

What Caused the L.A. Fires and How Can We Prevent Wildfire Toxicity?
What we know about the harms of wildfire illness and a review of the forgotten therapies that treat it

Story at a Glance:
•The Los Angeles area is currently experiencing one of the most damaging wildfires in California’s history.
•These events unfortunately highlight the same recurring themes I’ve seen in each of the previous disasters (e.g., Lahaina) I’ve covered in this publication (e.g., dysfunctional Uniparty rule), but unfortunately, a widespread push is being made to ignore those lessons and instead blame everything on “climate change.”
•Wildfires expose individuals in the area to significant health risks, particularly those who already have sensitive constitutions (e.g., due to a pre-existing chronic inflammatory disease). These effects are best demonstrated by data that was collected on the physical and mental health of the Lahaina survivors.
•This article will explore the strategies which can be used to prevent and treat wildfire toxicity (many of which can also be used for other chronic inflammatory lungs diseases like COPD).
Note: the people in Los Angeles are going through a very tough process right now. In the days to come, it is likely that those there will require an immense amount of support. In turn, if you plan to give money, I highly advise working with a local charity rather than a large organization, as the larger organizations tend to be highly inefficient at bringing your aid dollars to those in need.
Uniparty Rule
One of the major problem with governance is that conniving sociopaths will always exist, and that they tend to have an endless craving for power (as their sociopathy eliminates the intrinsic satisfaction with life many others have). As such, governments inevitably get hijacked by these sociopaths who gradually normalize the exploitation of others (which everyone else is forced to turn a blind eye to), and then eventually shift from exploiting select segments of the population whose suffering can be kept out of sight and out of mind to broad swathes of the population (e.g., consider the abhorrent COVID-19 vaccine mandates).
Note: an excellent overview of this cyclical process can be found in the (brief) Wikipedia summary of Łobaczewski’s Political Ponerology. A key point that Łobaczewski made is that many of these psychopathic tendencies originate from individuals with brain damage that eliminate natural human empathy—a remarkable insight given that its only recently been possible to prove sociopaths have organic brain damage. Additionally, a strong case can be made that the inflammatory brain damage certain vaccines cause results in sociopathic behavior, as a rippling wave of unprecedented violent crime spread across America in tandem with the adoption of the vaccine which was notorious for frequently causing encephalitis (which I discussed further here).
Because of this, I’ve spent decades thinking over the competing models of governance and come to the conclusion famously elucidated by Winston Churchill:
Democracy is the worst form of Government except all those other forms that have been tried from time to time.
More specifically, I believe that since psychopathic individuals will always exist, the best “solution” is to have a form of checks and balances in place where different (likely sociopathic) parties are continually competing against each other for power, and hence “cancel their evil out” by forcing each other to act in a somewhat decent way so they can be the ones to hold into power.
In contrast, anytime healthy competition is eliminated, the quality of government rapidly declines as there is no longer an incentive to do a good job or produce the results the electorate actually wants (which is essentially identical to what is seen in market monopolies—which for example is why American medical care is so expensive yet its results rank last amongst the affluent nations).
On one hand, we have this at a national level, as (at least until Trump’s recent political insurgency) legislators from both parties will consistently vote to spend trillions on abhorrent foreign wars or bank bailouts while simultaneously refusing to support basic necessities that benefit most of the populace. This video for example synopsizes an extensive 2014 study which found public opinion had no influence on the likelihood a bill would become law, and rather, a law passing is entirely dependent upon what the upper class and business interests want.
On a state (and frequently on a municipal) level, we see a similar situation where once one political party becomes entrenched, there is no longer an incentive for them to “do their jobs” and things gradually fall apart as individuals who fail to fulfill their duties (but appease the lobbyists) continue to be re-elected solely due to their party affiliation.
California is particularly known for this issue, as Democrat candidates are typically selected from within the party rather than on merit. For example, Tucker Carlson recently broke down how Kamala Harris had an atrocious performance record, but due to favoritism kept on being promoted within the party and likewise, it’s an open secret that California’s political leadership has often been sourced from four intertwined San Francisco families (e.g., the Newsoms and Pelosis).
On one hand, this has led to the state adopting abhorrent policies that caused many to leave the state (in fact, since 2020, California has been the state with the highest rate of residents choosing to leave). These policies included widely opposed childhood vaccine mandates in 2015, lengthy COVID-19 lockdowns, a poorly worded law banning doctors from discussing COVID vaccine dangers with their patients—which courts later struck down as unconstitutional, or schools concealing children’s gender transitions from parents—which caused Musk to pull his businesses out of California after he could not change Newsom’s mind about that law).
On the other, it’s led to numerous catastrophic bungles which collectively have resulted in higher taxes (California currently has the highest tax rates) and it being harder and harder for residents to stay in the state.
For instance, one of the best known examples is California’s “bridge to nowhere” a project conceived after it was recognized a high speed rail linking the North and Southern parts of the state together would yield tremendous economic benefit. However, unlike China (which has built over 6000 miles of railway in 7 years at a rate of 24.6-48 million per mile), California since 1982 has spent over 23 billion dollars on its high speed rail project, but other than a few unconnected bridges totaling 0.3 miles, no track has yet been laid for it, and despite immense political pressure to finish it, the railway is likely at least 10 years away from the initial parts becoming operational.
Another is California’s recurring wildfire problem. Essentially, due to California’s climate, wildfires are a regular issue. However rather than adopting policies which can prevent these fires from becoming catastrophic (e.g., controlled burns, forestry management, making sure communities have sufficient firefighting water infrastructure or fixing the power lines) more and more money has gone into suppressing the wildfires (which in turn has caused the subsequent ones to burn even hotter).
As such, devastating fires are becoming more and more common, but despite an uproar each time for steps to be taken so the next one does not create profound devastation, nothing gets done and a worse one follows (while spending on wildfire fighting services continue to spiral out of control).
For instance, journalists in the last 24 hours highlighted that:
•Many of the affected communities ran out of water to fight these fires (e.g., the fire hydrants went dry).
•Planned controlled burns had been cancelled.
•Power lines were not de-energized.
•In 2014, a proposition set aside billions develop a water infrastructure for California, yet despite repeated pushes to do so (e.g., from the Trump administration), nothing was ever developed.
•Many home insurance plans in California were recently cancelled due to California enacting laws that capped the prices insurers could charge (hence making it unaffordable for them to offer coverage and insurers simply leaving the state). As a result, many of the homes which burn down likely will not be covered and simultaneously, California’s much more costly state insurance program may collapse from the costs of these fires.
•Los Angeles recently made large cuts to the firefighting services to spend more on homelessness and had shifted its focus from firefighting to promoting DEI.
Likewise, throughout this fire, a common complaint has been that flammable brush that should have been cleared (and was largely responsible for the current fire) never was removed due to poor management by the city and excessive environmental regulations. Now consider this 2009 article:
LOS ANGELES — Federal authorities failed to follow through on plans earlier this year to burn away highly flammable brush in a forest on the edge of Los Angeles to avoid the very kind of wildfire now raging there, The Associated Press has learned.
Months before the huge blaze erupted, the U.S. Forest Service obtained permits to burn away the undergrowth and brush on more than 1,700 acres of the Angeles National Forest. But just 193 acres had been cleared by the time the fire broke out, Forest Service resource officer Steve Bear said.
The agency defended its efforts, saying weather, wind and environmental rules tightly limit how often these “prescribed burns” can be conducted.
Bear said crews using machinery and hand tools managed to trim 5,000 acres in the forest this year before the money ran out. Ideally, “at least a couple thousand more acres” would have been cleared.
Obtaining the necessary permits is a complicated process, and such efforts often draw protests from environmentalists.
Biologist Ileene Anderson with the Center for Biological Diversity, an environmental organization, said burn permits should be difficult to get because of the potential damage to air quality. Clearing chaparral by hand or machine must be closely scrutinized because it can hurt native species.
“Our air quality, for a variety of factors, doesn’t need to be further reduced by these controlled burns,” she said.
Similarly, in Maui, some of the key issues that led to the 2023 fire were years of neglected brush management (despite everyone warning brush around power lines could spark wildfires), the power lines not being turned off during high winds, neglected infrastructure which caused the fire hydrants in Lahaina to run dry (which has also happened in the recent Los Angeles fires), evacuation routes being blocked by bumped to bumper traffic (due to poor advice from police) and a failure to sound the warning sirens (which led to people not evacuating).
What many do not know is that in 2018, a smaller fire ripped through Lahaina, where concerned residents identified all of these issues, but nothing was ever done to address them (and remarkably, the official report about the 2018 fire failed to even mention any of it).
In turn, I (and many others) believe that if there was any type of accountability (e.g., the other party getting elected after repeated gross failures by the ruling party) these types of things would not happen. Unfortunately, Hawaii, like California, is effectively under Uniparty rule so nothing has ever been done (and to the best of my knowledge, the Lahaina fires did not change things in Hawaii either).
Breaking Points
Most of the systems in our society run well when kept a bit below their capacity, but rapidly start to fail ones overloaded (e.g., too many cars rapidly turn a fast highway into gridlocked traffic). One of the most common themes which occurs in natural disasters is that contrary to what’s promised, once the disaster happens, systemic failures begin to emerge which cannot be effectively addressed by the government.
For example, after the recent devastating hurricanes hit the East Coast (and particularly Western North Carolina), many became trapped and isolated, supplies rapidly ran out, and the expected help from the government never materialized. In fact, even after extensive media coverage of their needs and months of time for FEMA to respond, many survivors are still struggling with housing. Likewise, as I showed in here, an almost identical situation exists for the victims of the Lahaina fires.
Much of this is due to corrupt disaster responses from the government which prioritizing paying off preferred relief suppliers rather than helping those in need. As such, in those situations, individuals typically have to rely upon the community and private donations for help. Remarkably however, in disaster after disaster (e.g., in a recent article I highlighted this trend as far back as Hurricane Katrina), not only does the government fail to provide basic aid to these areas, but it actively blocks private aid from getting there (which in turn requires people who want to help having to come up with elaborate ways to bypass the blockades like covertly doing so by boat).
From all of this, I argued three key lessons must be recognized:
First, to some extent, you need to have a way to take care of your basic needs if the grid fails. For example, one of the factors I took into consideration when picking what I believed to be the healthiest water filtration option on the market (discussed here) was if I could use it in a disaster situation where clean water was not available (as this happens quite frequently—e.g., after the recent hurricane). Likewise, my system of medicine has been heavily influenced by not wanting to be dependent on the medical system (as supply shortages regularly happen), so I’ve been gradually introducing the items I always carry with me (e.g., DMSO) that make it possible to address the majority of issues you will run into (along with a few less portable ones like ultraviolet blood irradiation that can often prevent a patient from requiring a hospitalization).
Second, there is a human tendency to not want to believe something bad could happen and then hence repeatedly put off proactively addressing it (e.g., California and Hawaii’s government not fireproofing high risk areas).
Similarly, in most catastrophic situations I’ve studied over the years, a window existed to leave early on which then later closed or became gridlocked once everyone tried to take the necessary steps to protect themselves. For instance, in Lahaina, many were trapped because they did not leave in time (and the main road out was blocked by police) while in the current fires, many had to abandon their cars and walk out because the roads were clogged with traffic (which subsequently required bulldozers to push the abandoned cars out of the way for firetrucks).
Third, once breaking points emerge, many other things will often go wrong many did not expect. For instance, this was recently shared by one prominent Conservative influencer:
A friend of a friend in West LA just saw looters plunder her evacuated house on her Ring camera. Her friends, including some who voted for Harris, are calling for summary execution of the looters. Turns out, “In This House We Believe” politics disappear when your house does.
Like many others who have spoken out against the egregious pharmaceutical overreach during COVID-19, I believe the most viable solution is to develop local community networks which do not rely upon the predatory system we exist within for life essential resources (e.g., my focus has been on effective treatments that can be obtained outside of the medical system and many others have focused on how to locally source healthy food). This is because restricting the access to those life essential resources has always been one of the key ways we are controlled (and forced to accept very poor versions of those essential resources), so once we no longer “need” them, it creates the economic pressure to produce high quality versions that are affordable to the general populace.
Similarly, one of the most valuable resources we have around us is our community, but unfortunately due to the divisive political messaging we are continually bombarded with and all the things in our society which pressure us to be isolated from each other (e.g., by not being able to speak your mind at work and being encouraged to spend your free time in front of a screen), we’ve been disconnected from all of those we should be seeking out. In turn, what really struck me about the events which transpired in both Lahaina and North Carolina was that (due to the culture of each area) the local community came together to help each other as the government abjectly failed the citizens there. In many ways I felt this was the most important lesson of each event as its serves as a model for what we need to be able to do in the future, and ideally, have in place long before a breaking point is hit.
Wildfire Toxicity
Whenever a wildfire (or another event which releases a significant amount of aerial toxicity such as the twin towers collapsing on 9/11) occurs, we regularly see a significant number of people develop longterm illnesses from inhaling that smoke. Furthermore, individuals who already have sensitivities (e.g., from chronic inflammatory diseases) tend to become significantly worse after these events happen.
Because of this I typically advise doing one or more of the following:
•Leave the area until the fire is over.
•Try to stay inside.
•Wear an N-95 mask or respirator while outside.
•Consider getting a filter for your house (e.g., a decent HEPA filter) that can filter out the smoke particles.
When working with chronic inflammatory illnesses, there are two critical points to understand:
•Everyone has a toxicity threshold. Before that threshold, their systems can essentially compensate for the stresses already on them and new ones added on later. However, once they pass the threshold, symptoms rapidly develop, tiny additional stressors can significantly increase their symptoms, and it can become very difficult to walk them back to where they were before they passed that threshold. Two common (but not the only) things that push patients past this threshold are impaired fluid circulations (e.g., due to poor zeta potential) and impaired detoxification pathways.
This dynamic can be analogized to "the straw that broke the camel's back." This concept also applies to many other ailments (e.g., ones that are unrelated to inflammation), but sadly this entire concept is relatively unknown in medicine.
•When an inflammatory illness passes that critical threshold, it disproportionately affects the weaker points in the patient's system (which will also typically be where their symptoms initially arose, something which for example has frequently been observed after COVID vaccine injuries).
With those exposed to wildfire smoke, colleagues and I have observed the following concerning issues tend to occur:
•Existing circulatory disorders often worsen.
•Patients with pre-existing chronic and complex inflammatory illnesses (e.g., chronic fatigue syndrome, mast cell activation syndrome, or Lyme disease) tend to be the most susceptible to becoming ill from the smoke, especially if their system was already caught in an inflammatory loop. When this happened, we frequently observed acute exacerbations of their pre-existing illnesses, something also observed in these patients after they were vaccinated (e.g., patients with chronic Lyme disease often had their disease worsen after COVID-19 vaccination).
Note: This entire situation is analogous to one of the most common side effects of the COVID-19 vaccines: either a new autoimmune disorder or a worsening of a pre-existing condition. To illustrate—an Israeli study found that 24.2% of those receiving a booster developed an exacerbation of a pre-existing autoimmune condition.
•Some people (enough that you will come across them but not enough that it's a commonly recognized issue) develop chronic illnesses (e.g., long-term fatigue) after the wildfires. I have also noticed other people's health worsened, but those changes were minor enough that they typically were unrecognized.
•A doctor I spoke to who specialized in these complex illnesses and treated numerous people during the California wildfires stated that he saw this condition predominantly affect patients he described as "being on the edge." In those patients, the wildfires tipped them over the edge as their detoxification and anti-inflammatory pathways got overwhelmed, or to quote my colleague: "It's all susceptibility. If your body has been compensating and you get this big inflammatory trigger, wherever you are going to trigger is whatever the weakest spot is in your body."
•The earlier you begin treating the wildfire illness, the less long-lasting the effects will be. Similarly, the sooner you get away from the smoke, the less likely the issues are to become permanent (many patients got better once they left the area). The reason why the 2017 and 2018 wildfires in California were so problematic was that, from my colleague's perspective, they went on forever, so there was enough time to tip patients past their critical threshold. Because of all the unhealthy influences in our environment (e.g., processed foods that create chronic illness), Americans already have numerous stressors on them. As a result, my California colleague often saw something like a divorce or losing a job being the straw that broke their back and thought it was sad to see how often the California wildfires also ended up being that final straw.
•For younger people, the biggest wildfire issues were breathing conditions they were already on their way to developing (asthma and COPD being the most common). For older patients (those in their 60s, 70s, and 80s), the most significant issues were cognitive issues (e.g., my colleague had numerous patients receiving long-term treatment for their cognition who became significantly worse after the systemic inflammation triggered by the wildfires). Heart attacks and strokes could also occur in those predisposed to them.
Note: there is quite a bit of research showing particulate exposure causes cognitive impairment in all ages and accelerates the progression toward Alzheimer's. Much of this data was gathered in Mexico City when evaluating nano-particulates that are less than 2.5 microns in size. For those interested to learn more, consider reviewing this study, this study, this study, and this study.
Health Effects from Fires
After the Lahaina fires occurred (putting many through extremely traumatic situations I detailed here), Hawaii decided to comprehensively study the health effects on the survivors (which is fairly unusual). This unique dataset in turn provides some helpful insights for what those in Los Angeles may experience in the coming years.
That study found that six months after the fires:
•Only 24% of the participants remain in their pre-wildfire homes, 65%, are in temporary homes (e.g., hotels), and 11% have moved to new permanent homes.
•58% lost their jobs, 24% are still jobless and searching and 74% reported a drop in their household income. Additionally, 35% of households reported difficulties having enough food for the family (compared to a baseline of 20.5-23.7%).
•49% said their health is now worse than it was prior to the wildfires, 24% reported that they do not have steady access to medical care and 13% reported not having health insurance (compared to 1.7% of Maui residents being uninsured in 2022).
•Over 20% had elevated blood pressure, 8-18% of participants had blood work indicating compromised kidney function and up to 74% of participants had signs of poor respiratory health (49% exhibited signs of mild to severe lung obstruction, and 33% had compromised lung function linked to impaired tissue oxygenation).
Note: lung injuries often follow wildfire smoke exposure, but this is first time I’ve seen the extent of this problem quantified. Presently, I believe many of those issues result from the positively charged smoke particulates destroying the glutathione lining of the lungs, injuring the endothelium and impairing the physiologic zeta potential.
•55% reported depressive symptoms (compared to a baseline of 33%), with the rates increasing with age (e.g., depression was reported by 75% of those between 50-59 years old). Additionally, 34.6% reported low self-esteem (compared to a 13-14% baseline) and 1.3% reported suicidal thoughts compared to a 0.8% baseline). Finally the majority of respondents reported anxiety, but no comparative baseline was provided.
•The participants reported that they found community aid organizations to be more helpful than FEMA, state aid agencies or county aid agencies.
In the University of Hawaii’s most recent data release, they found that the majority of the fire survivors were experiencing significant symptoms (associated with wildfire smoke exposure) at least once a month and that the majority (60.4%) had not received medical attention for their symptoms.
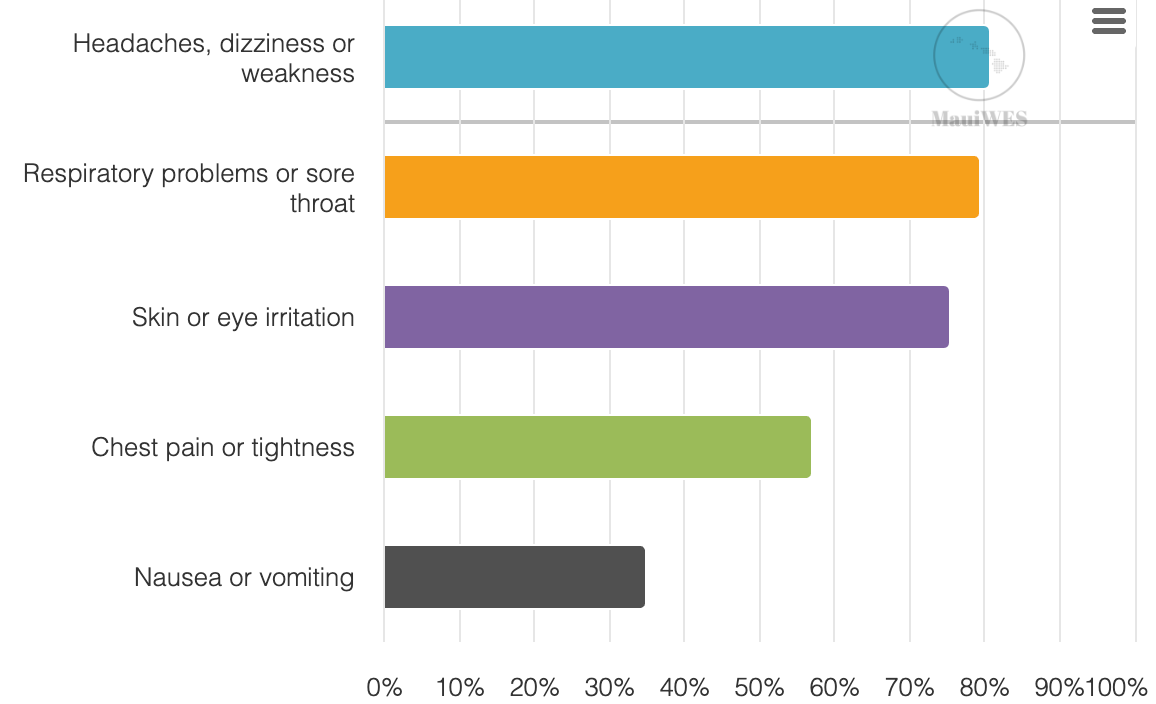
Note: a few months later (in a subsequent update of the report) the physical health outcomes stayed the same but the mental ones worsened (e.g., 30% of participants reported symptoms of moderate or severe anxiety and 4.4% had suicidal thoughts). Likewise, years after, many are still struggling with finding housing (with many families simply leaving Hawaii).
Why Do Wildfires Make People Sick?
I have seen three different models that explain why the smoke from wildfires makes patients ill.
The Kendrick Model
Malcolm Kendrick has made a convincing argument that heart disease arises from inflammatory or mechanical damage to the protective lining of the blood vessels (the endothelium). This then requires blood clots to form to patch that damage, and over time, those clots transform into the atherosclerotic plaques classically associated with heart disease.
Because of this, he believes factors that damage the endothelium are the primary cause of heart disease and argues for reducing them in parallel to providing factors that protect the endothelium and supports its production of nitric oxide (which dilates the blood vessels, allowing adequate blood supply to the body). One of the noteworthy things about COVID-19 is that the spike protein excels at creating the vascular damage that Kendrick has long argued causes heart disease and strokes.
Note: Kendrick's model also considers stress to be a primary contributor to heart disease.
One of the things that is known to increase the risk of heart disease is exposure to particulate matter. Kendrick, in turn, argues that this is due to the particulates damaging the endothelium. The pieces of evidence he collected to support this hypothesis were as follows:
•A study of 378,256 patients in general practices used AI to determine what diseases were the most likely to predict future risk of cardiovascular disease (CVD). It found that the greatest risk factors were COPD (66.3% developed CVD within the next ten years) and atrial fibrillation (67.8% developed CVD within the next ten years). Many would assume the COPD risk was due to COPD frequently resulting from smoking (which causes heart disease), but in the case of smoking, only 53.3% of smokers developed CVD within ten years. Kendrick interpreted this to mean that chronic inflammatory damage to the lung endothelium also damaged the rest of the endothelium in the body, thereby supporting his hypothesis that endothelial damage was the cause of heart disease.
•Coal miners (who repeatedly breathe in coal dust particulates) have a significantly increased risk for heart disease, and depending on how much coal they are exposed to, their risk of dying from it increases by approximately 50 to 100 percent. Since most coal particles are too big to enter the bloodstream, this risk likely is from the smaller nanoparticles that can. This link was further supported by the 2015 study "Subchronic inhalation of particulate matter 10 coal dust induces atherosclerosis in the aorta of diabetic and nondiabetic rats."
•The nanoparticles released into the bloodstream from smoking immediately damage the endothelium and triggers blood clots:
Brief active smoking of one cigarette generated an acute release of EPC [stem cells that replace dead endothelial cells] and MPs [remnants of dead endothelial cells] of which the latter contained nuclear matter. Together, these results demonstrate acute effects of cigarette smoke on endothelial, platelet and leukocyte function as well as injury to the vascular wall.
Vascular dysfunction induced by smoking is initiated by reduced nitric oxide (NO) bioavailability and further by the increased expression of adhesion molecules and subsequent endothelial dysfunction. Smoking-induced increased adherence of platelets and macrophages provokes the development of a procoagulant and inflammatory environment.
•This same process appears to occur in individuals who breathe in particulate matter generated from the combustion of fossil fuels:
There is a proven link between exposure to traffic-derived particulate air pollution and the incidence of platelet-driven cardiovascular diseases. It is suggested that inhalation of small, nanosized particles increases cardiovascular risk via toxicological and inflammatory processes and translocation of nanoparticles into the bloodstream has been shown in experimental models…this study provides a potential mechanism for the increased thrombotic risk associated with exposure to ambient particulate air pollution.
•This same process also occurs following the combustion of forests. Consider the results of one of the largest studies (published in 2015) evaluating the effects of wildfire illness:
Smoke exposure was associated with increased rates of ER visits, not just for breathing trouble, but also ischemic heart disease, irregular heart rhythm, heart failure, pulmonary embolism and stroke. The risk was greatest for adults age 65 and older.
The greatest increased relative risk was noted within a day of dense wildfire smoke. During these times, researchers found rates of ER visits among adults 65 and older increased 42 percent for heart attack and 22 percent for ischemic heart disease.
Overall, ER visits for all cardiovascular and cerebrovascular causes were elevated across all smoke days, with the greatest increase on dense smoke days and among adults age 65 and older. Respiratory conditions also were increased, as anticipated.
The Klinghardt Model
Dietrich Klinghardt is considered by many to be one of the pioneers in the integrative medical field and has treated many challenging patients with complex illnesses over the decades.
Like many, Klinghardt views chronic illnesses as often resulting from a confluence of factors that need to be addressed (e.g., EMFs, root canals, surgical scars dysregulating the autonomic nervous system, heavy metals, and unresolved generational conflicts in your family—all of which my mentors and I have also observed to be amongst the most common causes of chronic illness). Since Klinghardt focuses on heavy metals, he frequently emphasizes treating them before directly treating a chronic infection as he believes the infection (e.g., candida) is a compensatory response to that metal overload.
When the wildfires happened, Klinghardt proposed that much of the toxicity we were seeing came from the fact that the trees gradually stored heavy metals in the environment and were expelling them into the environment by being burned. Thus, we were effectively giving a gradual but continual heavy metal exposure to people whose systems were already near their critical threshold.
I asked my California colleague if they agreed with Klinghardt's assessment. They did, but acknowledged they did not have patients where they tested heavy metal levels before and after the fire. They also added that due to all the previous mining in California (e.g., a lot of mercury was used for gold extraction), the trees have a significant heavy metal burden. Furthermore, they directed me to examine the EPA's own research showing that wildfires disperse mercury in the environment. This is exactly what the science has found, especially during the hottest wildfires.
Note: my colleague also believed some of the fire's toxicity came from all the human structures (e.g., houses) that burned down and dispersed their contents into the atmosphere. I also suspect many of these buildings were old enough to have had various now-banned building materials like asbestos and lead paint (additionally, Kendrick has made a strong case lead being aerosolized from combusting leaded gasoline used to be one of the primary causes of heart disease in America due to how lead particles damage the endothelium).
Negative Ions and Zeta Potential
In this publication, I have tried to emphasize that fluid stagnation created by impairments of the physiologic zeta potential (the electrical charge that is responsible for ensuring the dispersion of colloidal systems like blood) is one of the primary causes of illness.
A now forgotten book, The Ion Effect, details how a great deal of evidence showed that:
•Weather patterns that flood the environment with positive ions are often highly detrimental to human physical and mental health.
•There was a great deal of evidence negative ions produced a wide range of health benefits and that many of those benefits (e.g., for burns and breathing) mirrored what one would expect from local improvements of zeta potential at locations where the negative ions contacted surfaces of the body. Given that the physiologic zeta potential relies upon negative charges to ensure a sufficient colloidal dispersion, it should hence make sense why negative ions in the air enhance it while positive ones worsen it.
My overall sense from observing both wildfire illnesses and COVID-19 is that the diseases initially enters the airway tract (where it creates symptoms correlating to blood stasis resulting from the positive ions present impairing zeta potential) and as it penetrates deeper, enters the lungs, then the smallest blood vessels lining the lungs, and finally the larger vessels of the body. In turn, you can observe people at each stage of this progression, and individuals who have a chronically impaired zeta potential (e.g., the complex patients with chronic inflammatory conditions my colleague saw) are typically the most vulnerable to wildfire exposure as they are already further down that pipeline—much in the same way those patients were also the most vulnerable to spike protein injuries (a COVID-19 infection or a vaccine reaction).
Note: one of the many side effects of positive ions was that they slowed the movement of the cilia (tiny beating hairlike structures), which the respiratory tract uses to clear particulate matter from it. Tobacco smoke plus positive ions was found to slow their movement by 3 to 10 times, whereas subsequent exposure to negative ions reversed this suppression of the cilia.
Treating Wildfire Injuries
There are a few approaches I and colleagues have observed help with the treatment of wildfire injuries. However, before I detail them, I must emphasize that the most critical thing is to get out of the area where the wildfire smoke is present or, if that is not possible, to do everything you can to mitigate your exposure to them, especially if you have a pre-existing vulnerability to the smoke. Additionally, the earlier these treatments are done (just like with treatments for COVID-19), the more effective they are.
The approaches we have found to be helpful are as follows:
•Do treatments that restore the physiologic zeta potential of the body. Additionally, one aspect of restoring zeta potential is drinking deionized water (distilled or reverse osmosis water), and having a sufficient amount of that water seems to be particularly important when addressing wildfire injuries.
•Intravenous Vitamin C (when administered early, it greatly helps with wildfire-induced inflammation).
•Treatments directed at the obstructions in the lungs.
•Treatments directed at treating the underlying chronic inflammation in the patient (e.g., what existed before the wildfire smoke exposure).
•Nebulized Glutathione.
•DMSO (e.g., after sheep experienced a lung injury from inhaling smoke, nebulized DMSO with heparin was found to reduce the damage to their lungs significantly).
Note: I have very little experience using DMSO to treat wildfire injuries (our preference is to use nebulized glutathione). However, as I showed in this article, DMSO works on both burns and a variety of related lung disorders (which nebulized glutathione also treats), so it very likely DMSO would help for wildfire toxicity too.
Pulmonary Glutathione
Glutathione, a powerful antioxidant, is one of the primary mechanisms the body uses to protect itself from toxins (e.g., heavy metals and free radicals) and is a commonly used therapeutic within integrative medicine for a variety of illnesses. One of the things that is not very well appreciated is that the lungs depend upon glutathione to protect themselves from damage (along with maintaining the survival of the lung cells), and thus concentrate glutathione at the interface where oxygen in the airway enters the circulation. Likewise, in chronic lung diseases, its presence is diminished:
Alterations in Glutathione in Lung Injury Studies show that the glutathione in epithelial lining fluid of the lung is altered in response to disease. Epithelial lining fluid in healthy volunteers show glutathione concentrations to be greater than 400 μM, placing epithelial lining fluid among the highest reported for any extracellular fluid…In cell studies on the toxicity of tobacco smoke, N-acetylcysteine [the precursor for glutathione which is also successfully being used to treat spike protein injuries] substantially increased survival of cultured human bronchial cells during exposure to cigarette smoke condensates. The glutathione in epithelial lining fluid from patients with interstitial pulmonary fibrosis was fourfold lower than in healthy patients.
Note: the article quoted above also discusses how exposure to an irritant causes glutathione to at least temporarily increase in the lungs and that reduced lung glutathione levels are seen in many other diseases like ARDS, pulmonary fibrosis, cystic fibrosis, and HIV.
One of the most common causes of death in the United States are chronic diseases of the respiratory tract (COPD being the most common). Before COVID-19, it was the 4th most common cause of death in the United States, but since then, strokes and COVID-19 (or things misdiagnosed as COVID-19) have edged it out. Because of how many people have COPD (e.g., it is a common consequence of smoking), therapies directed at COPD are one of the largest drug markets (the global asthma and COPD market is currently valued at 36.7 billion and expected to reach 60.3 billion by 2032). Unfortunately, they need to be taken indefinitely and don’t prevent the inevitable progression and horrible death many ultimately experience from the disease.
Given how much money is at stake with “treating” COPD, it should come as no surprise that almost no awareness exits that nebulized glutathione can treat it (e.g., see this case report and this review of it being used for other obstructive lung conditions).
Note: we find nebulized glutathione is one of the most helpful treatments for COPD, but typically, it can only halt the progression of the disease rather than reverse it (although as this case report shows, the results can sometimes be dramatic during a COPD exacerbation). As such, we try to start it as early as possible. Conversely, as I showed in this article, DMSO can treat a variety of severe acute and chronic lung diseases.
Nebulized Glutathione
Each time a wildfire breaks out, and patients get ill, a few integrative doctors and naturopaths in the area will promote using nebulized glutathione to treat wildfire illnesses. My colleague, for example, who utilized it for the 2017/2018 wildfires, told me it worked, especially when given early in the disease process. They also noted that many of their patients who were injured by the wildfire injuries were also patients they knew had previously had borderline or iffy glutathione levels (e.g., due to another issue preventing glutathione production).
Additionally my colleague also warned me that in a specific subset of patients (due to existing sulfur sensitivities), prostaglandins are released by nebulized glutathione, which can trigger asthma or other lung conditions in susceptible individuals (my colleague in turn has many very sensitive patients in their practice). For this reason, even though this procedure can be done at home, they advised doing the first administration in the office to monitor for this.
Note: another colleague in the Midwest has also found glutathione works for wildfire illnesses, but due to his location, like me, he does not see anywhere near as many of these patients. Since we have less experience with the wildfire issue, I would like to share this comment on an earlier article about wildfire toxicity from a California doctor (I verified) who utilized nebulized glutathione:
Lastly, many other uses for nebulized glutathione. For example, a common source of severe pharmaceutical injuries are fluoroquinolone antibiotics (which I hence believe should only be used as a last resort rather than routinely for things like urinary tract infections). In many cases, individuals who have been “floxed” by a fluoroquinolone struggle for years with their illness and hence try a wide range of things to treat it. In turn, I’ve spoken to numerous floxed individuals who found nebulized gluathione greatly helped some of their heart and lung symptoms.
Sourcing Nebulized Glutathione and DMSO
When I first started this publication, I made a decision to avoid promoting specific supplements as I felt for the mission I’d set out to do (bringing forth useful information that could directly help many) should not be obscured by any potential conflicts of interest. Once I realized I needed to provide a few (as otherwise it would not be feasible for many to implement the suggestions I’d provided), I ran into a new issue—I would frequently create supply shortages of the supplement and hence make it impossible for many of those here to obtain it (e.g., despite my best efforts to avoid it, I recently caused a nationwide supply shortage of DMSO).
Note: in many ways, this is analogous to the “breaking points” that occur in natural disasters, as much in the same way those systems (e.g., hospitals) are not designed to handle a much higher load and hence fail under stress. A small market exists for many of the forgotten therapies I use, so currently, they can’t be rapidly scaled up to meet a surge in demand.
Because of this, my current approach is to initially restrict who those product recommendations go to, both so that the initial group can get them without everything being out of stock (and hence be able to collect the initial data on their efficacy that can be used by the rest of the community here), but also so that the suppliers, seeing the increased demand, have time to ramp up their production of the supplement.
In the final part of this article, I will review the exiting options for sourcing nebulized glutathione (both for clinicians and those without medical licenses) and its dosing, the same for DMSO (where to obtain it, common protocols for standard uses, and how its used to treat lung conditions such as via nebulization) along with a few other options for treating wildfire illnesses.
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.