What Causes Alzheimer's Disease?
The causes and treatments of dementia are critical to understand for the era we live in.

In the first half of this series, I reviewed the tremendous costs to our society from Alzheimer's disease [AD]. Because of the urgency to address AD, billions have been spent researching it (for example the NIH was allotted 3.5 billion in 2022), yet, despite decades of research, we are still no closer to a cure for this condition.
This article from one AD activist further highlights both the incalculable human cost of these failures and the systemic corruption with the industry that maintains them while simultaneously vociferously attacking anything which does address the problem and threatens to dry up the billions the AD “research” industry receives each year.
I have come to believe that most industries or advocacy groups that are tasked with addressing a problem (if not held accountable for their failures) will inevitably fail to solve the problem, as solving it so would take them out of business. In the case of AD, there has been a tunnel vision focus upon amyloid plaques being its cause and countless failed attempts to treat AD by removing those plaques, with some of the examples highlighted in the previous article bordering on absurdity.
Much of the focus on the amyloid hypothesis was a direct consequence of intentionally doctored research. Sadly, the scientific community has so far refused to retract that research, which I suspect is because doing so would jeopardize the enormous industry built upon assuming that research was valid. Although this is an immense scandal that must be brought to the attention of the public, I believe the greater value to the story lies in contrasting the actual mechanisms behind AD with the conventional scientific conception of it.
Note: there are a variety of causes of dementia. While AD is the most common, other forms such as frontotemporal dementia and vascular dementia also frequently occur. In many cases, the exact type of dementia one is diagnosed with it is not always correct. One study found 30.2%-56.7% of those diagnosed with AD did not have it, an autopsy study found 12-23% did not have it, and a study found 63% of those with AD also had another dementia causing disease processes within their brain (an issue that increases with age, further increasing the difficulty of accurately diagnosing dementia). However, since each of these diseases share a similar process that causes their formation, it should be understood that what is described here often applies to treating forms of dementia besides AD.
Physiologic Momentum
Everything within the body is designed to adapt to the circumstances it finds itself within and to maintain the stable internal environment necessary for life. For this reason, chronic illnesses are often the result of a maladaptive physiologic process becoming established and distorting the physiology of the body, which in time creates the symptoms associated with a specific disorder. Within the holistic fields, it is often emphasized that the cause of disease should be focused on rather than its symptoms, but much less frequently is it acknowledged that the “cause” is typically a process that represents the culmination of a deeply established physiologic momentum and that a certain amount of time is always required for the positive momentum to yield results.
A recently published book, Malcom Kendrick’s The Clot Thickens, highlights how a very similar situation exists for heart disease as that for AD. Heart disease, like AD has enormous social consequences, and a massive research and treatment industry has been built around it that has been pigeonholed into heart disease having a single cause: excessive cholesterol. However, despite many lucrative (and harmful) treatments for reducing cholesterol having emerged, none have shown any real success in alleviating heart disease.
The industry’s response has been not to change course on the cholesterol hypothesis, but rather to double down and develop even more extravagant, and likely more dangerous ways to reduce cholesterol (which I suspect is because they can be patented as many of the statins are nearing the end of their patents). This was first done by creating monoclonal antibodies which targeted the protein that causes cells to release excessive cholesterol into the bloodstream (it may not be the best idea to stuff cells full of cholesterol). Then not long after, a gene therapy was developed that directly stops the production of this protein for a much longer period (I initially had difficulty believing this was being done when a friend called me up to inform me about a drug rep who had just shown up at his office promoting it). Now they are developing vaccines to create permanent autoimmunity to the protein.
Kendrick spent years trying to untangle the mystery of heart disease and eventually realized the epistemological error he like everyone else had made, was to focus on a single cause of heart disease rather than viewing it as the result of a normal physiologic process that had become maladaptive. Briefly, Kendrick's model is as follows:
•Cardiovascular disease, in most cases is due to damage to the arterial system, which often occurs as a result of lack of vitamin C (which humans and guinea pigs lost the gene to synthesize).
•This damage primarily consists of atherosclerotic plaques in those blood vessels.
•Although atherosclerotic plaques are believed to result from excessive cholesterol deposition on those blood vessels, there is a large body of scientific evidence that disproves cholesterol’s role in forming atherosclerotic plaques.
•Kendrick instead argues that these plaques are a result of successive blood clots forming at the site of a blood vessel injury, and the cholesterol found there is either from blood cells or the body using cholesterol to repair the damage because vitamin C is not available [vitamin C is also very important in the treatment of COVID-19 and to a lesser extent vaccine injuries including those from spike protein vaccines). Initially, this process is life-saving (otherwise you would inevitably bleed to death), but over time, it becomes maladaptive because successive healed blood clots interfere with the normal circulatory functions of the blood vessel.
•Many of the factors linked to heart disease (e.g. diabetes, smoking, lupus) all share the common characteristic of damaging the blood vessels and thus starting the clotting process within them.
Kendrick provides a remarkably solid case for his hypothesis. In addition, he also ties together many other crucial factors, such as the importance of protecting the blood vessel lining (the endothelium) from damage, the need for nitric oxide synthesis, and the enormous contribution of psychosocial stress to cardiovascular disease (which also plays a key role in disorders like AD and the metabolic syndrome).
Note: I strongly agree with this model, but believe it is incomplete as other factors (some of which will be discussed here) also play pivotal roles in heart disease.
There are three key reasons why the story of heart disease is so pertinent to the story of AD.
•First, both cannot be treated with a single silver bullet aimed at an uncertain cause; instead each requires reversing a maladaptive physiologic process and allowing normal physiology to establish a momentum that can restore health. Regardless of how much money we throw into researching it, no degree of amyloid or cholesterol removal will solve either of these diseases.
•Second, many of the causes and processes Kendrick ascribes to causing cardiovascular disease also frequently contribute to dementia.
•Third, many of the factors Kendrick identified as being the key contributors to causing cardiovascular damage are pathologic factors also shared by the COVID-19 spike protein (e.g. the spike protein vaccines are remarkably effective at attacking the endothelium), which helps to explain why COVID-19 vaccinations are frequently associated with heart disease, blood clots or strokes, and dementia.
Most businesses rely upon having a recurring sales model and a guaranteed market they can indefinitely provide their product to (hence why there is such a strong disincentive to ever produce an actual solution to a problem an industry is tasked with addressing). Similarly, to sustain a pharmaceutically focused medical industry, it is necessary to view each disease as having a single cause which can be targeted by a single drug that is then sold to thousands or millions of people alleged to have that disease, with the drugs being periodically updated as the lucrative markets for previous drugs expire due to waning patent protections on the drugs.
In addition to the enormous development and advertising costs needed to bring a pharmaceutical to market, a large number of people have to be paid off to support this model (e.g. politicians who legalize the medical monopoly, the drug regulators who approve the medications, and those who provide the medications). As a result, the drugs are priced accordingly; those given to smaller numbers of people or only on a short-term basis are much more expensive (with a few costing over a million for a course of treatment and quite a few costing tens of thousands per month), while those distributed to the masses, although still expensive are priced significantly lower.
Since many diseases instead require an individually tailored gradual repairing of a maladaptive physiologic process (which industry cannot monetize and thus avoids), the current model of medicine often fails abjectly. However, since so much inertia has been established behind it (healthcare expenses now accounts for one-fifth of all money spent in the United States), a too-big-to-fail type situation has been created, leading to countless fiascos like the amyloid hypothesis continuing to dominate research (despite its pivotal study proven to be fraudulent) or the medical profession repeatedly doubling down on a dangerous and ineffective vaccination.
Additionally, as Robert Malone has highlighted within the vaccine program, these industries often cannot handle a “pause,” which is a key reason why useless influenza vaccines are promoted each year (as the U.S. needs to maintain its capacity to manufacture vaccines in the event of a pandemic).
Although many diseases could be chosen to highlight this dynamic, I believe AD represents one of the best examples. As detailed in the previous article, because of the massive consequences AD brings to society, we have made enormous investments in finding a cure for the disease, all of which have failed. On the opposite end of the spectrum, numerous approaches have been developed that mitigate or treat the disease by focusing on the processes that create it, including one that was proven to do so in clinical trials. Despite this, those approaches remain almost completely unknown.
Changes in the Nature of Illness
From an evolutionary perspective, human beings have remained relatively unchanged since the industrial revolution as far too few generations have been born to shift our genome (although mRNA technology may change this) and many diseases that were present at the dawn of recorded history are still with us. However, our environments have undergone a rapid unprecedented shift, and since our genome has not changed significantly, in many cases our species has not successfully adapted to its new environment.
Numerous medical systems have observed the nature of human illness has changed throughout the ages (I believe Chinese medicine, due to its long written history has done the best job of documenting this), and again and again, how widespread disease results from certain changes in our environments. In my own exploration of this subject, I found that the most significant decline in the health of the human species began approximately 150 years ago around the time of the smallpox vaccination campaigns, accelerated in 1986 after the vaccine manufacturers became shielded from any accountability for their products, and again accelerated after the “emergency” COVID-19 vaccination campaign. However, while I believe vaccines have played a key role in this debacle, I also believe they are by no means the only factor responsible for what has occurred.
Since my initial discovery, I have learned that many other healthcare practitioners have made similar observations, with each remarking that throughout the course of their careers, patients have become much sicker and harder to treat (which in my eyes explains why some therapies do not provide the “miraculous” benefits or therapeutic responses attributed to them in the past). I asked many of my mentors (who belonged to different fields of medicine) if they observed those same trends, most did, and in a few cases, informed me they had asked the same question of their mentors. From this, I have been able to determine that a continual decline was observed since at least 1900.
The majority of the debilitating diseases that have resulted from this decline in health are neurological and autoimmune in nature. Cognitive decline is a common consequence of the unhealthy changes that have emerged in our environment, and for this reason, the causes of dementias like AD provide an excellent means for understanding the origination of many other chronic illnesses we face.
Medical Diagnosis
The art of diagnosis is tricky. Frequently, since the precise testing to identify an illness is expensive and inaccessible, a far less precise method such as a physician’s observations is used to diagnose an illness. Many doctors cannot recognize subtle signs of illness and lack a framework that has the correct diagnosis for those symptoms. Oftentimes, since there is so much variation in individual response to illness, the same disease can present quite differently, with many individuals being on a cusp where it is difficult to determine if they do or do not have a specific disease.
Medicine solves the inherent uncertainty human physiologic variability creates by forcing everything into a rigid diagnostic box that catches some cases and misses others. I instead address this challenge by viewing everything I encounter as the countless manifestations of a single shared cause. This style of thinking runs in opposition to our educational system which teaches everyone to see things as linear lists to fit into algorithms, and as a result, doctors often struggle with understanding diseases such as mold toxicity, Lyme disease or COVID-19 vaccine injuries which can have entirely different presentations depending on the patient.
In the case of cognitive decline and dementia, we typically classify them by if the change is sudden or gradual (sudden changes, if severe, are known as delirium, and are often reversible if the causative agent is identified). The chronic ones are much harder to reverse and are often classified by the agents known to improve them (for example depression is a common cause of cognitive decline in the elderly), the results of expensive tests, or the pathological findings found during autopsies (which is helpful since different causes of dementia are more likely to exhibit certain symptoms). Unfortunately, while we have developed a sophisticated means for classifying these diseases, we have fairly limited options for treating them, which I believe arises from their actual causes not being recognized and these labels being applied instead of identifying those causes.
In writing this article, I also conferred with numerous physicians I know who have had success treating dementia (hence why it took so long). Here, I will compare their observations with the most compelling research in this field, the work of Dale Bredesen M.D., a neurologist who established an affordable protocol that was proven to successfully treat dementia and has since been replicated by many other physicians (including distant friends of mine). Since many of my references are from his book, I strongly suggest those wishing to learn more read it.
In the same way that a complex chronic diseases symptoms can vary greatly from patient to patient, there can also be completely different things which cause the same disease leading to none of the original causes being recognized as the cause and instead the disease remaining in diagnostic limbo as a poorly understood “syndrome.” Bredesen in turn argues that there are three different types of AD, that it is possible to discern which type is occurring from the patient’s presentation and that each treatment must be catered to the type that is occurring. The types are as follows (sometimes 1 and 2 can occur concurrently):
•Type 1–Excessive inflammation (often metabolic or infectious in nature) that causes the brain to support the inflammatory process and to protectively reduce brain cells that are not deemed essential. It typically occurs in the sixties to seventies, but for those with the strongest genetic predisposition, it occurs in the late forties to fifties (and in the late fifties to sixties for those with a weaker genetic predisposition).
•Type 2–Nutritional and hormonal deficiencies (e.g. vitamin D, thyroid hormone, progesterone) which cause a similar neuronal downsizing to that seen in type 1. Type 2 typically occurs about a decade later than type 1.
•Type 3–A toxic agent is present in the brain which directly kills brain cells. Unlike the first two types, type 3 occurs earlier in life, has a weaker genetic link, and the process of neuronal destruction is not selective, so a variety of cognitive (and psychiatric) impairments occur rather than the classic inability to store new memories associated with the early stages of AD.
Note: Since publishing this original list, Breseden updated it to include a type caused by vascular dysfunction and a type caused by a severe concussion or multiple smaller concussions (this is a very common issue in professional football players, which as Pierre Kory shows the NFL has used the scientific disinformation playbook to cover up for decades).
Understanding these types helps to explain the functions of amyloid and why attempts to eliminate it are doomed to fail. To quote Bredesen:
“This mirrors the three hats worn by the multitalented molecule, amyloid-beta, which is derived from APP. It is part of the inflammatory response and can function as an antimicrobial agent (thus it is part of your body’s ability to fight infections); it responds to inadequate levels of hormones, vitamins, nutrients, and other supportive (or trophic) factors by downsizing the more expendable synapses; it is part of the protective response to toxin exposure—for example, binding very tightly to metals such as mercury and copper.”
Although I strongly agree with Bredesen’s model (which he admits is also applicable to other forms of dementia) and recognize that as a genuine expert in cognitive decline, he has far more knowledge in this area than I ever will, I also feel it is incomplete. Like many multifactorial models of disease (he incorporates dozens of factors into developing his treatment plans), his model fails to answer why individuals can have such dramatically different responses to the factors he has identified as causing dementia, and why some are seemingly immune to developing cognitive decline.
The Circulatory Hypotheses
To write this article, I interviewed a few highly regarded physicians who had been known to reverse cognitive decline. All of them told me that the further dementia had progressed, the harder it was to treat, and after a certain point, all they were able to do was halt further decline as they viewed the existing damage as unrepairable.
To some extent Bredesen shares this sentiment and believes it is critical to address Alzhiemer’s disease in the decades leading up to severe cognitive impairment as much more can be done then. However, unlike my mentors, in certain cases, Bredesen has been able to reverse later stages of cognitive decline.
Each of the physicians I spoke with shared the belief that dementia was often circulatory in nature. For example, to quote one:
“Dementia is normally due to poor blood flow to the head and too many toxins being present in the brain. If you can fix the cerebral circulation and drainage early in the disease process (which is often impaired because of a previous traumatic brain injury), you can reverse it, and if you do so later, at least stop its progression. In addition to directly addressing the circulatory issues, I often must do some type of general therapy for them such as addressing the underlying imbalances in their constitution. I also believe the energy present within the blood must reach the brain, which based upon what you have told me about zeta potential, is likely dependent upon the dispersion of the blood.”
Cerebral circulation is extremely important for:
•Delivering the nutrients necessary for preventing type 2 AD (which to some extent can be surmounted with supplementing larger amounts of those nutrients).
•Draining the inflammatory products that create type 1 AD.
•Eliminating toxins from the brain.
•Removing amyloid protein from the brain.
•Facilitating healthy sleep (which as Bredesen notes is critical for preventing minor cognitive impairment from progressing to dementia). For those interested, this is the best book I have found on the physiologic importance of sleep (although like many books, it makes a few exaggerations not supported by the existing evidence).
As mentioned above, one of the most consequential mismanaged diseases of the modern age is heart disease, and in many cases, the same circulatory impairments which give rise to heart disease also give rise to dementia. As a result, there is a large overlap in therapeutics for the two, and many of the therapies Kendrick shared for addressing heart disease, such as chelation therapy or the nitric oxide producing PDE5 inhibitors, also have been observed to prevent dementia and improve cognitive decline (e.g. in a study of approximately 7 million Americans, Viagra was found to reduce the risk of AD by 69%).
Similarly, there are many other therapies Kenrick did not discuss which have proven themselves for addressing heart disease that also reverse cognitive decline. One example is ultraviolet blood irradiation (which provided it is correctly administered also often helps acute or chronic COVID-19 and spike protein vaccine injuries).
Another, external counterpulsation therapy (ECP), involves having external pumps on the body which move one’s blood in coordination with the electrical signals emitted as the heart beats.
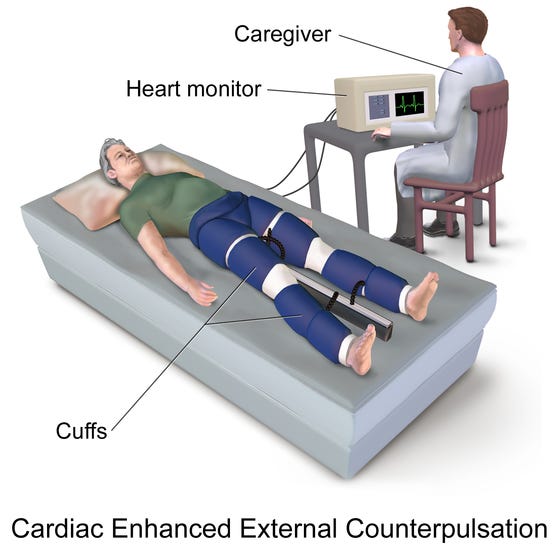
ECP is well known for improving heart failure (for example, it causes the heart to form new collateral blood vessels, thereby increasing its blood supply–which in effect is a non-invasive form of coronary artery bypass surgery) and has met significant resistance from the cardiology profession as it often provides a cheaper alternative to the procedures their livelihoods depend upon. One of my colleagues has also found ECP is also very helpful for treating the heart damage that follows COVID-19, while another showed me many of ECP’s benefits can also be observed in the kidneys and for various types of cognitive impairment including those progressing towards dementia.
Zeta Potential
Note: I would highly advise reading the article below to fully understand what is presented in this article. It also contains the references and graphics for this section and details how many of these concepts apply to the vaccine spike protein. Lastly, this section also contains additional information not covered within the article.
When a substance is mixed in water, it has three options, not mix with it (typically either floating to the top or settling to the bottom), dissolve like a salt, or form a colloidal suspension. Stable colloidal suspensions are typically finely dispersed microparticles and as that stability is lost, the particles clump together in larger and larger agglomerations which eventually will separate out from the surrounding water.
I believe that not recognizing the significance of colloidal stability in biological solutions is one of the largest oversights in modern physiology. For example, a variety of medical systems (e.g. Chinese medicine) have recognized that if blood clumps together, a large number of diseases, including countless circulatory problems emerge. Furthermore, as the clumping or agglomeration gets worse and is able to obstruct progressively larger blood vessels, organisms move closer and closer to death—decades ago it was demonstrated that malaria kills by causing this to happen in the largest blood vessels unless a blood dispersing agent is administered; recently Pierre Kory informed me through ultrasound (he is a specialist in critical care ultrasound) he repeatedly saw critically ill patients developing clumps of blood in their largest blood vessels and pass away less than an hour later much like the monkeys did in the malaria trials decades ago.
A key factor that determines if colloidal solutions clump together or remain dispersed is the balance of electrical charges present (positive charges agglomerate, negative charges disperse). Zeta potential provides a way to model this immensely complex balance and explains why tiny amounts of positive ions with high charge densities (e.g. aluminum) are capable of agglomerating colloidal suspensions, and why microstrokes often follow injections of these substances.
Decades ago, very few options existed for treating heart disease and it thus was often a death sentence. Riddick, a colloidal engineer with a debilitating heart condition had the epiphany that blood behaved as a colloidal suspension and if its zeta potential was corrected, would likely become dispersed again and resume a normal flow. After this corrected his heart condition, a physician in a similar situation learned of his work, also was cured and went on to develop a successful medical practice focused on treating zeta potential.
In addition to helping heart disease this now deceased physician also discovered restoring zeta potential was remarkably effective for a variety of other medical conditions including various types of cognitive decline such as AD (although after a certain point in the disease process, he found restoring it could only prevent its progression rather than cure it). His practice eventually shifted to helping individuals age without decline, and solely through focusing on zeta potential, he was able to retain a sharp mind that could practice medicine into his early 90s (this is very rare).
Colleagues who attempted to replicate this work found that while treating zeta potential was still quite helpful, they did not observe the same degree of benefit in reversing cognitive decline that the earlier doctor did. Each of us believes this is reflective of the changing nature of illness described before and the increasing environmental toxicity burden we are exposed to.
Riddick also observed that the normal zeta potential of the blood allowed dispersion, but was very close to the threshold necessary for agglomeration and thus clotting to initiate (many agents that increase colloidal dispersion also function an anticoagulants). This calibration he hypothesized was an evolutionary adaptation that allowed clotting to immediately occur following the rupture of a blood vessel (so you don’t bleed to death), as the normal flow of blood creates a small degree of colloidal dispersion and losing this dispersion was hence sufficient to cross the threshold into agglomeration and thus clotting. I suspect that because there are now a large number of factors that cause colloidal agglomeration in our environment, the physiologic zeta potential our species evolved with is no longer correct and natural selection will gradually favor those with a more electronegative zeta potential that is further from the agglomeration threshold.
It should be noted that many aspects of aging reflect a worsened physiologic zeta potential (which likely results from decreased kidney function). Amongst other things, this explains why elderly individuals are so much more vulnerable to temporary reductions in zeta potential, such as those which follow viral respiratory infections or aluminum-laden vaccinations (this point was made to me by an older patient I admitted to a hospital who during intake step by step described the progression of a zeta potential collapse following a pneumococcal vaccine).
Note: there is a huge variability in lot-to-lot vaccine aluminum concentration, which likely explains part of the variability seen in injuries that follow vaccination
Cerebral Lymphatics
Blood is not the only biological colloidal suspension that agglomerates in response to a decreased physiologic zeta potential, and I believe many of the consequences of blood agglomeration described by other medical systems (e.g. the autoimmune disorders attributed within Chinese medicine to blood stasis) are due to the concurrent stasis of fluids besides blood.
One of the most consequential fluid agglomerations is that of the lymphatics, the drainage system of the body (which amongst other things is what removes products of inflammation from tissues). The brain’s lymphatics (the glymphatics) are particularly vulnerable to this issue as rather than having specialized lymph vessels, its lymphatics exist in a perivascular space within the blood-brain barrier (a structure which is frequently disrupted in neurological illnesses such as AD, COVID-19 and most likely spike protein vaccine injuries—although it may be a while before someone will risk their career to research that).
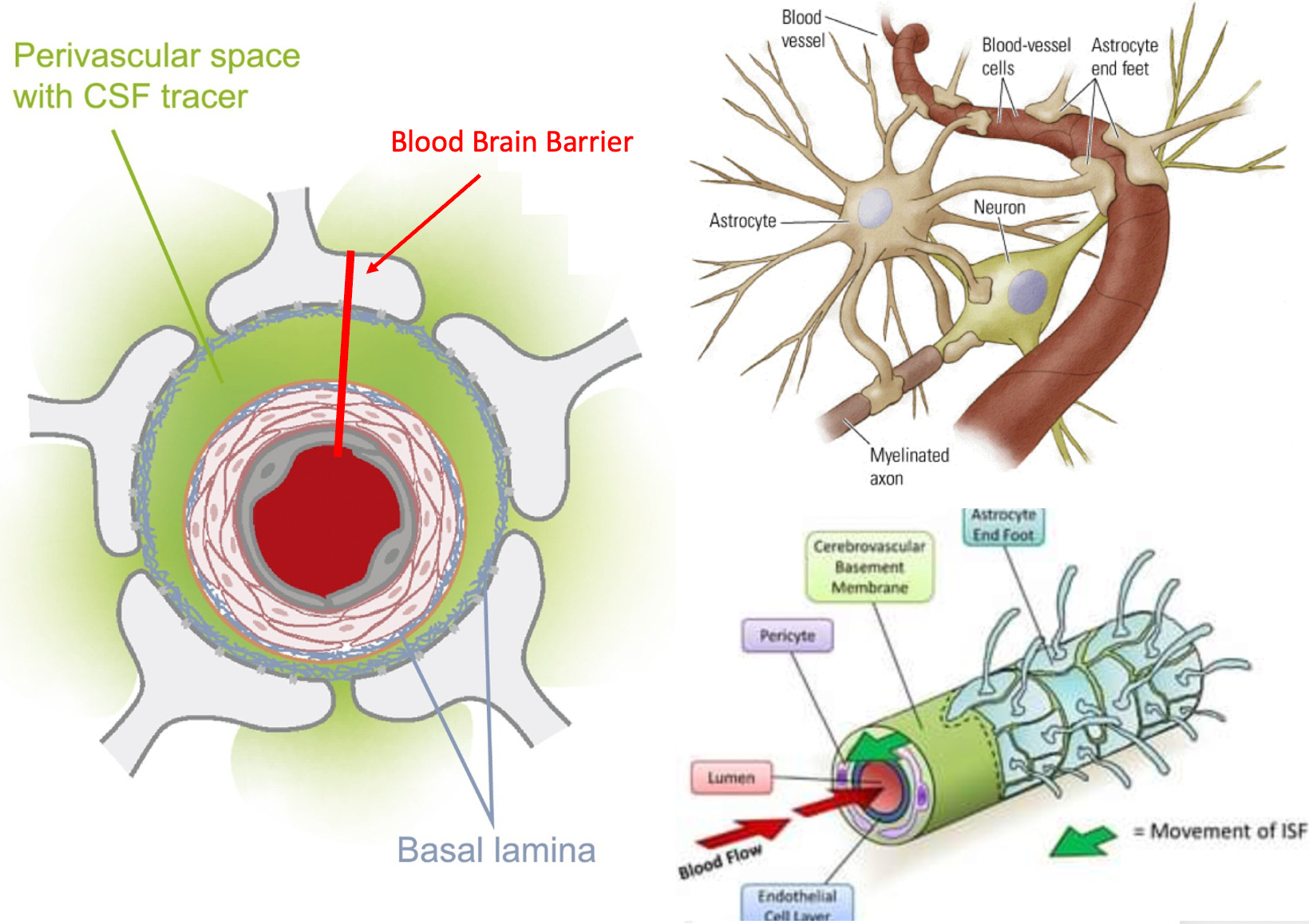
Since this space is hidden between the feet of the astrocytes and the walls of the blood vessels and only expands during the night when you sleep as the astrocytes pull their feet back to support glymphatic drainage (a key reason why proper sleep is important for preventing AD), it was not discovered until 2013. The structure of this system is important to understand because the only pump it has are the external walls of the blood vessel, and it is thus highly vulnerable to lymphatic agglomeration obstructing its flow or pathologic changes to the adjacent blood vessels that reduce their pumping motions.
Many different neurodegenerative disorders, especially those of aging, are associated with impaired glymphatic drainage (for example, traumatic brain injuries reduce glymphatic drainage, which helps to explain why experiencing a second concussion prior to the healing process completing can be so devastating and their association with AD). In the case of AD, the brain relies upon the glymphatic system to remove the neurotoxic and inflammatory agents linked to AD along with its pathologic proteins (e.g. amyloids), so disabling this system (either directly or temporarily through sleep deprivation) in turn increases the levels of those proteins by reducing their clearance.
In the same manner that physiologic zeta potential decreases with age, glymphatic drainage also decreases with age. As this decrease occurs in conjunction with the increased incidence of neurological degeneration with aging, the glymphatics have been argued to be the shared pathway for many of those disorders, which I would argue also suggests zeta potential is a key concern.
Many other factors such as your sleeping position (it is not good to sleep on your stomach), the phase of sleep you are in, and possibly utilizing an inclined bed, affect glymphatic drainage.
One of the factors most associated with glymphatic drainage is the presence of melatonin in the brain. Interestingly once in the brain, melatonin is rapidly metabolized to 6-hydroxymelatonin sulfate. Because sulfates are one of the most effective negatively charged ions for improving zeta potential, the body often relies upon sulfated molecules for this purpose and may also do so to facilitate glymphatic drainage.
As melatonin secretion is highly sensitive to your external environment (e.g. the blue light we are exposed to has a horrendous effect on melatonin production), many experts, including Bredesen, argue for improving sleep hygiene to prevent neurological degeneration, while other highly regarded integrative physicians such as Dietrich Klinghardt endorse using liposomal melatonin to improve glymphatic drainage (his brand and DaVinci are the only ones I know of that seem to work for this purpose), which Klinghardt argues is critical for addressing many complex illnesses. The glymphatic system is responsible for many of the restorative effects we experience following sleep (e.g. a clear head), which is most apparent when working with patients who have complex illnesses and highly disrupted sleep patterns.
The Life of Cells
One of the things I continually marvel at about nature is not only the ability of a species to genetically adapt to their environments, but the inherent adaptability each organism has within its own lifespan to adapt to its environment. Within the human body, there are many systems that are designed to change based on the needs of one’s environment (e.g. this is why weight training creates larger muscles), and among the most adaptable is the nervous system.
At any given moment, neural circuits which support certain activities are reinforced, while other circuits are pruned and eventually disabled, a process that allows the nervous system to adapt to the complex needs of its environment. At the same time, many complex neurological and psychiatric disorders arise from a momentum being established where dysfunctional neurological circuits perpetually reinforce themselves.
For these disorders to be treated, a momentum must instead be established behind a healthy circuit (for those interested, this is the best book I have seen on that subject). This momentum is a key reason why it is so important to have healthy thought patterns and regularly actively exercise your brain (another core component of programs for preventing AD). If you do the opposite (e.g. watch T.V. all day), dysfunctional patterns can become established habits, while neurological damage occurs as parts of the brain you need but under utilize are pruned away.
A key way the brain accomplishes this adaptability is by eliminating neurons that are no longer deemed essential. Bredesen’s theory of AD is that it results from the balance between preserving and eliminating neurons being shifted towards eliminating them, which inevitably will result in cognitive decline. Bredesen thus advocates for reversing that balance by creating an internal environment that preserves neurons and eliminates the factors that promote cell death.
Within Bredesen’s model, amyloid protein plays a key role in this process, as when it is initially formed as amyloid precursor protein (APP), it has the choice to then be split into two or four parts. If it is split into two parts, those parts protect the neurological function in the brain, while if it is split into four parts, the neurological function of the brain is damaged and brain cells are eliminated. Interestingly, its splitting into 4 parts causes future APPs to also be split into 4 parts (which creates a downhill spiral), and as a result, Brenden’s approach focuses on regaining a healthy momentum towards the two-part splitting while also providing the signals cells within the body require to survive.
One of the better models I have come across for understanding complex illness, the cell danger response, shows that in response to environmental stressors or pathogens, cells can enter a defensive metabolic cycle where they partially or fully “turn off“ (e.g. mitochondrial respiration and protein synthesis within the cell decline). The cell danger response is often observed in patients with chronic illnesses (e.g. fibromyalgia or childhood vaccine injuries), and when looked for, is frequently observed following COVID-19 vaccine injuries.
A variety of therapeutic strategies have been put forward for treating the cell danger response. Suramin for example, which blocks the signaling pathway that maintains the cell danger response, when tested (both in a small clinical trial and by physicians in practice) was remarkably effective in improving childhood autism, but unfortunately is no longer available (it is difficult to manufacture correctly and the only pharmaceutical company which did so recently stopped producing it).
Note: Pine needle tea is often stated to contain small amounts of suramin, and is one of the few treatments for COVID-19 vaccine injuries I have seen numerous people report a benefit from online. At this point in time, I have not been able to locate any research showing suramin is present in pine needle tea.
One of the more promising approaches to treating cognitive decline also targets this process of the cell turning off by disabling what is referred to by its proponents as the “integrated stress response.”
“The principle that blocking protein synthesis prevents long-term memory storage was discovered many years ago. With age there is a marked decline of protein synthesis in the brain that correlates with defects in proper protein folding. Accumulation of misfolded proteins can activate the integrated stress response (ISR), an evolutionary conserved pathway that decreases protein synthesis. In this way, the ISR may have a causative role in age-related cognitive decline.”
When tested, an ISR inhibitor was found to restore the structure and function of cells within the brain and to improve a variety of age-related memory deficits in mice.
Within regenerative medicine, one of the most commonly encountered issues is cells becoming senescent and no longer dividing (in other words the cells partially turn off). This is addressed by providing signals to the cells to come back to life and resume their division.
Frequently cells receiving a signal to turn off precedes them undergoing programmed cell death. As Bredesen’s model highlights, neurons within the brain have receptors (termed dependence receptors), which if not repeatedly stimulated, will initiate that cycle, and amyloid precursor protein, if split into 4 parts, blocks those receptors from being stimulated thereby triggering programmed cell death.
Many other things can initiate programmed cell death of the neurons. For example, following vascular strokes, many cells in the brain will turn off, and if not brought back will frequently die, resulting in long-term damage from strokes.
In these instances, IV DMSO (which for reasons I do not understand is quite expensive) is often quite helpful, while oral and topical forms are somewhat effective (I have also successfully used topical DMSO applied to the blood vessel that fed the affected area of the brain at the time of a stroke to resolve the incident). Umbilical cord blood stem cells can also be extremely helpful after strokes and in the early stages of dementia, but are expensive, required a skilled practitioner to administer, and sadly were recently removed from the American market by the FDA.
Another common situation that results in brain cells turning off is anesthesia (which is what has to happen when they put you out). This is problematic because some neurons in the brain will not wake up after surgery is completed, and once looked for, it is often possible to track cognitive decline emerging after the anesthetic was applied at a time that is often too far out (e.g. six months later) for the patient to recognize an association between those two events (although some evidence now exists for this association). This is primarily an issue with inhaled anesthetics (Bredesen does list previous anesthetic exposure as one of the many toxin exposures he evaluates for), and can be avoided if agents such as IV Ketamine or Midazolam (Versed) are used instead for anesthesia, which some anesthesiologists will agree to.
A key aspect of Bredesen’s approach, like many within the functional medicine field, is to use numerous lab tests to evaluate for appropriate nutraceutical and hormonal supplementation (which he extensively details within his book). Due to the cost of this approach, I tend to avoid it, but as Bredesen’s work demonstrates, it is an excellent investment for those with cognitive decline.
“But, surprisingly, they would commit suicide at the drop of a hat! That is, when we disrupted the control cells by taking away some nutrients or adding any slightly toxic compound to the petri dish, they basically fought it off and hung in there. But when we made life difficult for cells containing genes for one or another neurodegenerative disease, they all died, seemingly without putting up even the pretense of a fight! It was like an entire battalion surrendering after the enemy had fired off only a few rounds. Surprisingly, this was true across the board—whether the gene we slipped in was associated with Lou Gehrig’s disease or Huntington’s or Alzheimer’s.”
One of my mentors who has extensive experience in this area and has treated numerous patients with dementia uses a smaller number of neutraceuticals and has found injectable B1 and B12 (B12 deficiency is commonly associated with cognitive decline) are the most important to administer for preventing cognitive decline. If these two vitamins are taken before and after, to some extent, doing so can prevent the adverse events associated with anesthesia and my mentor was able to cite many cases demonstrating the difference in outcomes between patients who did and those who did not.
Note for practitioners: most injectable B vitamins use aluminum as a preservative (which due its effects on zeta potential should be avoided). The only way to get around this issue is to have the B1 and B12 (in the form of methylcobalamin) be prepared by a compounding pharmacy that uses a different preservative such as benzyl alcohol. Additionally, the best results are obtained by subcutaneous administration rather than intramuscular or intravenous administration.
Infections
A variety of infectious agents have been tied to cognitive decline. Interestingly, many of these infectious agents or their toxins also carry a positive charge that adversely affects zeta potential. As a result, it is quite common to observe significant fluid stagnation within individuals who have chronic complex infections (I believe that the resulting lymphatic stagnation is one of the most overlooked problems in these patients), and within patients affected with acute infectious diseases, especially those severe enough to require hospitalization.
Because many of the chronic infections which are the most effective at disrupting zeta potential are difficult to detect (e.g. because they are cell wall deficient bacteria such as mycoplasma) and if bacterial in nature, resistant to many common antibacterials, these issues often go unaddressed. Similarly, I often wonder if many of the negative effects attributed to the infections (e.g. inflammation) actually result from their effects on zeta potential.
Typically, a few infectious agents will be focused on by each practitioner. One of my mentors has found that Cytomegalovirus or Human herpesvirus 6 periodically cause cognitive decline and once an antiviral is administered (e.g. acyclovir for HHV6) a significant improvement is observed. Many believe Lyme disease within the brain is a common cause of many forms of cognitive decline (and to some extent this has been proven). Bredesen in his work highlights the importance of Herpes simplex-1 virus, Lyme disease (a spirochete bacteria), P. gingivalis (an oral bacterium), and various fungal infections (mold toxins are notorious for causing cognitive impairment at all ages). Others also emphasize the importance of oral spirochete bacteria which are able to travel into the brain.
Although identifying the infectious agent can often be immensely valuable for determining the cause of cognitive decline, it can also be quite challenging to figure out which pathogen is the key issue for each patient (and for some conditions like Lyme disease, an immensely time-consuming and expensive infection to address). For this reason, I prioritize broad-spectrum therapies such as ultraviolet blood irradiation that can affect a wide range of infections. It should also be noted that Lyme disease has been associated with heart disease.
Toxins
A foundational component of Bredesen’s approach is removing toxins from the body. Since chemical detoxification is a somewhat complex subject that is frequently written about by many authors (including within Bredesen’s book), I feel it is beyond the scope of this article to detail those approaches. However, there are two classes of toxins I believe bear special importance.
The first are toxic metals, such as mercury and aluminum. Many of these metals respond to chelation therapy with EDTA, and when they are a key issue for a patient, multiple sessions are often required for the desired improvement.
One thing that is rarely appreciated about EDTA is that it is remarkably effective for improving zeta potential (provided it is administered at a low dose that remains in the bottom of the zeta potential curve). Another is that it is possible to take EDTA orally as a liposomal preparation, which will remove metals, although this is not as effective as an IV form and since it must be taken over a prolonged period, essential metals it chelates must be simultaneously supplemented so one does not develop deficiencies of them. Zinc (which is often critical for reducing a dangerous copper overload), magnesium, and manganese are the most important in this regard, particularly since their deficiencies are tied to cognitive decline.
One of the fascinating things about amyloid beta is that like EDTA, it has a negative charge, and preferentially binds positively charged metals that would otherwise cause damage to the brain (chelating agents like EDTA in contrast bind metals and then are excreted from the body, whereas amyloid remains in the brain as plaques). For this reason, I would expect amyloid to have a high affinity for aluminum (additionally due to its charge density, aluminum is a highly effective agent for denaturing and precipitating proteins and I suspect also for causing them to misfold).
There has been a significant degree of controversy on if aluminum is associated with AD. Studies have been put forward suggesting it is not (Bredesen for example believes the evidence is sufficient to link mercury but not aluminum to AD), while others suggest it is and can be found within amyloid plaques.
I personally agree with the author of the latter study, both because he provides a sensible argument for why his results should be trusted, and since many significant financial interests would be threatened by this link being established (which typically results in systematic research fraud occurring). My position may also be a product of bias, as both I and my colleagues have witnessed significant cognitive declines in elderly patients following an aluminum exposure (e.g. an aluminum containing vaccine), and because of the expected effect aluminum’s alternation of physiologic zeta potential would have on glymphatic drainage.
Many different pharmaceuticals have also been linked to cognitive decline, and my own experience has been that most of the elderly individuals I encounter who maintain their mental clarity into old age inform me that they have almost entirely avoided pharmaceuticals throughout their lifetime (which while often beneficial is also challenging because at times drugs are helpful or necessary). Some of the common medications associated with cognitive impairment (Bredesen also acknowledges these links) include:
•High blood pressure medications–As you age, your body becomes less able to maintain an adequate blood supply to the brain, and as a result, blood pressures the elderly are medicated to can drop their blood pressure below that necessary for brain perfusion.
•Cholesterol medications–Statins block the production of many compounds the brain needs to function and are frequently associated with aggressive or paranoid behavior and memory loss (which can go away once they are stopped). The best books I have read on this topic was written by an MD who develop cognitive impairment immediately after starting a statin and demonstrated the issue is extremely common. It should also be noted that levels of cholesterol under 170mg/dL are associated with cognitive decline, while many of our (corrupt) guidelines argue for using statins to maintain a cholesterol level below 150-170 mg/dL
•Acid reflux medications–Because stomach acid is needed for the absorption of numerous vital nutrients, being on a proton pump inhibitor predisposes one to nutritional deficiencies which can eventually result in brain cell death.
•Psychiatric medication–Psychiatric medications frequently cause subtle or overt forms of neurological damage and many prevent the restorative effects of sleep from occurring.
•Antihistamines–These medications also can cause brain damage and prevent the restorative effects of sleep from occurring (most sleeping medications such as benadryl and the benzodiazapenes are sedatives that shut down the restorative aspects of sleep such as the brain’s glymphatic drainage, which to a large extent invalidates the sedatives “putting you to sleep” in the first place).
•Anticholinergics–Some of the most common anticholinergics on the market are those taken by the elderly for incontinence. Like many of the medications above, these medications are frequently associated with cognitive impairment and causing acute episodes of delerium.
Note: Many of the current (but not that effective) treatments for AD are pro-cholinergics. Years ago when I experimented with a variety of nootropics, the only one I ever found helped improve my ability to memorize was galantamine, a common pro-cholinergic treatment for AD (that was also available as a supplement as it comes front a plant), which is primarily used off label to facilitate lucid dreaming, and must be taken at the appropriate dosage.
There are many other neurotoxic medications that are also on the market (e.g. fluoroquinolone antibiotics).
Metabolic Health
Metabolic syndrome is the current term to describe the exponentially growing incidences of diabetes, strokes, obesity, and heart disease within the population (and is arguably the most widespread and impactful syndrome affecting modern society). It is defined by high blood sugar levels, high blood pressure, obesity (especially within the belly), and "elevated" cholesterol levels.
A variety of causes have been attributed to metabolic syndrome, such as our diets being full of processed sugars which continually spike our blood sugar and create insulin dysfunction rather than the nutrients we need to be satiated. While these are contributors, I believe the underlying issue is something else because I have seen numerous cases of individuals who could eat large amounts of unhealthy food for decades without gaining weight suddenly having their metabolism switch and need to be much more judicious with their food consumption to avoid obesity.
Some of the best candidates I have seen put forward include:
•Thyroid dysfunction (which is very common and a common cause of mitochondrial dysfunction)
•Mitochondrial dysfunction (the mitochondria are adversely affected by many of the factors that also cause complex chronic illness including EMFs).
•Many of the chemical toxins in our environment (Joseph Pizzorno, an expert on the effects of environmental toxins makes an excellent case for this).
•HPA axis dysfunction resulting from chronic stress and disrupted sleep cycles (stress-reducing programs are a key component of Bredesen's protocol).
One of Bredesen’s most important points is that the enzyme the body uses to break down insulin (which is nearly always chronically elevated in those who have metabolic syndrome) is the same enzyme it uses to break down amyloid plaques. For this reason, it is often critical to be in good metabolic health to prevent AD.
Note: Chronically elevated blood sugar levels are also well known for causing damage to the blood vessels, and microcirculation, which as this article demonstrates frequently contributes to cognitive decline. Additionally, high blood sugar concentrations will cause colloidal agglomeration, and I believe this is a key, but overlooked mechanism for why high blood sugar levels impair circulation, particularly within the smaller vessels which are the least able to circulate thickened blood.
Because elevated insulin levels and metabolic dysfunction play such a key role within AD (particularly type 1), which has led many to refer to AD as “type 3 diabetes,” Bredesen emphasizes addressing metabolic health within his protocol. Bredesen thus employs many of the common strategies utilized to holistically treat the metabolic syndrome, such as intermittent fasting, regular cardiovascular exercise (HIIT seems to work the best) avoiding gluten (which can be particularly problematic in AD), avoiding processed sugars, and following a healthier diet like the Mediterranean diet or a low carbohydrate primarily ketogenic diet. Additionally, many, including multiple readers here, have also found consuming MCT oil from coconuts (which enables ketosis) improves AD, there is some evidence for it working, and as best as I can tell, while not “the cure” for AD, it is almost comical coconut oil works dramatically better than anything the billions upon billions we have spent on finding AD treatments can offer.
Additionally, like many, he has drawn a link between an unhealthy microbiome and cognitive decline, which is an issue that typically can only be fixed with a healthy diet.
It should be noted that a strong case can also be made that much of our metabolic dysfunction (and systemic fluid stagnation) arises from the extremely unhealthy sedentary lifestyles (“sitting is the new smoking”) we now follow as we are forced to sit in front of the computer all day.
Conclusion
I originally felt compelled to write this series after I began hearing of numerous tragic cases of elderly individuals rapidly developing cognitive decline and dementia shortly after COVID-19 vaccination (documented here), and as the comments on the previous article illustrated, many readers here have observed the same thing often within their immediate family.
It is my belief that many of the causes of dementia detailed here (impaired zeta potential, damage to the blood vessels, small or large blood clots, neurological inflammation, protein misfolding, pathologic alternations of the microbiome, B-12 deficiency etc.) are also caused by the SARS-CoV-2 spike protein. As these issues (along with many other consequences of the spike protein vaccines) can cause a variety of chronic health issues, this speaks to how unwise it was to conduct an experimental mandatory vaccination campaign on the population when most of the short and long term effects of the technology were still unknown.
It is very difficult to comprehend what cognitive decline (which is a nice way of saying losing your mind) can be like until one directly experiences it and the gaslighting that comes with it. Many patients who have experienced adverse reactions to pharmaceuticals frequently tell me that cognitive decline occurs in conjunction with the injury, and in most cases those around them either did not believe it was happening (as this is something that is very difficult to empathize with unless you have directly experienced it) or argued that it was a result of stress.
Similarly (largely because we lack a viable alternative to address the tsunami of unhealthy aging), we treat our elderly who experience these declines quite poorly. Typically they are warehoused in often abysmal conditions where they can be kept out of sight and out of mind until they die rather than being providing a dignified environment for them to conclude their lives within (although a few progressive models like dementia villages do exist for those lucky enough to be have access to one).
It is important to remember that individual responses to an adverse agent (e.g. a toxin) distribute on a bell curve, and the severe acute reactions are much less common than the subtle chronic complications that emerge. In many ways, I view the current form of aging we face (in other cultures and eras the elderly have remained highly functional in old age) as a result of these complications gradually increasing until the body breaks down.
This unaddressed epidemic has affected individuals close to each of us, and in time is likely to affect many of us. I also believe this lack of knowledge around cognitive decline is particularly problematic for our country as our lack of term limits has resulted in many politicians serving in Congress long enough to develop unaddressed cognitive decline and a corresponding inability to address many of the legislative challenges facing them and our nation (I also periodically hear of this issue from insiders within the United States circuit courts because the appointed judge refuses to retire).
In order to cover the topics I felt needed to be covered (especially since they link to the root causes of many other diseases besides dementia), this article needed to be on the longer end. I thank you for your patience in reading this and your willingness to share it with those who could benefit from it (e.g. on Gab or GETTR)!
You missed the low hanging fruit. This is from Hormone Secrets, my book about bioidentical hormones. Your readers can download it free here: https://dl.bookfunnel.com/p7dvqow83g
This sells on Amazon and has 100 five-star reviews.
Women who use estrogen get less Alzheimer’s disease, and some studies say it is 80 percent preventive. But this robust scientific support is unknown to the mainstream. The current standard is to wait until after the disease has advanced, then use toxic, heavily promoted, fantastically expensive patent drugs. Even the academics who are paid to study these understand they are dubious.
AD is tragic and epidemic. Eleven percent of those over 65 have it, and it kills more people than breast and prostate cancer combined. Sixty-seven percent of Medicare long-term care payments are related to Alzheimer’s, more than $250 billion a year—it is the most expensive disease in US healthcare. Our patients are being criminally mistreated.
A similar literature underpins the beneficial effects of growth hormone and testosterone for Alzheimer’s and other diseases of the aging brain for both sexes.
Appendix C has over 50 citations supporting all this. Stop here and spend two minutes scanning them. If you understand this story, the rest of the book will be transparent and credible. Properly referencing every hormone subject would have required dozens of books. --Robertyoho.substack.com
MWD you really do a phenomenal job. I have no idea WHO you are BUT. You are brilliant. I am in contact with so many physicians around the world that I highly respect that set your SubStack on a unique pedestal. Well deserved. Your deep dives as in this post are amazing. Keep up your work.