


Why Isn't There a Safe and Effective Treatment for Neck or Back Pain?
Dissecting the dangers of the spinal pain industry

Story at a Glance:
•A lot of money is made in “treating” pain. For this reason, a variety of ineffective or dangerous therapies (e.g., gabapentin) are kept on the market to indefinitely sustain it, while many highly effective therapies that would destroy that market are kept off. Likewise, a remarkable number of parallels exist between the pain industry and the unconscionable profiteering that was seen throughout COVID-19.
•The worst examples are NSAIDs and the opioids. There are numerous instances where their manufacturers knew the drugs had serious safety issues, but covered them up and through the power of bribes (e.g., to the medical journals or the FDA) were able to have these dangerous drugs pushed on America.
•Neck and back pain is a particularly lucrative condition due to the costly spinal surgeries and steroid injections that are routinely used to treat it. Unfortunately, these dangerous treatments often worsen the structural causes of spinal pain, which in turn, like many things in medicine is addressed by more of “treatments” being sold to the patient.
•In this series, we will look at the actual causes of spinal pain so we can understand how to safely, effectively and affordably to treat it.
Surgeries often have a variety of risks that patients do not learn about until after they’ve had the surgery and experienced those complications, which is a huge problem since you can’t “undo” a surgery. For this reason, patients are often advised to seek out a second opinion on if a proposed surgery is really necessary, how likely it will be to benefit them, and what potential risks they face from it.
In turn, spinal surgeries are by far the most common surgery I am consulted about, and likewise something I have become increasingly skeptical of as the years go by. Unfortunately, since spinal surgeries are one of the most profitable areas in medicine, there has been a general reluctance by the medical field to seriously consider if their risks outweigh their benefits or if safer and more effective alternative exist.
What Causes Spinal Pain?
One of the most common reasons patients see their doctors is for spinal pain. Yet, despite trillions having been spent on it (e.g., in 2016, 134.4 billion dollars was spent on neck and low back pain in the USA) the majority of these patients are stuck with chronic pain, and frequently experience significant side effects from the treatments they receive to temporarily alleviate it. Since pain is typically one of the greatest motivations for a patient to seek care, I often wonder if the current state of affairs exists because too many parties cannot afford to lose all the money to be made from pain management.
Note: cures that threaten lucrative markets are frequently suppressed by the medical industry. One of the most well-known examples occurred during COVID-19, where off-patent drugs (e.g., hydroxychloroquine, ivermectin, fluvoxamine and nitazoxanide) were repeatedly demonstrated in clinical to be highly effective in treating the infection, but could never receive an approval (or EUA) for that use. Instead a variety of unsafe and ineffective products (e.g., remdesivir and the mRNA vaccines) were pushed onto the market so a lot of money could be made off of them.
Typically, to manage pain, one of the following can be done:
•Fix what is generating the pain so the pain no longer exists.
•Fix an exacerbating factor which is worsening the existing pain.
•Provide a systemic therapy that reduces pain in the body but does not treat the source of the pain.
In turn, when it comes to spinal pain, I feel each of these is not done correctly.
Spinal Pain Generators:
In my experience, the following things are the most common causes of pain in the spine, particularly in the neck and low back (lumbar) spine:
•Tight muscles—this is one of the most common pain generators. Sadly, I find it is rarely recognized and physical therapists (who would typically be responsible for addressing this) in general tend to focus on strengthening weak muscles rather than stretching or releasing tight muscles.
Note: trigger point therapy, especially when performed with a local anesthetic (e.g., lidocaine), is often extremely helpful for chronically tight muscles, and more importantly, is still utilized by many doctors across the world (which I believe resulted from the remarkable success Janet Travell had in treating President Kennedy). I consider the book on that subject to be one of the most informative things that has been written on the subject of musculoskeletal pain.
•Something being out of place—this requires an adjustment and often correcting the lifestyle habits that create the issues (e.g., too much sitting or staring at a screen). Commonly a patient will have a short leg which distorts the entire spine, and once this is corrected with an adjustment or an appropriately placed foot-lift, the patient will experience a dramatic improvement in their pain (especially you use the arms placed in front of the body to muscle test for the correctly sized foot-lift).
Note: there is significant variability in how spinal manipulation is performed. In some cases, it is remarkably helpful, in some cases it provides a temporary benefit, and in other cases, it can make things worse. For this reason, I have found it is very important to send your patient to the correct practitioner.
•A disc herniation—although this is not the most common cause of spinal pain, it will be discussed throughout the article.
•Ligamentous laxity of the spine—this is often the primary cause of spinal arthritis, spinal muscle tightness, disc bulges and disc herniations.
•Some type of disease process in the spine (e.g., a fractured or weakened bone)—this is the least common cause to come across and can sometimes be treated with appropriate nutritional support (but in other cases requires surgery).
Additionally, I frequently find that:
•Trapped emotions and certain emotional response patterns (e.g., habitual emotional contractions) can significantly exacerbate chronic pain conditions.
Note: Dr. Sarno argued that unresolved emotional trauma triggered “tension myositis” (back pain from tight muscles) which needed to be treated with psychotherapy. His approach helped a lot of people (and thus had a large following), but likewise did not work for many others (including some of my patients). I attribute this both to psychotherapy not always being sufficient to release a trapped emotion and emotions not being the only cause of back pain.
•Chronic inflammatory conditions (e.g., mold toxicity, lyme disease, spike protein injuries) often significantly worsen existing pain patterns.
•Over-activation of the sympathetic (fight or flight) nervous system alongside under-activation of the parasympathetic (rest and relaxation) nervous system exacerbates pain in a manner similar to what is seen from a chronic inflammatory state.
Note: a common effect of unresolved trauma is an over-activation of the fight or flight nervous system.
•Scars (such as those created by surgeries) can frequently generate significant autonomic dysregulation (e.g., too much sympathetic activation) and pain in the body. For example, one patient I saw with a COVID-19 vaccine injury had multiple spinal surgeries (due to a complication from their original neck fusion). These surgeries caused chronic issues for the patient which became dramatically worse (to the point the patient became effectively disabled) after they received the vaccine (severe inflammation at the site of a previous surgery is a common side effect of the COVID vaccines), and their symptoms dramatically improved once the scar was treated with neural therapy.
•In many cases, chronic pain is associated with altered processing of pain in the brain—something which in many cases I suspect is due to a microstroke injuring the thalamus (the part of the brain that dampens pain signals as they reach the brain). In turn, a variety of approaches exist for addressing the brain’s increased sensitivity to pain signals (e.g., IV ketamine therapy is one of the most popular ones now), and when used appropriately, I have seen many of these approaches work wonders for chronic pain patients.
Systemic Treatments of Spinal Pain
Since a variety of different things can cause spinal pain and it can be quite time consuming to entangle what the issue is, physicians typically prefer to either prescribe a pill to treat it, or to refer the patient to someone else. Sadly, each of these leaves much to be desired.
For example, an extremely common story I hear is a patient requesting a pain medication from a doctor (as they have some type of debilitating pain), the doctor refusing to prescribe it (as doctors—who used to be penalized for not prescribing opioids—now get in trouble for prescribing them too frequently) and instead sending the patient to regular physical therapy. This is often quite challenging for the patient to get to (e.g., it’s far away or they don’t have a car), but if the patient is able to make it to PT, typically it doesn’t help them (sometimes it actually dramatically worsens the pain), which in turn either leads to more PT referrals or being sent to a spinal surgeon.
Note: some PTs consistently help their patients, but these PTs are hard to find. I believe this is due to both the training PTs receive not focusing on the most effective ways to treat musculoskeletal pain and the insurance based model of PT prioritizing checking boxes (for insurance reimbursements) rather than helping patients.
When medications are considered, typically four types are utilized: NSAIDs, Tylenol, Gabapentin (or Lyrica) and Opioids.
Unfortunately major issues exist with each of them.
NSAIDs
In the case of NSAIDs (e.g., ibuprofen or naproxen), they often appear to reduce the pain, but since that benefit is temporary and only offers a partial improvement, this leads to patients taking large amounts of the medications (as people will understandably do whatever they can to get out of pain). This is often quite problematic as NSAIDs are toxic, especially at higher dosages.
Many in turn have argued NSAIDs are amongst the most dangerous drugs prescribed in America as:
•NSAIDS are the most common drug class that results in a hospital admission for a drug reaction (typically for heart attacks, bleeding, strokes and kidney failure).
•NSAIDs are well-known for causing kidney damage. For example one large study found NSAIDs increase the risk of kidney disease by 20%, another study found that they increased the risk between 68%-154% (depending on the NSAID), and many studies (e.g., this one) have found individuals with chronic kidney disease (CKD) are typically long-term NSAID users, with the likelihood of NSAID use increasing with the severity of CKD. For this reason, kidney doctors (nephrologists) often order their patients to discontinue NSAID use, and non-nephrologists rarely question this decision.
Note: While NSAID kidney damage is a huge issue, I was unable to find a good estimate on how many people died as a result of this side effect since CKD is a progressive disease rather than one that causes sudden deaths (the closest was a study that found NSAIDs, depending on the type, increased the risk of someone with CKD then dying by 36%-61%—but this does not account for all the people who develop CKD from NSAIDs).
•NSAIDs are well known for causing heart disease (and in some cases strokes). The most infamous examples of this were Merck’s Vioxx and Pfizer’s Celebrex, both of which were NSAIDs designed to cause less gastric bleeding—which unfortunately also made them more likely to cause heart attacks and strokes. Since the drugs made a lot of money (as pain management is highly lucrative), Pfizer and Merck covered this up. Eventually the truth came out and Vioxx was withdrawn from the market (although recently the industry has started working to bring it back). When it was all said and done, just from heart attacks and strokes, Vioxx was estimated to have killed 120,000 people, while Celebrex (which was never taken off the market) killed 75,000.
Note: the year Vioxx was pulled (2004), Merck’s CEO received a $36 million bonus. Following losing over 5 billion dollars in lawsuits, Merck then pivoted to creating the disastrous (but incredibly profitable) HPV vaccine. In turn, much of the playbook Merck developed to push its unneeded and incredibly dangerous vaccine onto the market was then copied throughout the mRNA vaccine roll-out (e.g, very similar fraud occurred during the clinical trials).
Sadly, Vioxx and Celebrex are not the only NSAIDs that kill. For example, in a study of 83,677 patients who had had a single heart attack (making them be at high risk of another one), taking an NSAID was found to increase the risk of a second heart attack or death by approximately 50% (with the exact risk depending on the NSAID—diclofenac increased the risk by 326%). Similarly another study of 107,092 patients who were hospitalized for heart failure (and then recovered enough to be discharged) found that taking an NSAID increased their subsequent risk of dying by 22%-108% (depending on the NSAID), often due to NSAID associated heart failure or a heart attack. The largest study I found that attempted to assess the risk of an NSAID causing a heart attack in the general population found taking NSAIDs for any period of time increased the risk of a heart attack by 24%-58%.
•NSAIDs are well known for causing gastric bleeding, something which is often fatal. In 1999, it was estimated that over 16,000 Americans were killed as a result of NSAID gastric bleeds (along with many more being hospitalized but surviving)—so it is likely between 10,000-20,000 Americans are killed each year from this complication.
Note: NSAIDs also damage the small intestine, but since we can rarely peek inside there (whereas the stomach is easy to see with a scope), and damage there rarely results in a fatal bleed (as there is not abundant stomach acid), this complication of NSAIDs is often goes unrecognized. For decades, there has been a well-known link between NSAIDs and intestinal webs (strictures that prevent the passage of food through the small intestines) while more recently advances in diagnostic technology have shown that 50% of chronic NSAID users have damage there (which is termed “small bowel enteropathy”). This often leads to chronic health issues, because once the mucosal lining of the small intestine becomes damaged, pathogenic substances (e.g., plant lectins, undigested protein, or inflammatory components of bacteria) can easily pass from there into the bloodstream—and many have argued this leakage is the root cause of chronic illness in the Western World.
•NSAIDs cause a variety of other severe health issues as well, best illustrated by them being one of the most common classes of drugs to be pulled from the market (e.g., multiple NSAIDs were withdrawn for causing severe liver damage). For example to quote Peter Gøtzsche
Several drugs that were so kindly treated by the FDA were later withdrawn from the market because of their toxicity despite claims to the contrary, e.g. ‘Excellent gastrointestinal tolerance’ (benoxaprofen), ‘superior tolerance’ (indoprofen), ‘proven gastrointestinal safety’ (rofecoxib), ‘hurts the pain not the patient’ (ketorolac) and ‘least possible side effect profile’ (tolmetin).
•A variety of less obvious side effects also occur. For example, NSAIDs impair ligaments repairing themselves after an injury, so since they are frequently given after things like an ankle sprain, a chronic weakness forms in the area which some evidence suggests predisposes it to further injuries.
Fortunately, the dangers of NSAIDs at last are being gradually acknowledged by healthcare authorities around the world (e.g., the FDA has gradually strengthened its warnings that NSAIDs cause heart attacks and deaths). Nonetheless, they are still given out like candy for every ailment imaginable, doctors rarely withdraw patients from them, and since many can be purchased without a prescriptions, overdoses of them are inevitable.
Peter Gøtzsche has provided one of the best summaries of this tragic situation in his book Deadly Medicine and Organized Crimes. Amongst other things he noted that:
•Trials alleging the benefit of NSAIDs are frequently intentionally deceptive and frequently create the illusion of a benefit where none exists. What this means is that many patients ruin their lives with drugs that did almost nothing for them in the first place.
•With Vioxx, Merck knew early on the drug would cause fatal heart attacks, but chose to doctor their studies so this was not visible to the public. To hide the heart attacks, Merck did not disclose many that occurred its trial, and midway through changed the trial protocol so the heart attacks would be monitored for over a much shorter duration (whereas the benefits Merck wanted to show like reduced gastric bleeds were monitored for a much longer time).
This was clearly fraudulent, but nonetheless given a pass by the FDA—the data the FDA received showed Vioxx doubled the risk of a heart attack, but at the time of approval the FDA ultimately stated that it lacked ‘complete certainty’ that Vioxx increased cardiovascular risk. Finally, as you might imagine, once Vioxx was approved Merck began illegally pushing for it to be used to treat every illnesses under the sun, which resulted in many people who had no reason to take their drug being killed by it.
Note: Dr. Mercola was one of the earliest people to recognize the obvious risks of Vioxx, but despite his large following and how clear the risks were, his warning went unheeded. I share this example to illustrate just how resistant the medical industry is to considering science which gets in the way of its bottom line.
•Likewise, when the New England Journal of Medicine received Vioxx’s pivotal study (which was clearly fraudulent), rather than address this, they chose to publish it (which in turn allowed Merck to market Vioxx to America since the NEJM had endorsed it). Then, despite more and more evidence accumulating that Merck’s NEJM paper was fraudulent, NEJM refused to retract the article or issue a correction, and it was only 6 years later when Vioxx was withdrawn and lawsuits were working their way through the legal system that NEJM chose to issue a “statement of concern.” It should hence come as no surprise that NEJM received a lot of money from Merck—929,400 reprints of the article were purchased (this is a common way Pharma pays off journals) netting NEJM approximately $800,000, and in that year NEJM’s owner made $88 million.
Note: it is likely many other payments were also made to NEJM or to its editors (which is also a common industry practice), but unfortunately, that financial information is not available to the public.
The story of Vioxx is important because an almost identical thing happened with the Pfizer vaccine. Like Vioxx, it was clear from the start the vaccine would be dangerous and that the vaccine trials were doctored to conceal that risk. Yet, NEJM and the FDA ignored those issues and instead published a glamorous appraisal of the new product, and even after a deluge of evidence showing that Pfizer’s trial was fraudulent (including numerous whistleblower testimonies), neither NEJM or the FDA did anything about it (rather they doubled-down on the value of the vaccines).
Finally, now that the market for the mRNA vaccines is starting to sour (e.g., only 2% of America elected to receive the most recent booster), admissions are gradually appearing indicating in the medical literature that the vaccines are in fact dangerous and frequently cause heart damage. This is quite similar to how Vioxx is now considered to be one of the worst drug disasters in history, but until it was pulled from the market (and no more money could be made from it) it was very hard to discuss its toxicity.
It is hence regrettable that we did not listen to the warnings of NEJM’s editor-in-chief in 2004 that the medical journals are corrupt and cannot be trusted. Had we done so, there might have been more skepticism towards NEJM’s infamous trial that extolled the safety and efficacy Pfizer’s vaccine and was embraced with a cult-like devotion by the entire medical community.
Tylenol
As Tylenol is one of the only other over-the-counter pain killers, it is frequently used in a very similar manner to NSAIDs, and overall is a safer option (but still typically not sufficient to alleviate significant pain). Unfortunately, the drug has two major issues.
The first is that one of its potential metabolites is quite toxic to the liver. At lower doses, minimal amounts of this metabolite are produced (and that which does is neutralized by the liver) but at higher doses, much more is and it frequently overwhelms the livers ability to safely metabolize it (via glutathione), which ultimately leads to significant liver damage. Since people often take excessive doses of Tylenol (e.g., to reduce pain), liver failure is a far too common side of the drug and presently 56,000 emergency department visits, 2,600 hospitalizations, and 500 deaths result each year in the USA as a result of Tylenol toxicity.
Secondly, Tylenol works by suppressing fevers (which is another common reason why people take it). Since the body uses fevers to combat illnesses, suppressing them can lengthen the duration and severity of an infection. This was something I saw numerous times during COVID-19, and what many parents of vaccine-injured autistic children observed, as their child’s autism began after Tylenol was given to suppress the extremely uncomfortable high fever their child developed after vaccination.
Gabapentin
One of the most common tactics used by the drug industry is to get a medication approved for one condition where it’s relatively easy to prove the drug does something, and once it gets licensed, groom doctors (e.g., with bribes) to use it for a variety of other conditions where it doesn’t work very well and could not have won an FDA approval. While this is illegal and pharmaceutical companies frequently get fined millions if not billions of dollars for doing it, the practice makes so much money that they keep on doing it anyway.
Gabapentin (Neurontin) was originally approved as a drug to treat epilepsy (a relatively small market), so once it was approved, Pfizer started aggressively promoting it to treat a variety of other conditions. This was done to such an egregious degree that the federal government decided to pursue charges against Pfizer, which eventually resulted in almost a billion dollars in fines.
One of those off-label uses was neuropathic pain, and since physicians have limited options for tackling pain (especially since the government went after the opioids), gabapentin gradually became one of the most commonly prescribed pain medications. My own experience has been that with certain types of pain (e.g., neuropathies) it often works quite well, but for the majority of pain conditions, it does almost nothing.
Note: pregablin (Lyrica), and mirogablin (which is only approved in Japan) are very similar to gabapentin and often used in place of it.
While gabapentin is not as toxic as the NSAIDs, it does have side effects (sleepiness, lethargy, dizziness and impaired cognition are the most common, while allergic reactions, respiratory depression and allergic reactions are also known to occur). In turn, many (including numerous people I know) have had fairly bad reactions to gabapentin. For this reason, I feel it should only be given to patients who clearly benefit from it—which is a rule many other doctors do not follow as patients are often kept on it for years despite the drug not doing anything.
Note: another major problem with gabapentin is that can sometimes be quite addictive.
Opioids
Opioids are the most effective pain killers on the market and simultaneously have a lot of issues—which has led to there being a lot of mix messages within the medical profession on how they should be used.
Note: Despite this, I know of numerous cases where an opioid could not heal pain that a more natural systemic pain-killer could.
One of the very first medications used in Western medicine was opium and likewise, one of the first drugs which caused immense social damage from the addiction it created (e.g., China unsuccessfully went to war with England to stop English merchants from flooding the country with opium). Since the opioids are extremely effective, as time moved forward, other more potent variants of opium were also discovered and many of the same mistakes were repeated. For example, after heroin was discovered in the 1874, it was initially viewed as a wonder drug, then later discovered to be quite addictive and eventually was outlawed.
In 1991, Purdue Pharma was incorporated and immediately began focusing on the opioid market (which previous iterations of the company had experience in) and before long, had created its own proprietary opioid—OxyContin. Purdue concluded that if it could market its drug as being both safe (not addictive) and effective, this represented an incredibly lucrative market.
To accomplish this, rather than producing the necessary clinical trial data to show their drug was safe, in 1995, Purdue decided to bribe the official in charge of the FDA’s department which managed painkillers and addictive drugs as he had the final say on approving OxyContin. That corrupt official then privately worked with Purdue (which was illegal) to put together a review of OxyContin, which included the phase "Delayed absorption, as provided by OxyContin tablets, is believed to reduce the abuse liability of a drug," a line which was used by Purdue to market (the incredibly addictive) OxyContin to everyone.
Shortly after its approval, that official left the FDA, and before long had a lucrative job with Purdue. Understandably, he denied all of this (including the private meetings), but it all eventually came out in court after Purdue’s records were scrutinized by prosecutors. Nonetheless, he never was criminally prosecuted for his conduct at the FDA or for lying about it under oath.
Note: it is almost impossible at the FDA to get convicted for bribery (which I believe is due to having a culture that has gradually normalized corruption). Purdue Pharma has been cast as a villain due to how incredibly damaging the opioid epidemic it created has been to the country (and the many investigation which thus followed), but the reality is that their actions mirrored what’s been done by many other companies.
For example, Trump’s second FDA commissioner is now a board member for Pfizer, while his final commissioner went behind Trump’s back to sabotage safe and effective treatments for COVID-19 (which killed a lot of people and created the “need” for the emergency COVID-19 vaccines) and then was hired as an executive for Moderna’s parent company. Similarly, Biden’s FDA commissioner (who also served under Obama), has been repeated criticized for being in bed with the pharmaceutical industry, and during his tenure has pushed through highly controversial (but lucrative) medications and was a keynote speaker at a major industry conferences promoting those medications to investors.
A common tactic used by industry is to pay off a third party to promote its message (e.g., a polluter paying off a group that on the basis of its name appears to advocate for protecting the environment). This tactic is commonly used by the pharmaceutical industry to promote its products and Purdue did this through the American Pain Society, which in 1995 (coinciding with OxyContin’s approval) launched its “Pain is the 5th Vital Sign” campaign. This campaign called for all suspected pain to be aggressively treated, and many others (e.g., the VA and state medical boards) took it up, before long leaving many doctors in a position of being open to disciplinary action if they did not widely distribute OxyContin.
Since everyone pushed Purdue’s products and they were incredibly addictive (e.g., you get severe withdrawals once you stop), there was an immense and sustained demand for them, leading to Purdue ultimately making over 30 billion dollars in sales. However, they simultaneously unleashed a devastating opioid epidemic on the country (e.g., hundreds of thousands of people have died from overdoses), which eventually led to the government completely reversing its position and penalizing doctors for prescribing opioids unless it was absolutely necessary.
Because of this, doctors are thus reluctant to prescribe opioids (instead making patients do other things like gabapentin or repeated PT), and a common theme doctors in practice encounter are patients with severe pain who cannot get the opioids they need to manage their pain. Understandably, this is particularly frustrating for chronic pain patients who had previously been able to receive opioids for their pain.
While opioids do work quite well for managing pain (at least initially), in addition to their high likelihood of creating severe addiction, I feel there are two major issues with the drugs.
•First, they often disassociate people from their bodies, which leads to a lack of interest in being alive and connected to life (similarly, many have observed being on an opioid appears to interfere with the spiritual transition during the dying process).
•Second, they drain the vitality of the body, and I have seen many cases of this happening to long-term prescription and illicit opioid users (e.g., this is well known to happen in heroin addicts and it eventually killed my friend’s spouse after they had been placed on OxyContin for ten years following untreated back pain from a car accident). I suspect this side effect is largely due to exogenous opioids reducing endorphin production in the body (since miraculous improvement in vitality are often observed when an opioid blocker is administered which instead increases endorphin production in the body).
In short, we do not have any medications for treating pain throughout the body which are both safe and effective. Given that quite a few safe and effective pain killers do exist (most of which cannot be commercialized), this has led me to suspect they’ve intentionally been kept off the market so that the lucrative pain market can be sustained indefinitely, as the only way new (but less than satisfactory) pain products can come to market is if nothing satisfactory is available in the first place.
Note: This situation sadly has also happened many other areas of medicine. For example, the FDA spearheaded a baseless fear-mongering campaign ivermectin and hydroxychloroquine (as all of the unsafe but lucrative COVID-19 products were given emergency approvals due to “no effective treatment” for COVID-19 existing). Similarly, after the one effective treatment for insomnia went off-patent, a huge (but baseless) media campaign was launched against it, leading to it becoming almost impossible to obtain and patients instead being stuck with a variety of harmful and often ineffective sleep medications—which has been quite consequential for the country as poor sleep a root cause of many chronic illnesses.
Disc Herniations
One of the most common causes of spinal pain is a disc herniation, something which occurs due to the outer capsule of a vertebral disc weakening and hence allowing the discs contents to protrude into the area behind the disc. This in turn causes pain because spinal nerves lie immediately behind the disc, and they can become compressed by the herniated disc (along with being irritated in a less severe manner by a bulging but not herniated disc).

Before we go any further, I want to note that medicine is biased to believe that something must be seen for it to be “real.” In addition to this causing important things that are hard to see being violently rejected by the scientific field, it also causes science to quickly believe things which can be seen but are not consequential. For instance, MRI abnormalities (e.g., a vertebral disc bulge or disc degeneration) are used to assess back pain, determine its progression, and decide what treatments should be given (e.g., spinal surgery or an opioid), because the problem is self-evident on an MRI. Yet, when this is studied, it’s found that:
•Patients with abnormal MRIs often do not have back pain, nor do they develop in it the future.
•Patient’s with back pain frequently have normal MRIs and there is no correlation between MRI findings and the severity of back pain.
Note: one common practice in the illicit drug market is to claim to have severe pain to obtain an opioid prescription that can be resold. This requires faking an MRI to convince the prescribing doctor, which is accomplished by positioning the body to create a temporary disc abnormality at the time the MRI is taken.
My own experience has likewise mirrored the results of those studies, and I find spinal pain is often due to something besides what the MRI identifies (e.g., tight muscles).
Note: in many cases, a disc bulge is a symptom of ligamentous instability, and ligamentous instability will cause pain independent of a bulging disc (which means an incorrect correlation is assumed between disc abnormalities and spinal pain).
I thus believe that the MRIs only become significant if there are also clear clinical signs a nerve is being compressed (e.g., a weakness or loss of sensation in the area affected by a spinal nerve). Similarly, the existing evidence on spinal surgery shows that it typically creates the best outcomes for patients who have both pain and signs of a spinal nerve impingement (which is termed a “radiculopathy.”
Note: in some patients, we do find that reversing disc degeneration dramatically improves spinal pain—however it’s important to note that this does not apply to every patient with a disc that looks abnormal.
Managing Disc Herniations
Classically disc herniations are thought to be due to either age-related degeneration of the vertebral disc, connective tissue disorders (which weaken the disc), significant trauma, or a combination of the previous (e.g., trauma happening to a weakened disc). Unfortunately, while these causes are recognized, they are rarely thought about before (often harmful) treatment is initiated for the disc.
Note: I believe the loss of zeta potential and liquid crystalline water that occurs with aging plays a major role in disc degeneration (as the inside of the disc is a liquid crystalline gel). Similarly, because the discs have no inherent circulation, they depend upon continual compression and decompression to bring nutrients into the disc (and waste products out), so as we become more sedentary and reduce that circulation (e.g., worsened by the spine frequently becomes less-flexible with age), the discs also weaken.
Similarly, disc degeneration is often a consequence of the cell danger response (CDR) activating in the disc (which then often spreads to the surrounding vertebrae). For this reason, local CDR treatments frequently (such as those which reduce TNF-α, a cytokine intimately associated with disc degeneration) can frequently reverse the process and restore the health of the spine.
Unfortunately, while a variety of treatments are used to manage disc herniations, they often do not consider a simple but critically important principle of the spine:
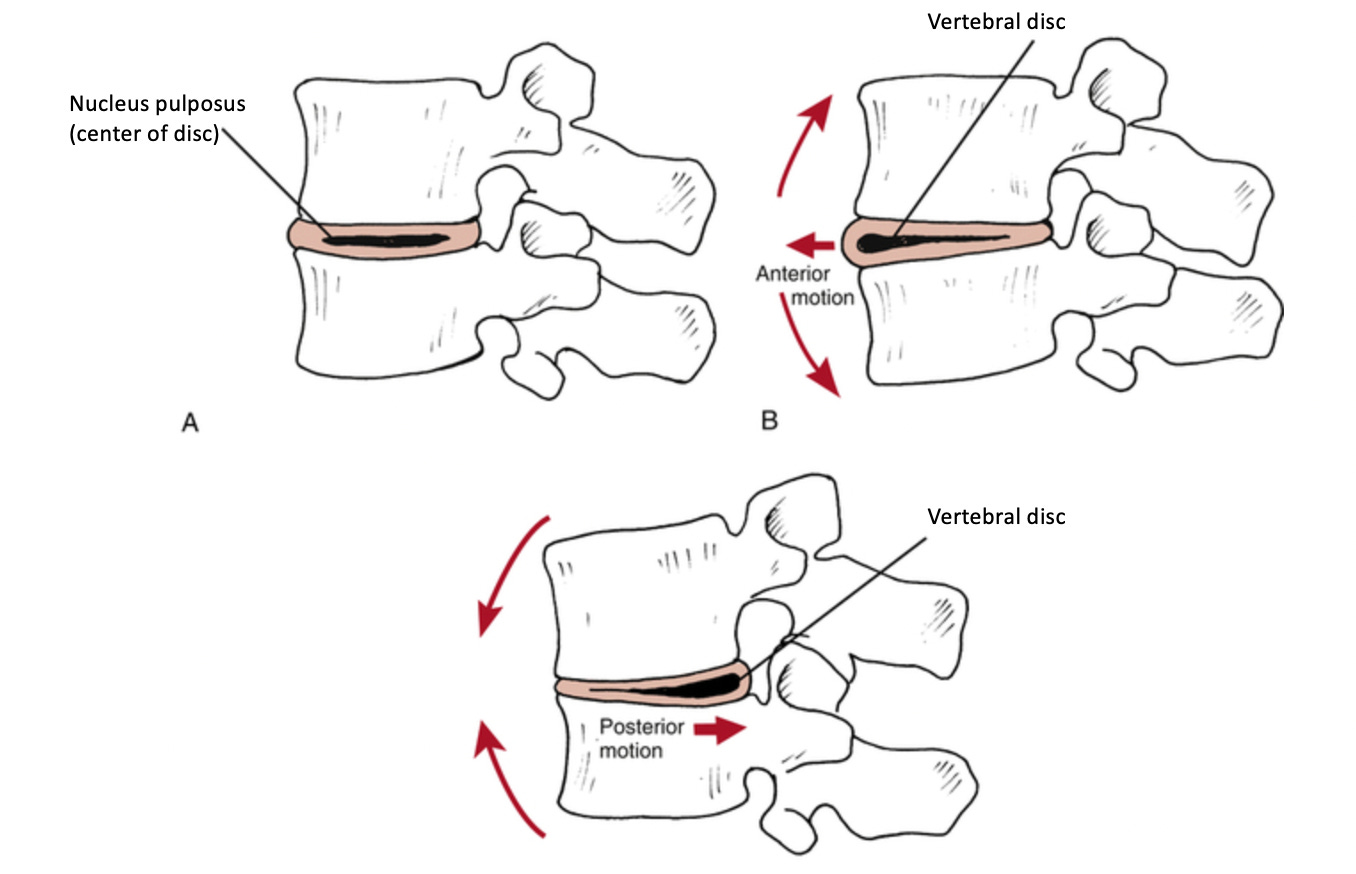
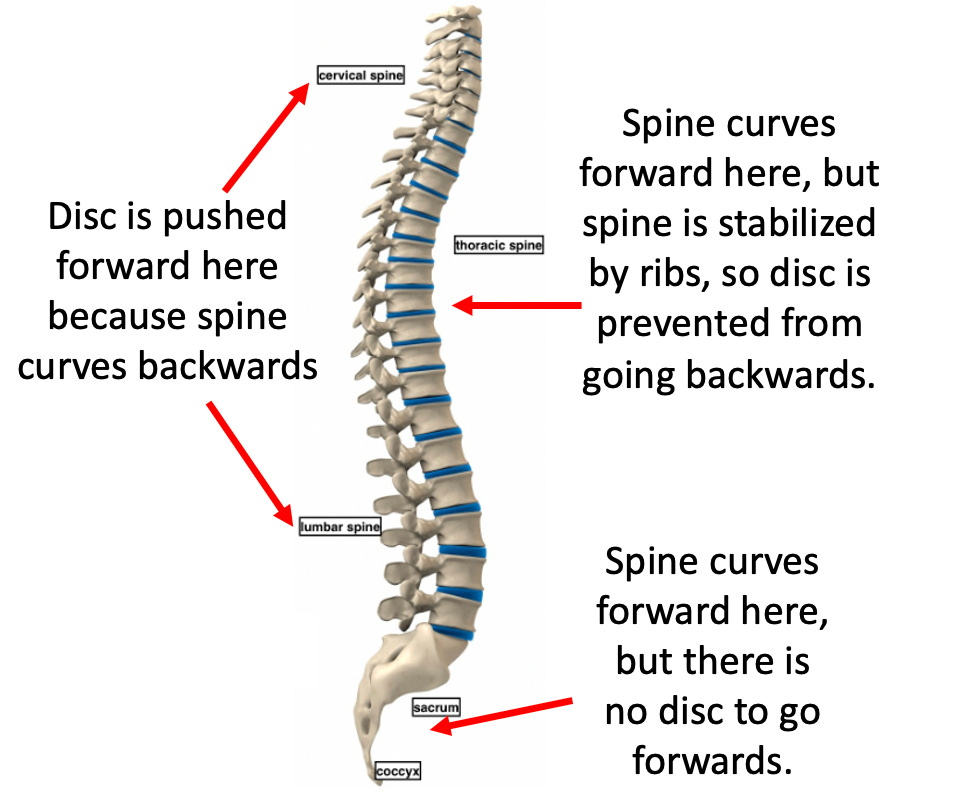
When you bend backwards, the disc is pushed forwards, while when you bend forwards, the disc is pushed backwards and can compress the nerves behind it.
Spinal Curvature
From an engineering standpoint, the spine is a marvelous structure as it both supports the body while also providing a significant degree of mobility. For example, because the spine is curved, its absorbs that load by curving more, and then dissipates it by having the elasticity of its ligaments (and discs) restore the spine’s original curvature.
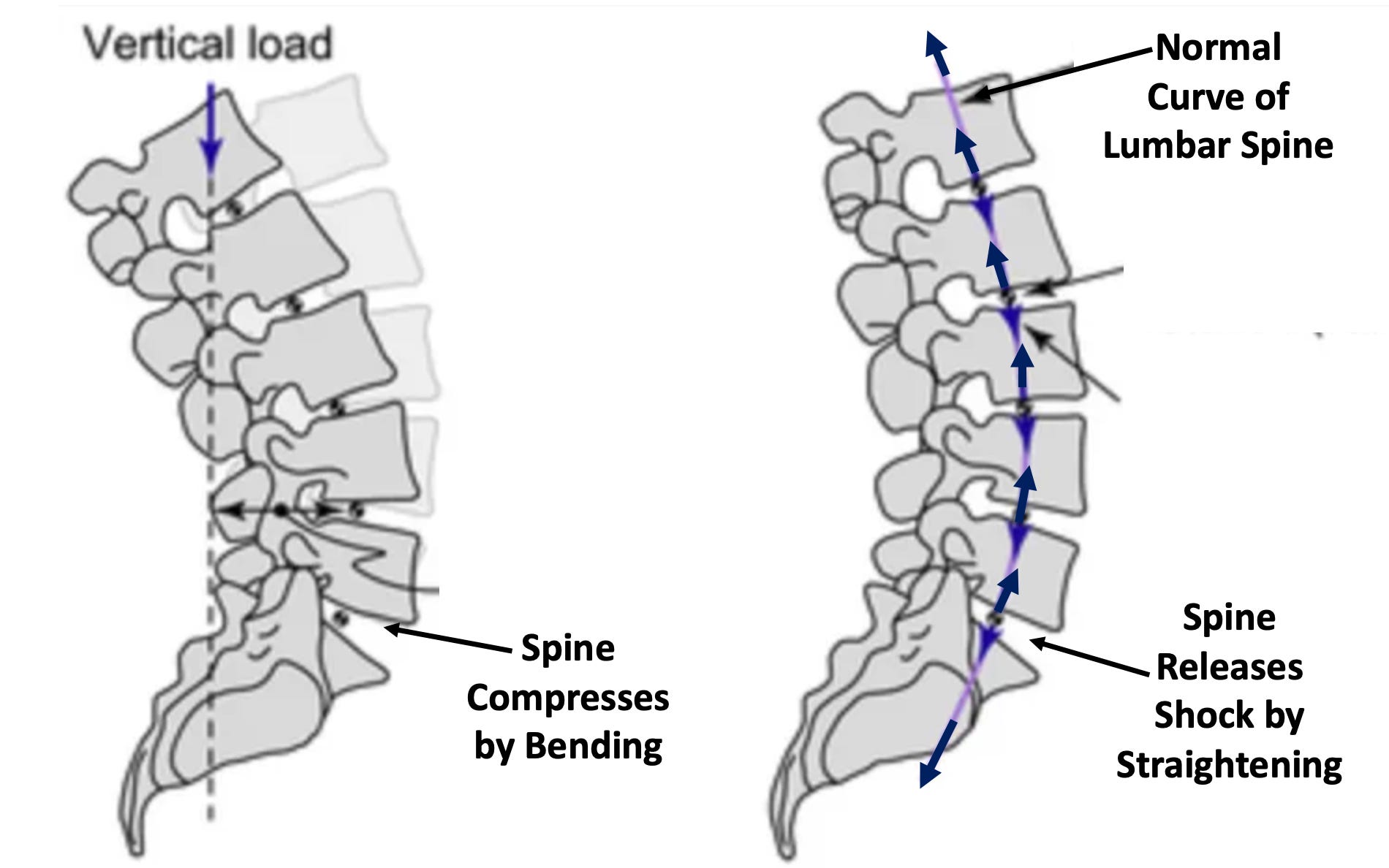
Because of this natural shock absorber, we can handle large numbers of vertical shocks (e.g., those created by running). However, for this shock absorber to work, the spine needs to have curves going in alternating directions. Fortunately, nature also solved the problem of those forward curves pushing the discs backwards.
Unfortunately, this healthy curvature is frequently disrupted in modern life.
Upper Cross Syndrome
One of the most common postural issues in modern life is a hunching forward in the spine (termed kyphosis) a condition which typically worsens with age.
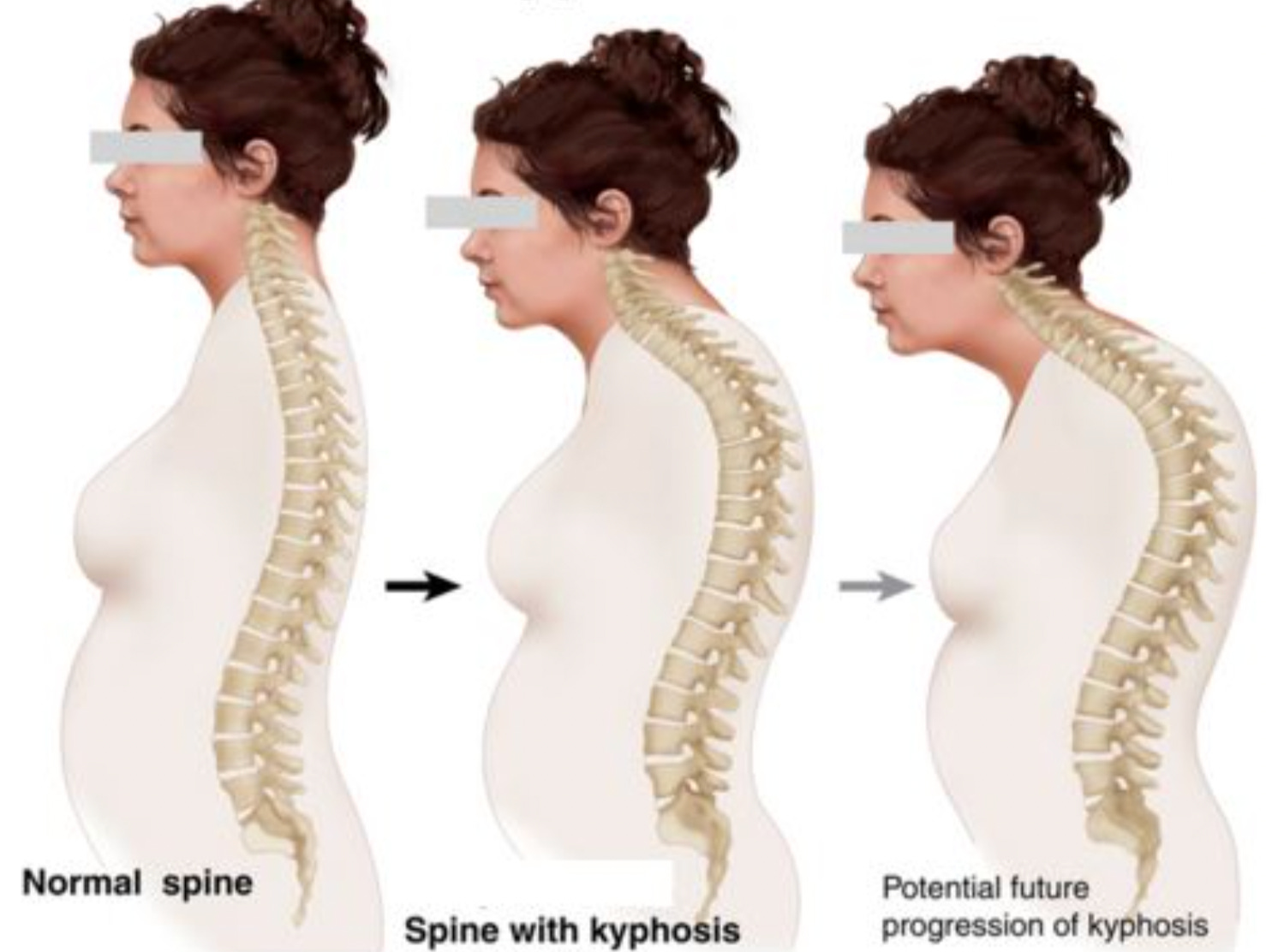
This disruption to the normal curvature of the middle of the spine also affects the rest of it and amongst other things frequently leads to the cervical spine losing its backward curvature.
A variety of things can cause this happen, many of which are a consequence of our current lifestyle which encourages hunching forward in front of a computer:
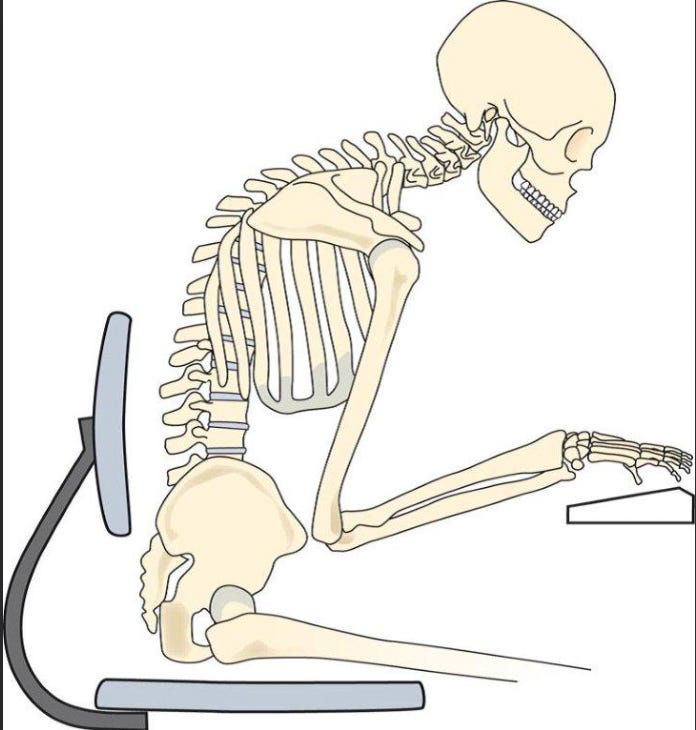
Typically, a few things happen simultaneously:
•The ligaments on the back of the spine (which would normally prevent an excessive forward curvature) weaken.
Note: this also reduces the spine’s ability to function as a shock absorber for vertical force.
•The ligaments on the front of the spine tighten.
•The muscles on the back of the spine (which also help to pull the spine backwards) like the rhomboids weaken.
•The muscles on the front of the body which increase the curvature of the thoracic spine (e.g., the pectoralis minor) tighten.
All of which combine to make it increasingly difficult to straighten the spine.
In concert these changes are known as upper cross syndrome, and when diagnosed, it is typically treated by strengthening the back muscles (e.g., by rowing) and stretching the muscles on the front. In my own practice, I find that often the most helpful thing for patients to do is to simply encourage them roll up a towel and lie with it across the most tight portion of their back for a few minutes each day.

Note: I do not like using foam rollers because I find they are often too much for the patient, and as a result they briefly use them and then stop because of the discomfort. Furthermore, as upper cross syndrome worsens, patients often cannot just lie straight on their backs, and in time, even handle sleeping without a large pillow behind their head (at which point upper cross syndrome is much harder to treat and normal sleep function—something absolutely vital for health—begins to become impaired). For this reason, I try to encourage patients to address upper cross syndrome as soon as I notice it starting.
Typically, the upper cross syndrome diagnosis focuses on the muscular imbalance. However, as time has moved forward, I’ve come to believe a weakness of the ligaments on the back of the spine is actually the greatest issue and what is the most important to focus on when treating it.
Joint Stability
Two of the most common causes of arthritis and joint pain are:
•A poor exchange of fluids in the joint (because like the vertebral discs they do not have an intrinsic circulation).
Note: I believe this is a key reason why an impaired zeta potential (and the Chinese medicine equivalent—blood stasis) is often seen in conjunction with arthritis.
•Unbalanced forces pushing the joint out of its normal range of motion and gradually wearing the joint down. Typically, ligaments counteract these unbalanced forces, but as the ligaments weaken the instability within the joint will increase.
A variety of things can cause the ligaments to weaken including:
•A few key nutritional deficiencies.
•Acute or chronic unbalanced forces on a ligament (which are more likely to create problems in already weakened ligaments).
•Chronic inflammatory states, a chronically activated Cell Danger Response (which causes the ligaments to not rebuild themselves and thus gradually decay), pharmaceutical toxicity (fluroquinolones are well-known from doing this) or connective tissue diseases like Ehlers-Danlos Syndrome (which is well-known for predisposing patients to drug and vaccine injuries along with being pushed to receive spinal surgeries).
Additionally, in many cases, chronically weakened ligaments will also trigger muscle spasms in the body (as the muscles reflexively tighten to stabilize the body). For this reason, it is often challenging to know if a tight muscle or a weak ligament is the root cause of back pain, but you can often tell once each is treated.
Local Treatments of Spinal Pain
One of the most common treatments given for both disc herniations and general pain in the spine are steroids—something I am not a fan of because:
•Steroids have a wide variety of side effects (e.g., I know quite a few people who developed a permanent illness from a course of oral steroids). Nonetheless, I have found brief courses of oral steroids can be very helpful for abrupt symptomatic disc herniations.
•Steroids weaken the ligaments of the body.
•Most of the injected steroids are not water soluble. Because of this they will often persist for a lengthy period in the injection site—something I learned of from an orthopedic colleague who showed me arthroscopic footage (via a video feed from inside a live joint) where the steroid could be seen coating the joint.
Note: my colleagues who are aware of this issue prefer to use Decadron as it is a water soluble steroid.
Let’s quickly look at the ligaments of the spine:
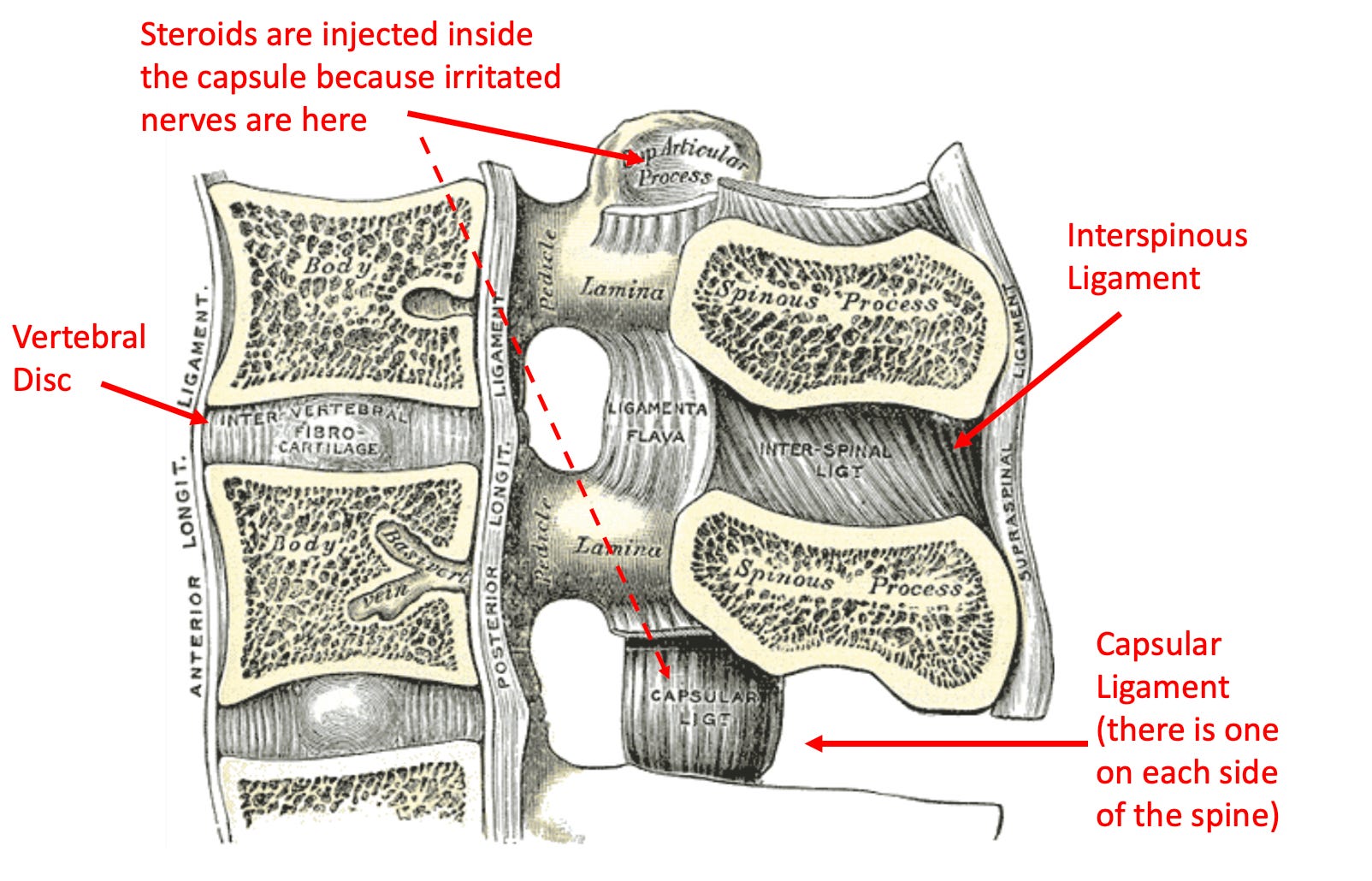
When looking at these ligaments, it’s important to understand that there are two major functions of the ligaments in the back of the spine. The first is that they stabilize the vertebrae, and the second is that they pull the spine backwards.
Thus, we again see an all too familiar pattern of medicine—the “cure” for a disease (in this case a steroid injection) creates the disease it is supposed to prevent (as steroids weaken those critical ligaments of the spine).
Note: this is similar to how low stomach acid creates acid reflux, so by putting a patient on acid blockers, in addition to a variety of health problems being created from deficient stomach acid, patients also become permanently hooked to those drugs.
Fortunately, the medical field is starting to become aware of this issue and the existing guidelines now say to avoid more than 3-4 steroid injections per year, as doing more than that can “potentially weaken ligaments or bones in the area.” Unfortunately, they are still not focusing on ways to restore ligamentous integrity.
Note: in addition to steroid injections, another popular option are nerve ablations, where a needle inserted into a nerve which is believed to be causing pain, and then running electricity through the needle to destroy the nerve. This approach “works” but since the peripheral nerves regenerate, it typically needs to be repeated within a year.
Spinal Refraction
Anytime a wave travels through something, if the density of the medium the wave travels through changes, the wave will also change (through a process known as refraction), with part of the wave being reflected at that transition, part of it being absorbed at the transition, and part of it continuing on through the new medium. For example, imagine what happens when a wave of water crashes into a wall—the water bounces back, it damages the wall, and the new shockwave propagates through the wall.
In the case of the spine, due to its alternating structure, it continually transitions between flexible mediums and inflexible mediums as the lumbar and cervical spine are much less constrained than their adjacent structures (the tail bone, rib cage and cranium). Because of this, any time a wave travels through the spine (e.g., your body weight falling into your foot and then bouncing up your body each time you take a step), it has to undergo a refraction at each of the transition zones.
As a result, many find the most common sites of musculoskeletal pain in the spine are at the following junctions:
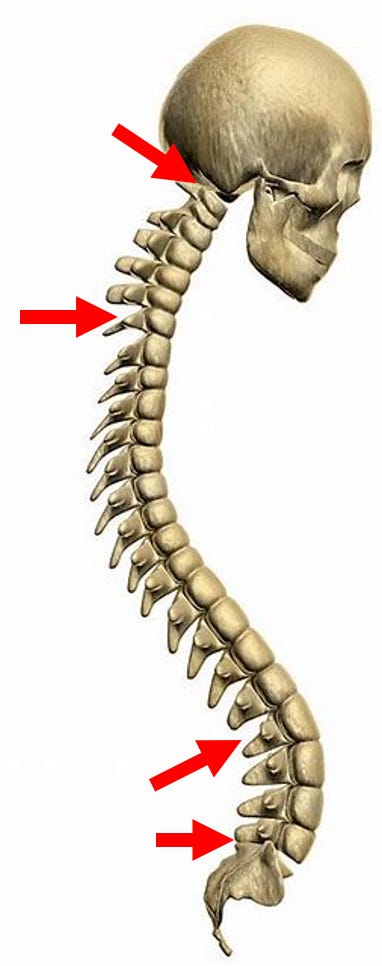
Typically, the spinal ligaments (and muscles) in turn dissipate the shockwaves created by the refractions which occur at those junctions, but as the healthy elasticity of the ligaments is lost, their ability to perform this function declines, especially if the area is subject to repetitive stress or a powerful shockwave.
Note: this is very similar to how discs in the spine eventually fail.
Two scenarios help illustrate this concept.
First, any time metal hardware is put into the spine, it freezes the intrinsic mobility and elasticity of the spine, thus creating a much denser medium for any wave of force to travel through. As a result, a common problems with spinal fusions (especially those in the neck) is that the vertebrae and ligaments adjacent to the fusion will gradually become worn down, which in turn often requires additional fusions to be performed on those vertebrae too. Furthermore, the body becomes much less able to smoothly transfer and dissipate the energy which runs through it, which results in greater amounts of shock being retained within the body (e.g., in the head).
Second, because the neck has much greater mobility than the thoracic spine, if a strong force goes through it, it will often lodge in the bottom of the neck as the top thoracic vertebrae (due to the top rib) has much less motion than the bottom cervical vertebrae. Let’s now consider what happens in a whiplash injury:
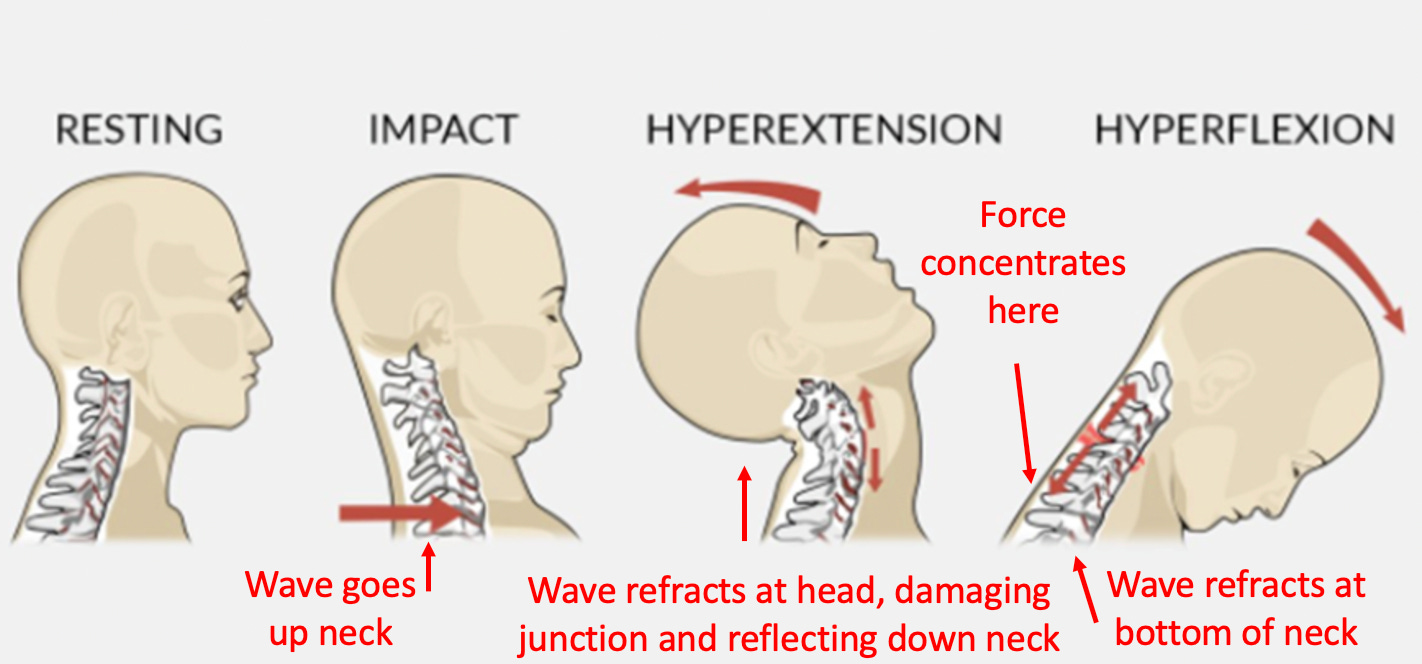
One of the most common symptoms of whiplash is dizziness. I believe that is because once the wave refracts at the bottom of the neck, it often partially tears the ligament that stabilizes the back of spine.
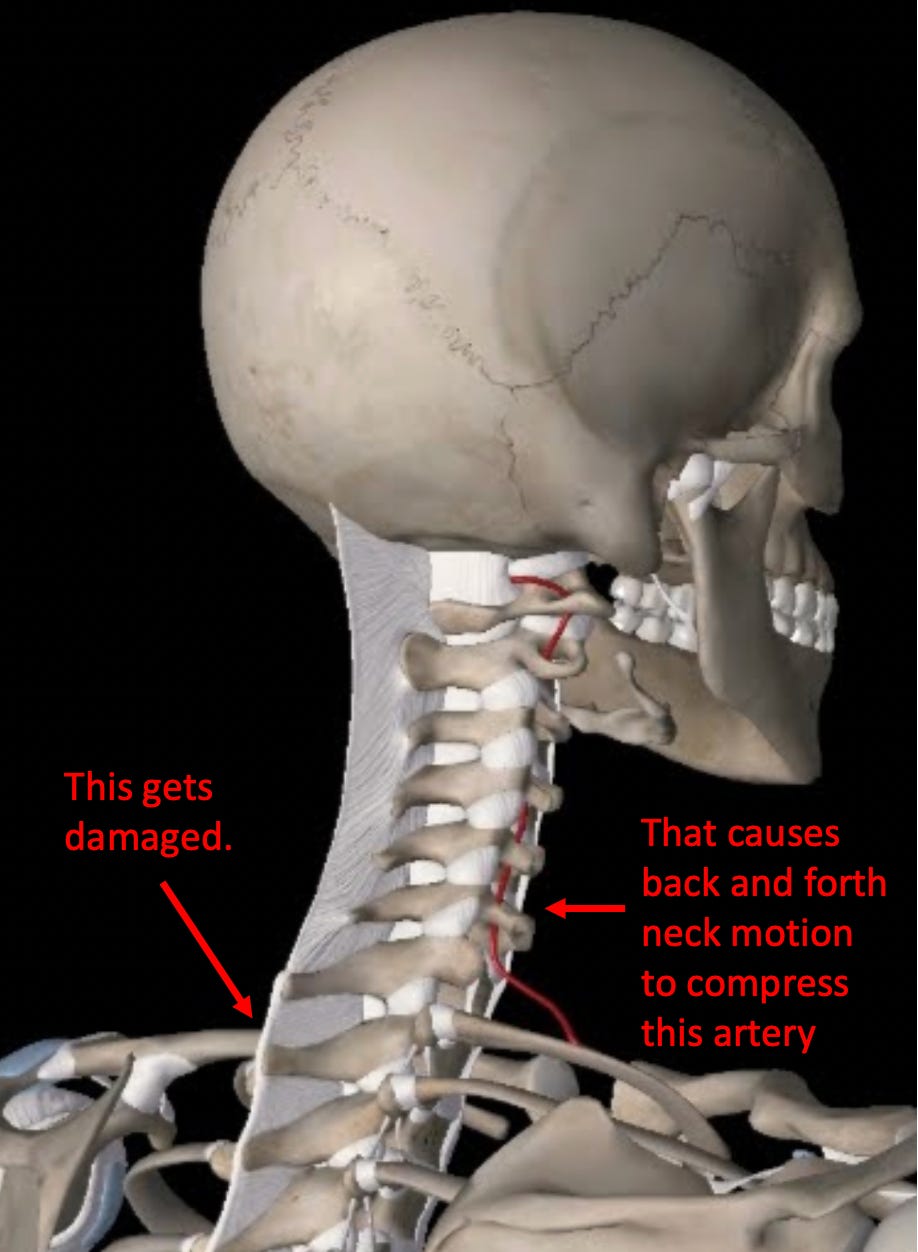
Once this ligament is damaged, vertebrae in the neck can inappropriately slide forwards or backwards. This becomes a problem because the vertebral artery travels in a small hole in the side of each of those vertebrae, so if they slide, the vertebral artery often becomes compressed. This sliding is most commonly triggered by bending the head backwards, but can also result from bring it forward, or just having vibrations pass through the body (e.g., while driving).
Since the vertebral artery feeds the parts of the brain that process orientation in space (the vestibular system and the cerebellum), if blood flow is intermittently interrupted to those regions, this can trigger dizziness. While this concept seems abstract, in practice I and colleagues find a weakness in the ligament behind the first thoracic vertebrae is one of the most common causes of dizziness, best demonstrated by how often the condition improves once those ligaments are repaired.
In most cases (which sometimes requires extensively going through the history), we can identify a whiplash injury as the responsible culprit for that whiplash damage. However, in many cases it was a minor injury the patient did not consider to be significant until the correlation was explained to them. I mention this to illustrate how it is for damage to occur at the refraction zones in the spine and why it is thus not necessarily the best good idea to artificially create them with a spinal fusion surgery.
Conclusion
In this article, I’ve tried to illustrate how the approaches we use to manage spinal pain often create a variety of major side effects, including worsening the existing pain. Sadly, while the examples I’ve shown here are disturbing, what happens with spinal surgeries is arguably worse—which in understandable given the perverse incentives that exist to perform these highly lucrative surgeries.
In the second half of this series (which can be read here) we will explore the spinal surgery industry and review the myriad of safe and effective treatments for spinal pain that are relatively unknown due to the fact there is very little money to be made off of them.
Lastly, I wanted to thank each of you for your support of this Newsletter—we’ve now passed 60,000 subscribers and I’m starting to periodically meet people who share that they read it (so a few of my Midwestern readers may have met me without realizing it).
I have been trying to get information like this out to patients for years but over and over doing so was like trying to climb an impossibly high mountain and I never imagined I would have the opportunity to do so. Much of that has been due to each of you sharing this publication with people who you believe could benefit from it, and to thank each of you who has, I’ve set it up so that Substack will automatically provide complimentary subscriptions to you for referring this newsletter to your friends.
I have an anecdotal support for your point: I had an event that resulted in intense lumbar pain and I was duly referred to a well-known specialist at a very large hospital. While waiting for the specialist to come into the examining room, I was able to overhear the employee at the front desk making phone calls. She made the same call over and over: “The MRI shows you have a stenosis, for which the only treatment is surgery.” I thought that was a little curious and filed that information away. Finally, the specialist came in and, after perfunctorily taking my “history”, recommended an MRI. I think even he felt a little awkward that he never even really looked at me, and so had me briefly pull up my shirt and point to where it hurt. Sure enough, a couple of days after the MRI, I got the “stenosis” phone call. My intuition told me not to go, and I didn’t.
The pain subsided and was manageable for a few years, but again I went to a (different) specialist who duly ordered another MRI, after which he informed me that I was not a candidate for surgery (his words were essentially that I could go to someone else and get surgery, but he was confident that I would come back to him to fix their mess) and suggested physical therapy. When he asked me what I did for pain, I told him OTC analgesics. He gave me a peculiar look and said “I can prescribe something stronger if you want”. I didn’t want, but got benefit from the physical therapy and have taught myself how to manage the problem, within the bounds of the underlying condition, through proper stretching.
Now, of course I have no idea whether the surgery would have helped or harmed (I suspect the second specialist may have been right), but I’m done with doctors, and will just live within the limitations of my minor disability.
As always, reading your substack gives me valuable information and teaches me so much.
Thank you for your insight and for sharing so openly with us.
My son is autistic and it is from Tylenol. I hope one day that something might be done to help him and all others who were injured by this drug. I struggle with bitterness every day of my life about what happened to him and I worry about who will care for him after I'm gone. I hate even looking at Tylenol and I avoid it like the plague.