

The Perils of Vaccinating When You Are Infected
What the forgotten HPV vaccine tragedy can teach us about the dangers of COVID vaccination

Story at a Glance:
•The HPV and COVID-19 vaccines are two of the most dangerous pharmaceutical products that were ever pushed onto the market. However, regardless of how much evidence of harm emerged, authorities always insisted they were “safe and effective.”
•Many of the issues with both vaccines were a result of those vaccines hyperstimulating the immune system, which in turn created a variety of debilitating autoimmune disorders.
•One of the less appreciated consequences of this hyperstimulation is that if it occurs while someone is infected with the disease, it can make the existing infection become more severe.
•Despite this being clearly shown within the HPV vaccine trials, since testing before vaccination would reduce vaccine sales, it was never recommended within the prescribing guidelines (some groups even said to not test before receiving the vaccine). Likewise, with the COVID vaccines, despite everyone being continuously tested for COVID-19, testing was never advised prior to a vaccination appointment, nor were members of the public informed of the dangers of vaccinating while infected.
Recently, Dr. Kory and I decided to begin tackling one of the most challenging topics with the COVID-19 fiasco—does something about these vaccines cause them to harm those around the vaccinated individual?
In theory, this should not be possible, yet over and over again we are coming across cases where it is happening (the evidence of which has been extensively documented here). Since “shedding” is used to describe the phenomenon where individuals injected with a replicating organism (e.g., the oral polio vaccine) can then make others become sick with the illness the vaccine is supposed to prevent, everyone has settled on referring to this curious side effect of the spike protein vaccine as “shedding.”
Because this is quite a perplexing situation, we’ve spent the last few years trying to come up with a mechanism that could explain how this “shedding” is possible. Recently, I published an article explaining the hypotheses we’ve developed, and presently we believe certain vaccinated individuals exhaling large amounts of spike protein coated exosomes is the most likely mechanism at work.
One of the alternative hypothesis I put forward was that the vaccine is impairing the normal immune response and causing injected individuals to become chronic silent shedders of COVID-19. After publishing the article, I received a lot of questions about a few points I highlighted, particularly readers wanting to know more about receiving an HPV vaccine in the presence of a pre-existing HPV infection. This article in turn will address what can go wrong if you vaccinate while already infected.
The Last Frontier of Medicine
Immunology is frequently referred to as the last frontier of medicine since the immune system is so incredibly complex and at this point, much still remains unknown about it. I personally believe this is because most of the research on it has revolved around trying to find immunological pharmaceutical products (e.g., vaccines or immune suppressing agents) rather than trying to understand the systemic processes that cause the immune system to go awry in the first place (as these are much harder to produce profitable therapies for).
Note: some of the existing immune suppressing agents are incredibly helpful for patients (and relatively safe), but many of the other ones we use in practice are quite dangerous and much harder to justify using.
Throughout this publication, I’ve tried to illustrate how much of medicine only makes sense if you understand foundational business and marketing practices and then see the existing way medicine is practiced through that lens (e.g., much of what constitutes the “standard of care” is only there because it makes money for the industry).
In the case of vaccines I would argue each the following are true:
•A central mythology the credibility of modern medicine is based upon is that vaccines rescued us from the dark ages of infectious disease. As a result, the medical field will almost always have faith each promise of a vaccine is indeed true and simultaneously be astonishingly resistant to the idea any vaccine (and by extension the medical profession) could be bad.
Note: a good case can be made that most of the benefits attributed to vaccination were actually due to the benefits of modern sanitation, as almost all of the decline in disease attributed to vaccination predated the vaccines actually coming into use. Conversely, the forgotten history of many of the early vaccines showed they worsened the diseases they were supposed to prevent and simultaneously injured many.
•Since you can in theory make a vaccine against anything by mixing a target protein with an adjuvant (e.g., aluminum), vaccine development is a very popular area of research—especially because the resulting product (due to the 1986 Vaccine Injury Act) has no liability for injuring people and is often mandated upon most of the country. This for example is why individuals, like Peter Hotez have received over 100 million dollars in research grants—much of which has gone to “developing” a vaccine for a human hookworm infection, despite still not having anything to show for it after decades of work.
•Vaccine research in turn rarely considers the possibility that their target protein or adjuvant might cause problems. For example, one of the longstanding issues with vaccines is that the proteins they try to train the immune system to attack partially match normal proteins within the body, and as a result, autoimmunity is a frequent complication of vaccination (there is even a textbook about this).
Note: one of the major issues with the COVID vaccine is how many different human tissues match the (spike) protein it mass produces within the body, which many suspect is a key reason why the vaccine has such an extraordinarily high rate of causing autoimmunity. For those wishing to learn more, the subject of vaccines and autoimmunity is discussed in more detail here.
•When it comes to vaccines, the same people who constantly espouse the “safe and effective mantra” with an absolute conviction rarely take the time to actually understand exactly what’s going on with the injections and familiarize themselves with the science behind them.
Note: the vaguely defined phrase “safe and effective” is a relatively meaningless marketing slogan which has been repeated over and over for decades because it has proven itself to be a very effective way to sell vaccines.
For example, there had been a longstanding challenge in producing a “safe and effective” live polio vaccine as making the vaccine “safe” required using formaldehyde to deactivate the polio virus, but doing so also destroyed many of its antigens which were necessary for developing an immune response. To address this issue, Salk put forward a theoretical argument for why his vaccine was “safe” that was accepted by the authorities despite Salk failing to provide the evidence for his contention. When his vaccine hit the market (with the dishonest blessings of the government), many were then paralyzed by it. One honest academic, Paul Meier, professor of epidemiology at the Johns Hopkins University School of Public Health, who critiqued the fiasco, provides some important context on the longstanding use of this marketing slogan:
When the Salk poliomyelitis vaccine was released for widespread use in April 1955, and despite assurances of safety, a number of vaccinated children developed poliomyelitis.
No public acknowledgment of the manufacturing difficulties was made at this time [a lot of Polio contaminated vaccine lots were found], but the Vaccine Advisory Committee released a public statement which was concurred in by the Public Health Service, and which, in effect, gave assurances that the vaccine was safe. [The VAC is the same group which has green-lighted every possible use of the COVID vaccines].
All manufacturers had rejected some lots because live virus had been found in them: and therefore Salk's theory that safety was guaranteed by the method of preparation obviously did not apply
Perhaps the most disturbing element of the entire program, has been the disparity between the risks that were known to be involved and the repeated assurances of safety.
The National Foundation, in a memo sent to doctors, also stated emphatically that the [polio] vaccine was completely safe and that the risk of ensuing paralysis was “zero”.
The best way to push forward a new program is to decide on what you think the best decision is and not question it thereafter, and further, not to raise questions before the public or expose the public to open discussion of the issue. [This statement was overview of what happened which was meant to be sarcastic].
Hyperpriming the Immune System
There are a variety of designs for vaccines. Some work by containing only a small number of proteins (antigens) which match the target disease, while others contain a large number of them. Typically, the former are created by mass synthesizing the protein antigen and mixing it with something that provokes a strong immune response (an adjuvant) as this significantly reduces how much of the most expensive ingredient (the antigen) needs to be administered to solicit the desired immune response. Conversely, the latter are created by taking the existing pathogen you want to develop a vaccine against, somehow making it less dangerous, and then injecting that whole pathogen (which thus has dramatically more antigens to vaccinate the person against).
My general impression with vaccines is that the latter (weakened or attenuated forms of the original pathogen) tend to be much more effective than the former at preventing disease and sometimes also have other nonspecific benefits (as they improve the immune system’s ability to fight off other things). Conversely, since these vaccines are a living organism which can replicate, they have the risk of both making the individual become ill and spreading (shedding) the disease into the community (which commonly happens with oral polio vaccine and to a lesser extent happens with the measles vaccine). For this reason, it is always advised that the “live” vaccines are only given to people who are not immune suppressed and that immune suppressed individuals avoid individuals who were recently vaccinated with live vaccines.
Presently, I know of the following benefits (beyond preventing the target infection) which are seen with live vaccines:
•The rabies vaccine being able to treat an existing rabies infection before it becomes fatal.
•The shingles vaccine being able to prevent future shingles episodes in someone who is chronically afflicted by them.
•The imunostimulatory effect of the tuberculosis and measles vaccine reducing the risk of dying from other infectious diseases (which in areas like Subsaharan Africa noticeably lowers the death rate since infectious diseases are such a common killer there).
•The tuberculosis vaccine functioning as a therapeutic for certain cancers (e.g., bladder) and is also currently being tested as a treatment for fibromyalgia.
Note: there are also a lot of problems with live vaccines; I am primarily sharing the above to provide the context for what follows.
When a single antigen is used instead (along with the adjuvant which makes the immune system have a disproportionate response to that antigen), an unnatural immune response is created. Some of the common consequences of that include:
•It rapidly triggers the pathogen to mutate so that it no longer has the antigen sequence in question. This effect is known as “strain replacement” and is a longstanding issue with vaccines (e.g., this is why they keep on having to add new antigens to the pneumococcal vaccine). Likewise, this is why many individuals were able to correctly predict that once the COVID vaccine was released, many COVID variants would emerge which had a different spike protein the vaccine didn’t work on (which is why boosters to each new strain “needed” to be made).
•The immune system becomes permanently locked onto antigen it has been primed to respond to. This becomes problematic since the immune system has a finite ability to respond to things, and as a result, if it locks onto the wrong strain (e.g., one that the vaccine had already made become extinct) it loses the ability to respond to the current threat (which is known as Original Antigenic Sin or OAS).
Note: one of the strongest arguments against the COVID-19 vaccines is that they still contain the spike protein sequence of the original SARS-CoV-2 virus even though that variant is now extinct.
For example, consider the author (mentioned above) who discovered that in areas where people frequently die from a variety of infectious diseases, the live measles vaccine reduced children’s overall risk of death by 38-86%, and the live tuberculosis vaccine reduced the overall risk of death by 37-48% because of a non-specific strengthening of the immune system. That same author also found that the pertussis vaccine (one which hyper-primes the body to respond to a few specific antigens) instead increased the overall risk of death by 293% in boys and 898% in girls as they became more susceptible to dying from a variety of other infections.
Prior to the COVID vaccines, OAS (and negative vaccine efficacy) had been most frequently seen with the influenza vaccine (e.g., see this review, this study, this study, and this study). However, the most tragic (and well documented) results have been seen with the spike protein vaccines, best shown by this study:
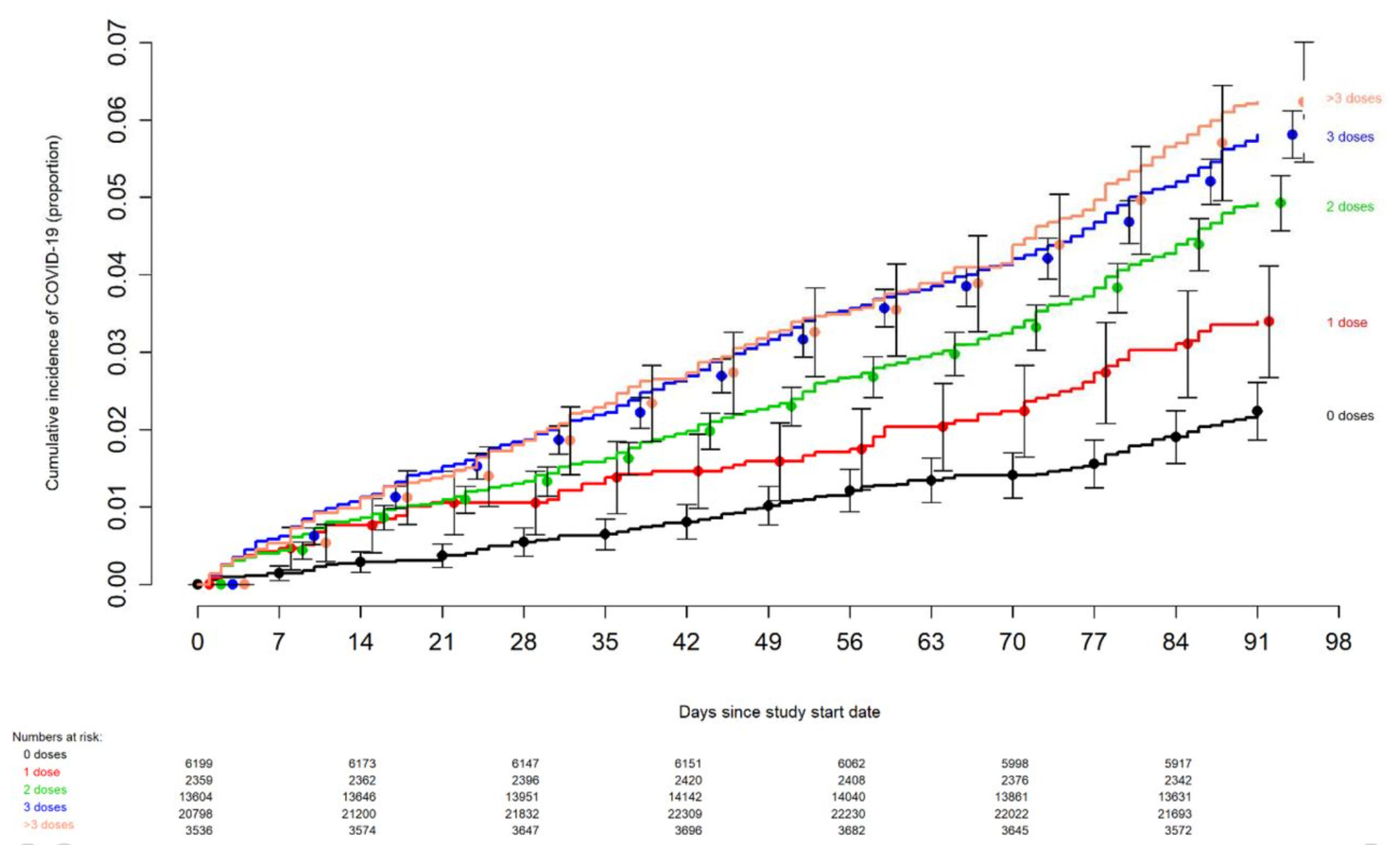
Note: there are other mechanisms besides OAS which may also explain why individuals who got the COVID vaccine keep on getting COVID.
•For certain diseases, the harm of the disease is a result not of the infectious organism but rather an overactive immune response damaging the body as it tries to eliminate the disease (e.g., rheumatic fever arises from the immune system attacking a critical valve of the heart as it attempts to eliminate a streptococcal infection). One of the major issues with adjuvants is that they don’t just provoke the immune system to attack the target antigen—they also provoke it to do a lot of other things you don’t necessarily want it doing. For example, one study showed that exposing mice to a pertussis vaccine (and its adjuvant) will cause them to also develop allergies to the currently circulating pollen.
Let’s now look at how these principles come into play with the two most dangerous vaccines on the market.
Note: the anthrax vaccine and the smallpox vaccine are also extremely dangerous but neither is currently given to the general population.
The HPV Vaccine
Note this section and much of what follows were sourced from the excellent book The HPV Vaccine on Trial which I have quoted with the author’s permission.
Prior to the COVID vaccines, I believe the most aggressive vaccine marketing campaign I’d ever seen was for Merck’s Gardasil and I was astonished to see how many girls quickly became deathly afraid of a cancer which had already been mostly eliminated with routine pap-smears (which were first introduced in the 1940s).

This campaign was motivated by Merck’s realization being able to sell a vaccine for cancer (given how much fear exists around cancer) could be incredibly lucrative since that would allow a massive markup and the vaccine could be sold to almost everyone.
Since so much money was on the line, this in turn necessitated ensuring everyone believed their product was safe and effective. To create this mythology, Merck essentially had to do the following:
•Cover up the unprecedented number of severe injuries which occurred in the clinical trials.
•Get the CDC and FDA to bend over backwards to protect the vaccine once the vaccine hit the market and a deluge of injuries were reported to them.
•Convince the world that the primary cause of cervical cancer was a chronic HPV infection (when in reality a variety of factors like smoking played a key role in it) and that producing an antibody response to an HPV antigen would prevent HPV and in turn would prevent cervical cancer.
Note: it’s hard to put into words how awful the trials for Merck’s HPV vaccine were. Since they represent the closest case precedent to what happened in the similarly atrocious COVID-19 vaccine trials, I wrote an article describing exactly what happened to the HPV vaccine trials.
One of the major problems with developing the HPV vaccine was that it was quite difficult to provoke the body into developing an immune response to its HPV antigen (which I suspect was because that HPV antigen had too much of an overlap with human tissue—something which was also the case for the COVID-19 vaccine). In turn to solve this (e.g., to overcome the body’s resistance to attacking antigens which resembled its own tissue), Merck had to use a very powerful adjuvant, which in turn led to a very high level of autoimmune complications from the vaccine.
For example, in Merck’s trial data, they disclosed to the FDA that 49.6% of vaccine participants developed a “New Medical Condition,” (many of which were likely quite severe), 2.3% of which Merck admitted were autoimmune disorders. Additionally, the participants died at 2-5 times the normal death rate typically seen in the age group.
For reference, this is what is stated in Merck’s package insert for the vaccine, which discussed all the (reported) autoimmune disorders which developed throughout its clinical trials.
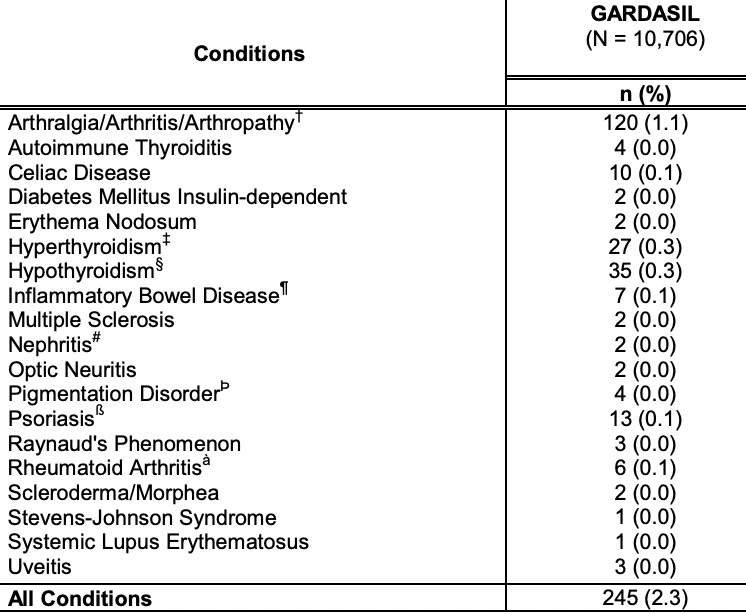
In turn, some of the autoimmune disorders which have been linked to Gardasil since it hit the market include Guillain – Barré syndrome, other demyelinating neuropathies (multiple sclerosis, MS; acute disseminated encephalomyelitis, ADEM; transverse myelitis, TM), postural orthostatic tachycardia syndrome (POTS), systemic lupus erythematosus (SLE), pri- mary ovarian failure (POF), pancreatitis, vasculitis, thrombocytopenic purpura, and autoimmune hepatitis.
Note: one of the most common side effects of Gardasil was POTS (severe lightheadedness when standing up, a debilitating disorder which can sometimes trigger fatal car accidents—and which coincidentally were a common cause of death in the Gardasil trials). Many have since concluded this disease was in part an autoimmune disorder as Gardasil victims have been found to have antibodies to the autonomic receptors which are supposed to bring blood to the head (see this article, this case study and this case study), As you might have noticed, POTS never appeared in Merck’s list of reported autoimmune disorders. I will also note that I believe to some degree, POTS appears to be due to an impaired zeta potential (something Gardasil was also notorious for doing), as restoring the physiologic zeta potential often significantly improves POTS.
Negative HPV Vaccine Efficacy
One of the most remarkable effects of the HPV vaccine was that its own trials showed it caused cervical cancer if someone was already infected with a vaccine covered HPV strain at the time of vaccination (specifically it increased the risk by 44.6%—something which is known as “negative vaccine efficacy”). Since HPV “causes” cervical cancer by creating chronic inflammation within the cervical tissue, my best guess is that this was a result of the immune system being provoked into creating more inflammation at the site of an existing HPV infection.
Note: alternatively, it may have been a result of the immune system losing its ability to keep the chronic HPV infection under control because it was diverted to addressing the vaccine antigen.
Let’s look at exactly what Gardasil’s trials found:
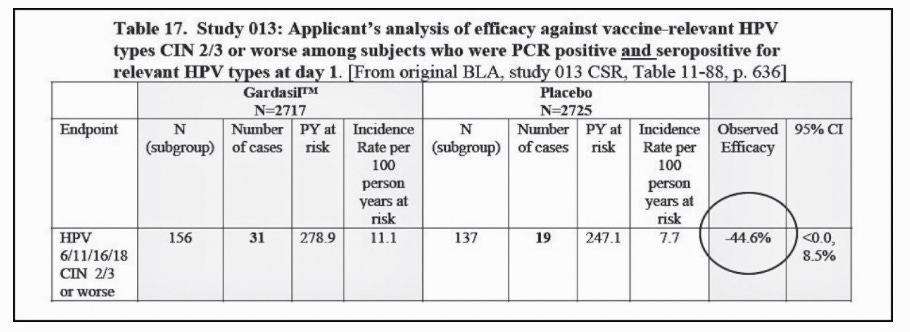
Note: PCR positive means the virus is currently present in the system and can be detected. Seropositive means that antibodies to the virus are present in the blood, which can either indicate a current infection or that there was a previous infection the immune system eliminated (which commonly happens with HPV).
Since that was a bit concerning, Merck looked for a way to lower this negative efficacy, which was accomplished by changing the criteria from “and” to “and/or:”
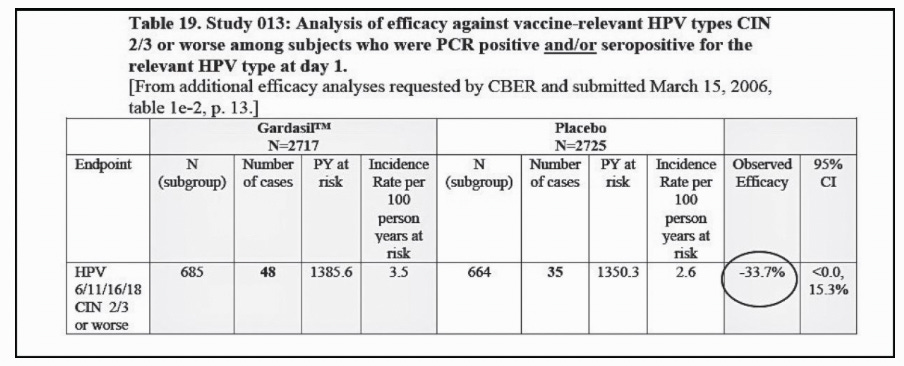
This in turn lowered the negative efficacy by about 25%, but nonetheless still was a fairly concerning amount. What appears to have been missed by the regulators was that this second data set strengthened the case that the HPV vaccine causes cervical cancer (in the context of a pre-existing infection) since being “PCR positive and/or seropositive” signifies a less active (inflammatory) immune response against an active HPV infection than being “PCR positive and seropositive” and in turn the negative efficacy was observed but to a smaller degree. This ties into the well known fact that a dose-response relationship is a classic criteria for determining causality.
Note: I also uploaded the full copy of this report in case the above link stops working.
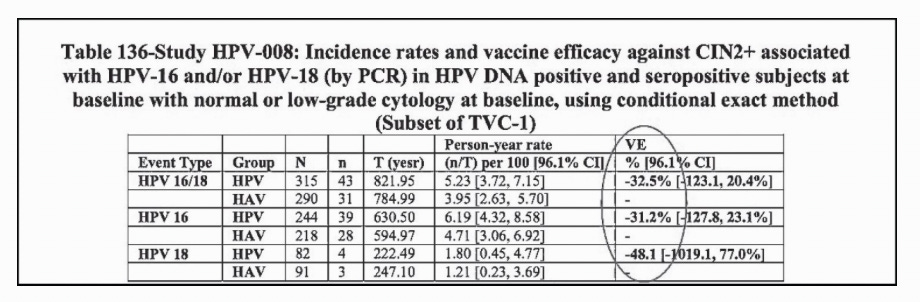
To further support this link between HPV vaccination and cervical cancer, the identical link was also found with the competing HPV vaccine, GlaxoSmithKline’s Cervarix (which was ultimately taken off the market for “low demand,” which I believe was a result of Merck doing a much better job marketing their vaccine):
Note: I also uploaded a full copy of this report in case the above link stops working.
If you take a step back, it’s extraordinary that Merck (and GSK) able to sell the world on the idea their vaccine “would prevent cancer” because it did something which might do something which might prevent cervical cancer. What’s even more extraordinary was that their data showed for many the exact opposite for many of the vaccine’s intended recipients. For example, to quote Minnesota’s Department of Health:
Human Papillomavirus (HPV) is a common sexually transmitted infection. More than 90 percent of sexually active men and 80 percent of sexually active women will be infected with HPV in their lifetime.
Around 50 percent of HPV infections involve certain high-risk types of HPV, which can cause cancer. Most of the time, the body clears these infections and they do not lead to cancer. However, persistent infections can cause changes that lead to cancer.
Note: I have multiple patients who had an existing HPV infection get much worse after HPV vaccination or developed HPV shortly after vaccination despite never having had sexual contact prior to the vaccine. Because of these observations, I am inclined to believe this data has real world consequences.
An Inconvenient Datapoint
Given that the HPV vaccine clearly increased rather than reduced the risk of cervical cancer for those already infected, this suggested the most appropriate thing to do would have been to have potential recipients first be tested for HPV prior to receiving the HPV vaccine. However, since that was at odds with the goal of having a blockbuster that was given every women in the world (along with many men), that didn’t cut it since:
•You couldn’t do mass HPV vaccination clinics if you have to wait for test results (as hard as this is to believe, there are numerous cases where groups of children at school were pressured to vaccinate so they wouldn’t die of cervical cancer, after which, many were injured due to the high rate of adverse events following the HPV vaccine).
•You would miss the sales opportunity to pressure a patient on a medical visit to vaccinate if you had to wait for a negative test to come back.
•Since many people had already had HPV, you would lose all of those potential customers.
•The general public learning the vaccine should not be given to those who had already a HPV infection would cast doubt on the 100% “safe and effective and necessary” mantra being used to sell the vaccine.
Note: it goes without saying that all of the above also applies to the COVID-19 vaccines, to the point that even when data emerged showed natural immunity provided better protection than the vaccine and people sued for natural immunity to exempt them from vaccine mandates, the mandates were still enforced.
See if you can guess what was done to get around this sales problem. To quote the HPV Vaccine on Trial:
Merck and GSK state that the vaccine may not protect women who have been exposed to HPV before. What they do not say, however, is that women who have been exposed to HPV before may have enhanced risk for cervical disease.
The clinical trial results show this risk, which should have prompted Merck and GSK to strongly consider screening before vaccination, or prescreening. Instead, by recommending the vaccine for children who are “sexually naive, this appeared to avoid the problem of so-called “negative efficacy.”
Note: since vaccines are typically dosed the same regardless of age, smaller and younger individuals often have the worse reactions to them (e.g., premature infants are more likely to die suddenly following vaccination)
The FDA asserts that these women had “enhanced risk factors” for CIN 2 or worse, including smoking or a history of sexually transmitted infections. These enhanced risk “factors reflect real-world cervical cancer risk, though. The FDA minimized these risk factors, suggesting that the data merely showed that the vaccine “lacks therapeutic efficacy among women who have had prior exposure to HPV and have not cleared a previous infection.” In its 2006 clinical review of Gardasil, however, the FDA “concluded that there was no clear evidence of vaccine related disease enhancement.” The FDA did not deny, however, that there was some evidence of risk enhancement.
The chart above shows enhanced risk for those who received Cervarix compared to controls, ranging from negative 31.2 percent for women positive for HPV 16 alone to negative 48.1 percent for those positive for HPV 18 alone. The FDA did not consider these results statistically significant or flag them for further scrutiny. Notably, in the Cervarix trial of women aged 26 and over (“VIVIANE”), the investigators reported as serious adverse events two cases of cervical cancer among women who received the vaccine.8
Note: these are both excellent illustrations of how the FDA will try to twist data that clearly shows “their” product is bad—something we have sadly seen throughout the COVID-19 vaccine campaign.
To this day, the FDA and CDC do not recommend prescreening before vaccination. The American College of Obstetricians and Gynecologists, a leading US professional association, goes even further. It recommends that physicians not prescreen patients. In a 2017 opinion, it stated:
“Testing for HPV DNA is not recommended before vaccination. Vaccination is recommended even if the patient is tested for HPV DNA and the results are positive. Even if a patient previously has had an abnormal Pap test or history of genital warts, vaccination is still recommended.”
Note: The 2017 guidelines can be found here, while the current ACOG ones can be found here.
Sadly, however:
Parents cannot even opt to check for HPV antibodies before vaccinating because no commercial HPV antibody blood test is available.
Let’s now look at what happened with the another dangerous vaccine that’s notorious for frequently causing autoimmune disorders.
COVID-19 Vaccine Negative Efficacy
As I discussed in the last article, one of the less appreciated side effects of the COVID-19 vaccines is that they appear to worsen a pre-existing COVID-19 infection.
Note: I believe the failure to recognize this initially arose from the COVID-19 vaccine trials having protocols which excluded subjects with an active COVID-19 infection from participating in the trial.
Since there a lot of well known reason why you should not vaccinate while fighting off an infection, it was quite telling to see how this sales obstacle was handled—especially given that unlike HPV, the mass deployment of COVID-19 tests made it very easy to know if someone had COVID-19 . For example:
The CDC initially recommended waiting 90 days after an infection to get vaccinated. But guidelines have since changed to reduce the chances that someone might skip the vaccine or booster altogether after waiting, she said. According to the updated guidelines "People with COVID-19 who have symptoms should wait to be vaccinated until they have recovered from their illness and have met the criteria for discontinuing isolation."
Note: typically the justification given for this was waiting until the infection cleared made the vaccine more effective. I looked through a lot of articles on the subject and could not find a single one which mentioned anything harmful might happen if you vaccinated while infected. I can’t prove this, but I suspect one of the key lessons the industry learned from the HPV vaccine was that it was critical to exclude anyone with an existing infection from future vaccine trials as otherwise, inconvenient evidence would be created that could harm future vaccine sales.
One of the first things that clued me into the fact it might be bad to vaccinate while infected with COVID was the observation that severe COVID-19 typically did one or more of the following:
•Was marked by a hyper activation of the immune system I rarely saw with other infections.
Note: to varying extents this also happened with more minor COVID-19 infections. For instance, when I had COVID, due to some unfortunate circumstances beyond my control, I was completely alone and had no access to any of the therapeutics I typically used to treat it, which necessitated doing a barebones approach to treating the illness I’d pieced together from working with a variety of life-threatening COVID infections. At the time I had the infection, based on how unstable my physiology was, I was quite worried things would go south, and I feel had I not handled things the way I did, it’s possible I would have died. I recovered completely (if anything I felt better a week after the infection than I had prior to getting sick) but I have in my life never experienced anything similar to what happened during that illness.
•Cause a cytokine storm (which could be fatal in hospitalized patients).
•Create a fibrotic response throughout the body (which lead to permanent debilitating complications like pulmonary fibrosis).
Additionally, one of the most interesting theories I heard to explain the pathology of COVID-19 was that much of the disease was an allergic reaction to the spike protein, which in turn was why it always took a few days after the initial infection for the individual to become really ill. I found this doctor’s model quite noteworthy since it was both prognostic for the course of COVID-19 (as he identified people would “recover” but then always get severe ill on the eighth day of the illness) and often fairly helpful as once he simply treated the allergic reaction, people got well.
In turn, prior to the vaccine hitting the market, I heard a lot of commercials say that if you had a horrible reaction to the vaccine, that was fine and “it meant it was working” (something I’d never heard for any other vaccine). Then, once the vaccine hit the market, I heard many people say they felt so ill they thought they were going to die—something I had learned to associate with the COVID-19 infections that could become life threatening.
This understandably made me worried the highly inflammatory nature of the vaccine had a good chance of tipping someone over into the dangerous form of COVID-19.
The first clue I got that this was going to turn into a big issue was the relentless marketing push used to sell the vaccine to individuals with long COVID (who understandably thought their condition meant they’d already had a chance to develop immunity to COVID-19 and hence didn’t need to vaccinate). This push in turn was rationalized under the logic that “since their long COVID was the result of an insufficient immune response being unable to clear the infection from their system, and that the vaccine stimulate the immune system enough to do that.”
As you might guess, while I never saw someone get better (except for someone who got better in some ways but worse in others), I saw multiple people with long COVID get much worse after vaccinating.
Note: like many, I believe many people who have “long COVID” actually have vaccine injuries they are in denial about (e.g., due to their political ideologies).
Simultaneously, I began receiving multiple concerning reports of someone who had appeared well, gotten the COVID-19 vaccine, and then immediately and rapidly came down with a severe COVID-19 infection which before long was fatal (some of which I logged). This suggested something similar to what had been seen with the HPV vaccines was occurring—a controlled existing infection spiraled out of control due to the extra inflammation which was induced by the vaccine.
Since that time I’ve also learned that:
•Analyses of VAERS report (e.g., this one) found after 1-2 weeks, the most common causes of death reported following COVID vaccination was a COVID-19 infection.
•I have seen a few reports (e.g., in a survey Steve Kirsch asked me to review) of someone who had a mild (PCR confirmed) lingering COVID infection then get a COVID vaccine and immediately crash (e.g., they needed to be hospitalized).
•I’ve come across numerous cases of individuals who had not gotten ill throughout the pandemic be around a recently vaccinated (or boosted) person who clearly got them ill with COVID-19. These reports suggest something about the vaccine impaired the vaccinated individuals immune response to an existing COVID-19 response, which in turn caused their viral load to rise, and hence likely resulted in a significant increase of how much of the virus was spread into their environment.
In short, I do not think it is necessarily a good idea to vaccinate while ill with an infection, nor am I sure there’s even a point in doing so in the first place (as you should already have immunity if you’ve already had the infection), but since not vaccinating, regardless of the reason, is bad for business—we vaccinate.
Conclusion
At this point, almost every has noticed COVID-19 got worse, not better once the vaccines were introduced, which understandably makes many question how the severe side effects of these vaccines can possibly be justified. Sadly, we saw something very similar with the HPV vaccine, and unfortunately, because there was not enough public resistance against it, Merck’s playbook was revised and updated for COVID-19.
Let’s take a brief look back and see exactly what resulted from over a decade of Gardasil:

When you look at these charts, it’s helpful to keep a few things in mind:
•The HPV vaccine trial showed it caused between excessive 41-100 deaths per 100,000 recipients, whereas at best, its saved 2 lives per 100,000 recipients (and most likely far less).
•In addition to this being much higher than the cervical cancer death rate, the average age of death from cervical cancer is 59, so the children and young adults in the trial lost a much greater portion of their lives than those who might have a preventable cervical cancer.
•Like the COVID-19 vaccines, the majority of side effects from the HPV vaccine were not fatal, and hence are frequently not recognized (e.g., the national disability rate went up by 10% after the COVID vaccines were deployed).
•As stated above, much of the benefit attributed to vaccination was actually due to an existing decline in infectious illness which the medical profession stole the credit for. Similarly, as these graphs show, it’s pretty clear that most of the decline of cervical cancer came from the pap smears which predated the HPV vaccine.

In both of these graphs, a case can be made that introducing the HPV vaccine not only did nothing, but rather it made cervical cancer worse. With the HPV vaccine, opinions are split between this resulting from the vaccine itself making HPV worse or its introduction causing the management of cervical cancer to be changed (since everyone became convinced that HPV vaccination was the most important thing for preventing cervical cancer).
A major reason why I started The Forgotten Side of Medicine was in the hope it could help our society stop repeating the mistakes that keep on being made. In turn, I’ve tried to show how each disaster we witnessed occurred throughout the pandemic did not come out of nowhere, but rather was an escalation of a longstanding but concealed issue. It is my hope that by exposing what happened in the not so distant past with the HPV vaccine it can help move our culture towards developing a “herd immunity” against these predatory marketing practices and the inevitable harm that follows once an unsafe and ineffective vaccine is pushed on the public.
A complete index of the articles published on the Forgotten Side of Medicine can be found here.
Postscript:
I forgot three major points when writing this.
#1 A huge issue with the COVID vaccines was it being known that prior to COVID-19, each attempt to make a SARS vaccine backfired and instead caused the vaccinated animals to become severely ill with SARS (when compared to unvaccinated animals). This phenomena was referred to as “antibody dependent enhancement” (Peter Hotez even warned Congress about it before he became the national COVID vaccine spokesman). It is quite likely similar is happening with the COVID vaccines.
#2 Antibody dependent enhancement has also been observed with the influenza vaccine.
#3 I and many others (e.g., the commenters here) have noticed that flu shots often make people become ill with the flu (which raises the possibility they had a stable flu infection in the background prior to vaccination) and likewise, anecdotally, I’ve noticed everyone I’ve worked with who was hospitalized for the flu had also received a flu shot that year.
I remember Geert VandenBossche saying something like, when you jab people in the middle of an epidemic, the virus will mutate quicker. that one would inject a pregnant woman is beyond belief. I saw the vaxxed films and remember a young woman who had the papilloma shots, got very sick from it, was vaccine damaged, and a few years later, got cervical cancer. I know several who got the covid shots and were sick from the shots and then had the virus.
I forgot three major points when writing this.
#1 A huge issue with the COVID vaccines was it being known that prior to COVID-19, each attempt to make a SARS vaccine backfired and instead caused the vaccinated animals to become severely ill with SARS (when compared to unvaccinated animals). This phenomena was referred to as “antibody dependent enhancement” (Peter Hotez even warned Congress about it before he became the national COVID vaccine spokesman). It is quite likely similar is happening with the COVID vaccines.
#2 Antibody dependent enhancement has also been observed with the one influenza vaccine.
#3 I and many others (e.g., the commenters here) have noticed that flu shots often make people become ill with the flu (which raises the possibility they had a stable flu infection in the background prior to vaccination) and likewise, anecdotally, I’ve noticed everyone I’ve worked with who was hospitalized for the flu had also received a flu shot that year.
Additionally, I miswrote original antigenic sin (it's "antigenic" not "antigen").