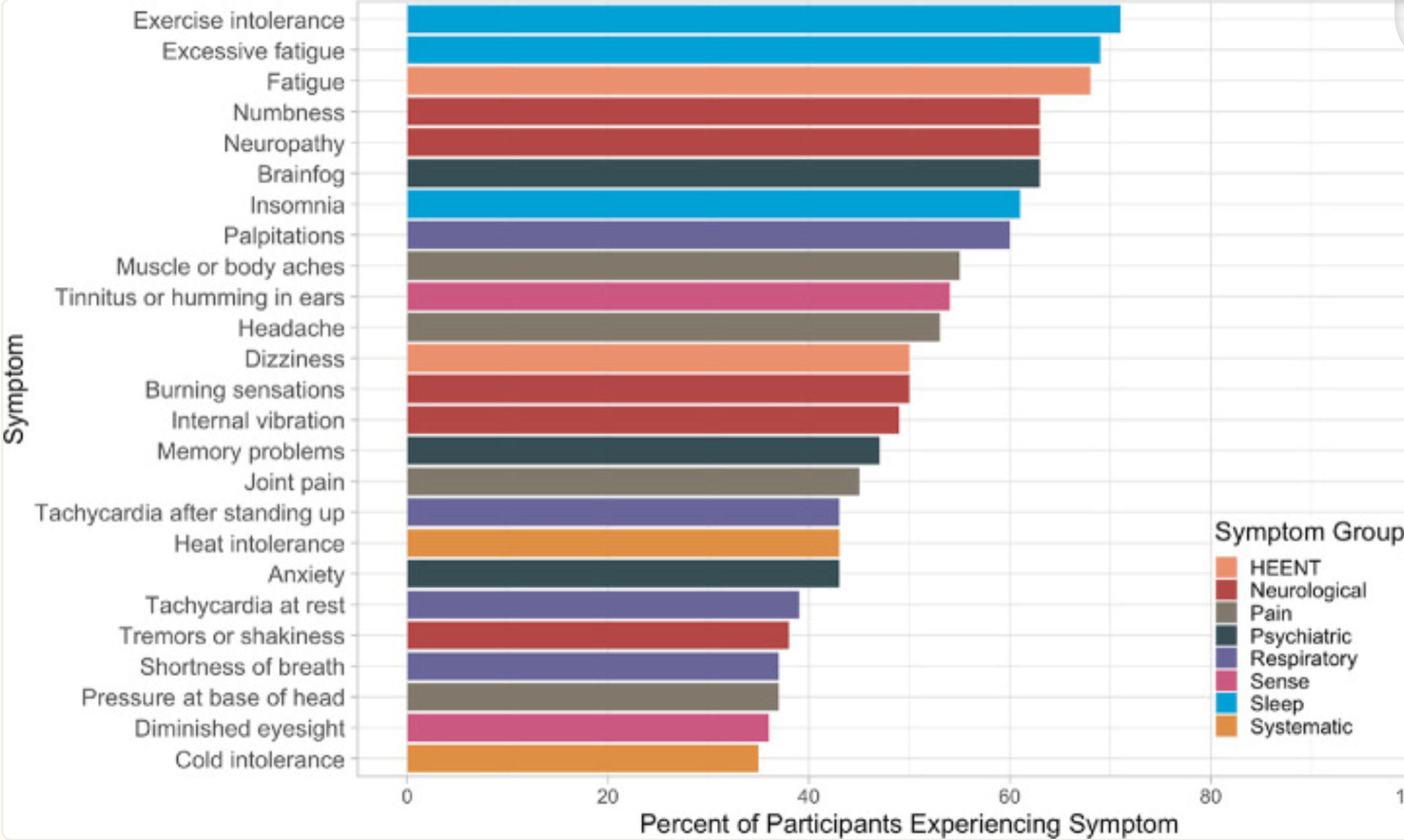
To quote the study:
In conclusion, people reporting PVS after covid-19 vaccination in this study are highly symptomatic, have poor health status, and have tried many treatment strategies without success. As PVS is associated with considerable suffering, there is an urgent need to understand its mechanism to provide prevention, diagnosis, and treatment strategies.
Note: these results were discussed in more detail in this October 2023 online conference (e.g., the mast cell component of the illness). From watching this conference, my impression was that the investigators sincerely want to help the trial participants, but due to the unpleasant implications of their findings, are in a very challenging position (hence why their 2023 pre-print has still not been published).
In their recently pre-published study of 42 post-vaccine syndrome (vaccine injured) participants (and 22 controls) a variety of changes were discovered. These included including lower CD4 cells and elevated TNFα+ and CD8 T cells (which equates to a picture of immune suppression and autoimmunity). Additionally, post-vaccine syndrome (PVS) participants had a tendency for the re-activation of chronic infections and had a chronic persistence of the spike protein.
General Health
Vaccine injured individuals reported lower general health scores, such as lower physical function scores, higher anxiety, depression, fatigue, and pain scores and increased sleep disturbances.

This is important because it demonstrates that vaccine injuries are a real condition with actual health effects (rather than just ‘being in your head’).
Spike Protein Persistence
To my knowledge, this study provides the best demonstration that the COVID vaccine persists for a prolonged period in the body and when present, typically is much higher than in controls.
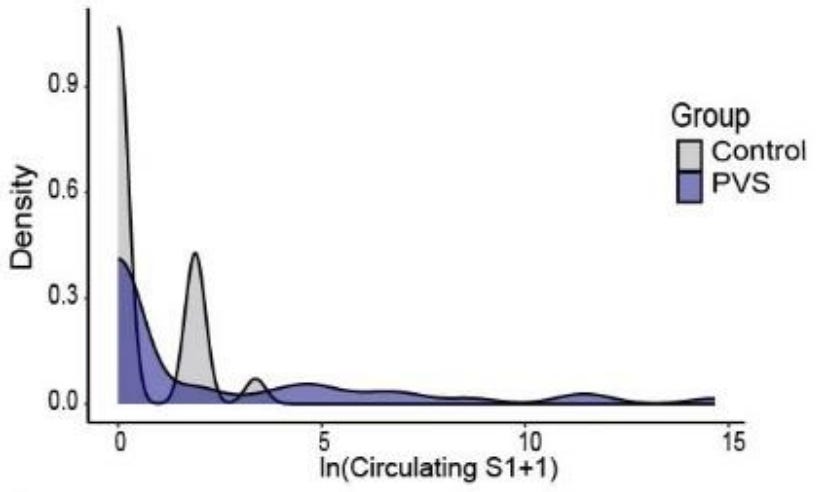
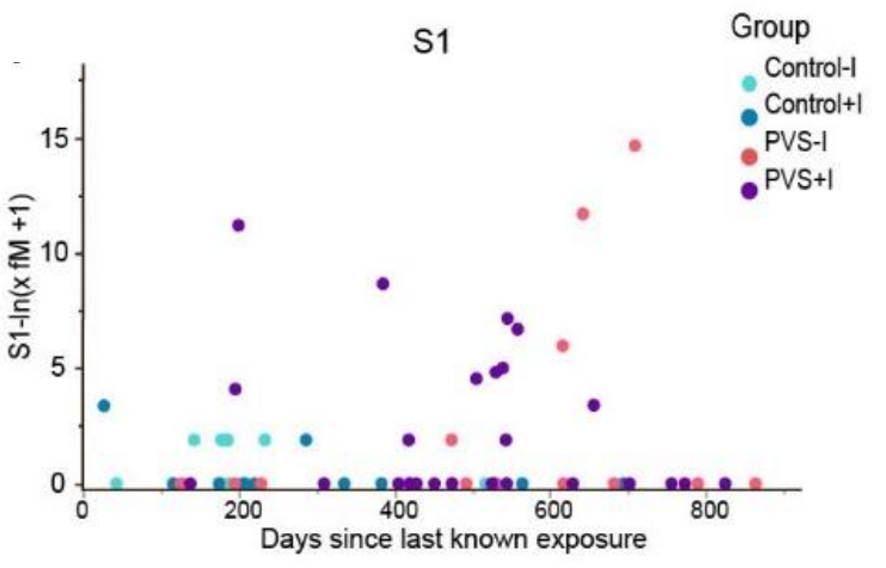

This data collectively shows that:
•The COVID vaccine spike protein can persist for years in the body. The major limitation with each previous study was that spike was still found at the end of the study duration, so it was not possible to know how long it actually persisted. As this study shows, a few months was not long enough to measure the spike protein’s persistence, as in some cases, it lasted for close to two years (were it to be measured again, might last even longer).
•In many cases, COVID spike protein persistence eventually stopped but symptoms continued. Assuming this is correct, that means in many cases the vaccine will eventually be eliminated (which may depend upon the vaccine lot they received), and that not all of the post-vaccine symptoms are a result of persistent spike protein production.
•The persistence of the spike protein without any proof of a natural infection provides strong evidence the vaccine’s spike protein is what’s persisting in the body.
Note: I recently discussed this topic with Dr. Malone (who I consider to be one of the most knowledgeable people in this area). We are both of the opinion that while genomic integration may play a role in spike protein persistence, the more probable explanation is simply that the body cannot break down the mRNA (and possibly the spike proteins) due to how it was modified, leading to the perpetual production of spike proteins. Presently, the data does not exist to quantify the scale of spike protein genomic integration, but with what is currently known (which could change as more data becomes available) cellular production of additional vaccine mRNA is most likely not responsible for the majority of the free spike protein found in the vaccine injured individuals.
Immunologic Suppression and Viral Reactivation
One of the major problems with the COVID vaccine has been that it causes a significant number of people to develop signs of immune suppression, such as continually getting ill with the flu or having a reactivation of a chronic viral infection (e.g., shingles in general along with severe cases of shingles has been strongly linked to vaccination).
Note: less severe versions of this immune suppression have also been observed to follow shedding exposures.
A variety of theories have been put forward to explain why this happens, such as:
•The immune system being locked onto the vaccine antigen, which results in it losing the ability to target other natural antigens (and has been proven to be an issue with many other vaccines as well).
•The vaccine creating an IgG4 class switch, which essentially causes the immune system to no longer fight back against COVID spike proteins.
•The overstimulation of the vaccine overtime causes a suppression of spike protein antibodies (which the study observed). This could either be a result of the vaccine injured patients have an existing inability to develop immunity to the vaccine’s spike protein (as suggested by the January 2023 study) or that the vaccine gradually eliminated the body’s ability to bind to the spike protein, resulting in individuals becoming more vulnerable to the spike protein over time if they happened to have a long-acting vaccine continue to produce spike protein inside them.
•The spike protein collapsing the zeta potential of the body (which as it gets more severe can cause blood clots of increasing sizes). Since many symptoms of infectious illnesses result from the zeta potential collapse they create, those symptoms of illness are magnified when there is already an impaired zeta potential.
•The spike protein directly destroying immune cells (e.g., CD4 cells—something also seen in HIV) and the stem cells that create the immune cells.
Note: these labs were sent to me by one vaccine injured participant in the study.
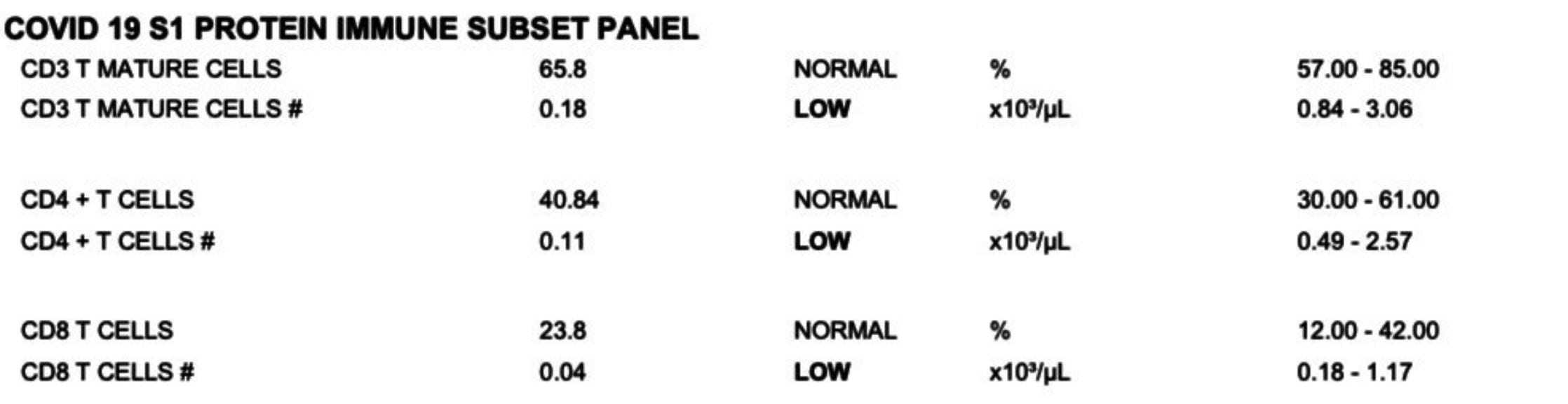
In addition to showing a loss of key immune cells, the study also showed both the CD4 and CD8 cells had signs of being “exhausted,” as changes were observed in them that are known to correlate with those cells partially losing ability to respond to infections due to a chronic over-activation of them (e.g., by persistent vaccine spike protein).
Finally, much in the same way that there were signs of immune dysfunction, the study also observed consistent significant signs of viral reactions in the cohort, most notably with Epstein Barr virus, but also with herpes (however for some reason, shingles was not assessed in this study) and frequently both concurrently. In turn, we have frequently seen EBV be a component of the vaccine injury picture (to the point sometimes it needs to be treated) and frequently also observe an increase in herpes.
Note: one of the best treatments I have found for all three of these viruses is ultraviolet blood irradiation (discussed here). Additionally, DMSO can be quite helpful for shingles and herpes (discussed here).
Additionally, there was also a possible increase in seropositivity to a few other pathogens (e.g., H. Pylori and the parasite Toxocara), which could potentially (but more likely than not doesn’t) explain some of the gastrointestinal issues seen in vaccine injured patients or their response to ivermectin.
Autoimmunity
One of the most common issues associated with the COVID vaccines were autoimmune disorders (detailed here) due to the fact the spike protein had an unusually high overlap with human tissue and because it was designed to express itself on the surface of human cells.
In the Yale study, they observed:
We observed significant increases in IgM reactivities against 65 antigens, IgG 309 reactivity against 1 antigen and IgA reactivities against 39 antigens in PVS compared to controls after multiple testing corrections. Among these antigens, two showed log₂fold change of greater than 2: anti-nucleosome IgM [which is strongly associated with lupus] and anti-AQP4 IgA [which is associated with a rare autoimmune disorder that attacks the central nervous system, particularly optic nerve and spinal cord].
Note: a significant increase in TNF⍺ levels in simulated CD8+ cells (which can often lead to immune dysfunction) and a non-significant increase in CD8+ IFNγ were observed.
I feel these results are important as they validate something many of us have been claiming for four years with the vaccines.
Note: less severe versions of autoimmunity have also been observed to follow shedding exposures.
Conclusion
Throughout my life, as I’ve come to feel that because of the bad trade-offs inherent to many policies or technologies, those behind them (particularly the government) will take an approach akin to trying to pound a square peg through a round hole (as government always defaults to utilizing the force at its disposal to solve the problems it encounters). In contrast, whenever I encounter situations where there really does not seem to be a good way to balance the trade-offs, I take that as a sign I need to consider a completely different approach rather than forcing the one I’ve committed to into working.
With COVID for example, I realized near the start that it would be an exercise in futility to address it with a vaccine—a truth much of the world has now had its eyes opened to. Instead, it was my assessment from the start that the best option would be to quickly develop viable treatments for the illness that could prevent severe complications from it and then allow infected individuals to recover with a strong immunity to the disease (and as we’ve now seen, natural immunity is vastly superior to vaccine immunity for COVID-19).
Unfortunately, rather than heed that approach, our medical apparatus decided to do everything it possibly could to push the vaccine upon us, while simultaneously doing all they could to bury the myriad of effective off-patent treatments developed for COVID-19.
Since the pathway Bill Gates put into place for lucrative accelerated approvals is still in place, I believe this highlights how important it is for us to actually understand how these technologies work and the trade-offs involved with them (which are never disclosed). In turn, it is my sincere belief that if the public had known part of what I presented here, they likely would have never taken the COVID vaccines (or any future mass-produced mRNA vaccine). Similarly, as I’ve tried to illustrate here, contamination and poor production is a systemic problem with vaccines, and were robust independent testing to be conducted (so people actually knew what was in the vaccines they were taking), the demand for them would likely disappear until the industry was forced to clean up its act.
In that light, this study is extremely important as it provides objective proof the vaccine is indeed doing something harmful and abnormal, and that it is occurring long after vaccination. As such, when this topic is broached with a skeptical doctor (or academic) you can now say “did you know a multi-year Yale study recently discovered that the vaccine does chronically damage the immune system of certain recipients and cause a variety of persistent and debilitating symptoms?”
Overall, it is my belief that the most effective way to stop these unsafe products (and those in the pipeline) is not to ban them, but to simply have enough people boycott them that they become financially unsustainable (and due to the new era of information diffusion we are walking into thanks to platforms like 𝕏, it’s actually possible). The FDA and CDC have lost an immense amount of trust because of how flagrantly they lied to the public, and have thus far refused to take any accountability for their actions.
Fortunately, this is something that will likely change once public pressures and financial pressures (e.g., people no longer buying the drugs rubber-stamped by the FDA) force the agency to make genuine amends for its conduct throughout the pandemic and return to good science, which as Secretary RFK Jr. showed in his recent inaugural speech he intends to do for America’s public health agencies.
While COVID-19 was a profound tragedy, because of it we now have an extraordinary opportunity to fix this continually proliferating corruption, and I sincerely thank each of you who has helped to make this moment possible. It’s hard not to understate what a profound shift RFK’s tenure marks for the course of America, and until very recently, I would have considered something like this speech (and the fact I know he intends to follow through on it) to be completely impossible.
An updated index of all the articles published in the Forgotten Side of Medicine (including the DMSO ones) can be viewed here. Additionally, to learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here.









THANK YOU for all of your work over these years - it is truly super-human. I print, read, mark, and learn (better than reading onscreen). It sure feels like a Best-Selling book in the offing =:-)))
What do you expect when you introduce a Messenger RNA molecule that reprograms cellular function. The medicine man is screwing with the blueprint of life and they haven’t got a clue how to control what is transpiring and the harm that is being created. Has to stop now.!