The Hidden Link Between Hypermobility and Vaccine Injuries
How ligamentous laxity predisposes sensitive patients to vaccine induced microstrokes

Story at a Glance:
•Ligamentous laxity is found to be commonly associated with a variety of complex illnesses, and is frequently seen in patients who have an increased sensitivity to their environment.
•A variety of unrecognized (and often treatable) factors in the modern environment have caused ligamentous laxity to become much more common in recent years.
•A novel hypothesis that explains many of the unusual complications of the COVID-19 vaccines is that they trigger a collapse of the iliac veins in susceptible persons (e.g., those with ligamentous laxity and a corresponding weakness of the tissue lining the vessels). This, in turn, causes a variety of complications including micro-clots and mast cell activation syndrome.
•Many of the agents which significantly injure patients (e.g., vaccines) partially do so by causing the fluids in the body to clump together. This directly impairs the circulation within the body and indirectly impairs it by removing the repulsive force which prevents weakened vessels from compressing.
•In this article, I will discuss how manganese plays a critical role in ligamentous strength and our preferred protocols for repairing ligamentous laxity.
Note: over the last month, individuals who’ve been injured by the COVID vaccine reached out to me to share the earlier version of this article was very insightful for them. As such, I felt it was important to revise it so more could learn about this concept (likewise why I recently published another article discussing what creates fluid motion in the body).
Frequently, a treatment which works very well for one patient will fail to help (or harm) a patient with a very similar issue. In turn, a critical aspect of medicine is being able to recognize the unique differences between patients so you can best determine what treatment fits best for each patient and what dose is the most appropriate for each patient. Unfortunately, in “standardized medicine” (where everyone follows treatment algorithms) there is no single approach which helps all patients, and as such, protocols and dose are decided upon which will overall fit the most number of people, but simultaneously fail many others (which is a major reason individuals quit conventional care and seek out alternatives).
Note: the art of selecting the correct dose (and the perils of our current approach to it) are discussed here.
Constitutional Archetypes
Fortunately, while this task seems impossible (as the basics of medicine are complicated enough), there are a variety of tricks that make the process much easier. One is a recognition of “constitutional archetypes” where individuals share a cluster of similar traits. This concept (discussed further here) is very useful, as once you become familiar with an archetype and you spot indicators of it in someone, it then becomes possible to identify to predict many other characteristics of that individual.
In medicine, I find one of the most helpful archetypal frameworks to be the three Gunas (from Hinduism), which posits that three primordial energies exist that individuals can be composed from:
Sattva, which has qualities including “goodness, calmness, harmonious.”
Rajas, which has qualities including “passion, activity, and movement.”
Tamas, which has many qualities including “ignorance, inertia, laziness.”
Note: Sattva in many ways mirrors Vatta, and to a lesser extent the ectomorph type. Rajas in turn pairs with Pitta and mesomorphs while Tamas pairs with Kapha and endomorphs.
From a medical standpoint, Tamasic patients tend to have a general thickness, heaviness and solidity to them, while Sattvic patients tend to have a more light and ephemeral quality to them. Each in turn has a very different response to medical therapies. Tamasics typically tolerate and often only respond to forceful interventions (e.g., many of the standard medical therapies) whereas Sattvic’s respond very poorly to aggressive therapies and instead need gentle ones to coax their health back (which are often energetic in nature like acupuncture)—something which often does virtually nothing for Tamasic patients.
Put differently, Sattvics are often recognized as being much more sensitive to environmental toxins and harmful medications (e.g., many of them refer to themselves as canaries in reference to the birds miners used to monitor for toxic gases in coal miners as they would be affected much sooner than the miners and that we should be taking their medical injuries as a warning sign many of the substances we are being exposed to are not safe). Likewise, Sattvics frequently need much lower doses of medications, but unfortunately often instead are overdosed because standardized medicine only uses the dose that best fits the entire population (which as I discuss here, is inevitably the wrong dose for many).
Note: COVID vaccine injuries disproportionately affected the Sattvic archetype.
Throughout my life, I’ve known more Sattvics than I can count, and one of the things I’ve always found immensely unfair is that most people cannot relate to the struggles they face (e.g., many, including some of their doctors, think they are “crazy” or “hypochondriacs”) or how sensitive they are to many things around them most never even notice.
As such, I’ve made one of the missions of this Substack to bring attention to their situation. At the same time however, I’ve always wondered “why is this constitution so sensitive?
Ligamentous Laxity
At this point, I often immediately recognize the sensitive patients by their presence, their psychological demeanor and their body shape. For instance, one of the frequent physical traits I associate with this archetype is a distinct pattern of movement (which is often graceful) that I believe results from laxity in their ligaments.
Since the ligaments stabilize the joints of the body by constraining their maximum range of motion, once the ligaments weaken, their laxity (looseness) frequently causes the maximum range of motion of the joint to increase.

Individuals with ligamentous laxity have certain advantages. For example, they are normally much more flexible (e.g., they can stretch their body much further), and often become dancers because of the mobility afforded to their body.
Conversely, ligamentous laxity also creates a variety of issues for those patients. The most common one is that since their body uses the ligaments to stabilize itself when a force enters it, once the ligaments weaken, things will frequently shift inside the individual more than they should in response to those forces.
For example, individuals with ligamentous laxity tend to be more susceptible to developing chronic injuries from car accidents or other physical traumas. Likewise, their joints “pop” easily, but if they get forceful adjustments to reset the position of their bones, the bones will often go back out of place (since the stability which would otherwise maintain that structure is lacking).
Note: I have seen numerous patients with ligamentous laxity that had far too many forceful adjustments that eventually created issues for them. This normally occurs either because the repeated adjustments (performed due to the patient’s pain rapidly returning after each adjustment) further weakened their ligaments or because the weakened joint exceeded its expected range of motion during a thrust and the bones of the joint ended up in a position which created other issues for the body.
Similarly, individuals with ligamentous laxity (especially when it is significant) tend to develop a variety of issues that are ultimately treated with surgery. Unfortunately, due to being more “sensitive” and having an impaired ability to heal following the surgery, they frequently suffer significant complications from those surgeries—which sadly leads to even more surgeries (e.g., there are many stories of this in the Ehlers-Danlos syndromes [EDS] support groups).
Note: since ligaments are composed of collagen, impaired collagen production often gives rise to ligamentous laxity. Likewise, since collagen production is needed to heal from surgeries, individuals with impaired collagen production have greater difficulty recovering from surgery.
Ligamentous laxity can also create a variety of other issues throughout the body (e.g., all sorts of gastorintestinal problems). One of the least appreciated consequences of hypermobility is that the body depends upon ligamentous tension for proprioceptive feedback (knowing where the body is in space), and as a result, once the ligaments become lax, hypermobile patients lose some of the general awareness that allows us to subconsciously navigate through the world.
For example, EDS is known to be associated with impaired balance and an increased likelihood of falling. However, it’s much less appreciated that this lack of proprioceptive feedback can give rise to a general sense of anxiety because the ground does not feel as stable below one’s feet—something which is difficult to appreciate unless one has experienced it directly (e.g., I’ve met people who easily survived a major earthquake but were psychologically disturbed for years after as a result of them briefly losing their sense of the ground which they had always previously taken for granted).
What Causes Ligamentous Laxity?
A variety of processes can cause ligamentous laxity. Frequently, a combination of these are at work (e.g., someone with a pre-existing weakness in a ligament is more likely to have something injurious to a ligament create a chronically lax ligament).
Physical Injuries
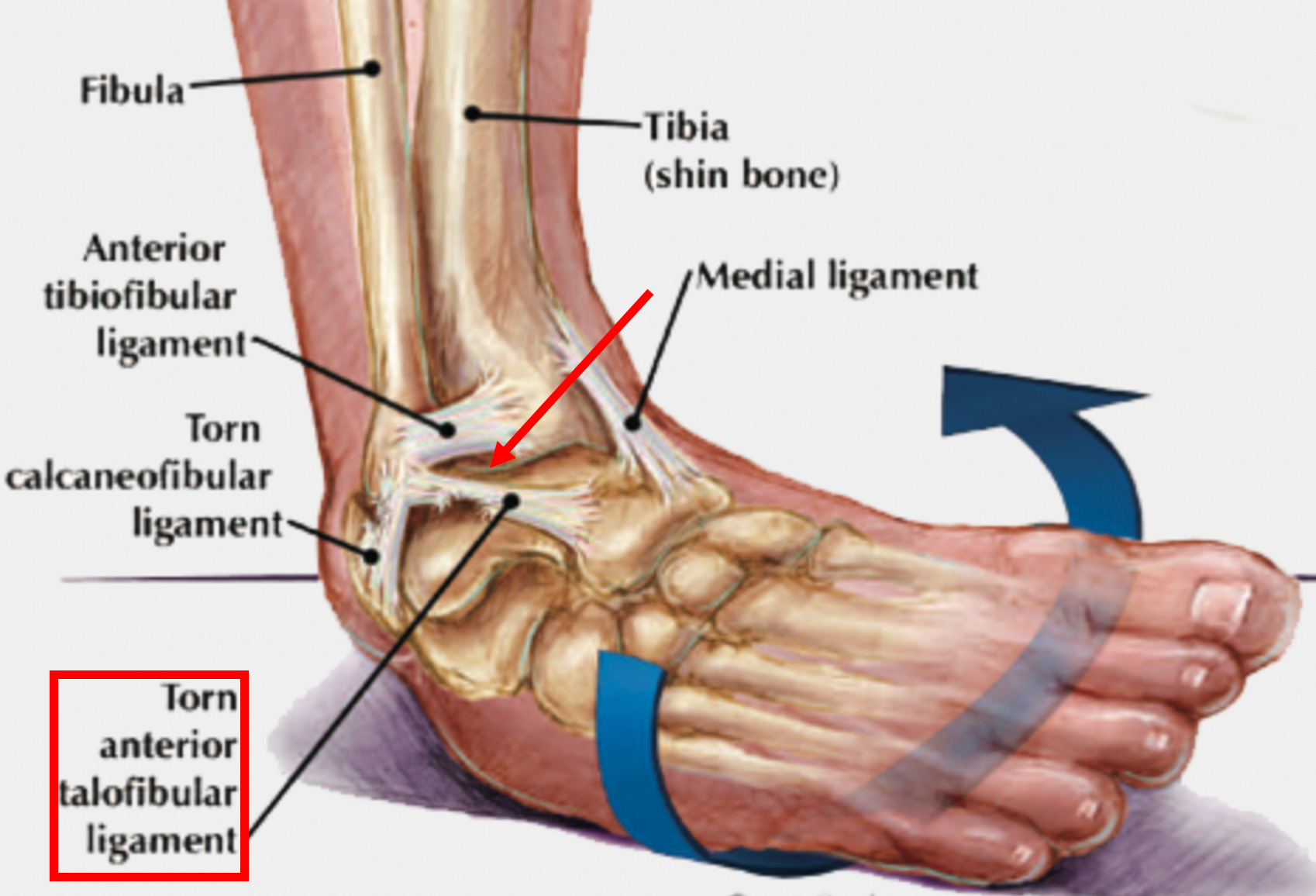
Ligamentous weakness is frequently caused by a chronic injury to a ligament (or an injury which did not properly heal). For example, when the ankle is injured from a sprain, the ligament that keeps the ankle from turning inwards gets damaged, predisposing us to an unstable ankle and future ankle injuries until the ligament is repaired and strengthened.
Pharmaceutical Injuries
In addition to physical injuries, biochemical injuries can also occur. This is best known to occur following the use of anti-inflammatory medications. For example, NSAIDS like Ibuprofen (which are typically the go to for “treating” sports injuries) in addition to reducing the discomfort of an ankle injury also weaken the ligaments (as by suppressing the inflammatory process it also suppresses the healing process).
This results in sprains that are treated with NSAIDs often being predisposed to future injuries (since the stability given to the joint by those ligaments is partially lost until something like a regenerative therapy is given to repair that ligament)—which in the case of ankle sprains is something I and colleagues frequently see in our patients.
One of the most common therapies given to treat joint pain are injected steroids, which, by being powerful anti-inflammatories, are often initially effective in making the patient feel better. Unfortunately, injected steroids are also weaken ligaments at the site where they are injected, particularly when they are given multiple times. Since joint inflammation (and pain) often is a result of improper joint stabilization by a ligament (leading to the joint being worn down by inappropriate pressures), this treatment approach results in patients needing more and more injections as their ligaments further weaken.
Note: this is also a common issue for those with chronic neck or back pain and unfortunately often results in them often “needing” to get a surgery to stabilize the spine—which often makes things even worse (that subject and alternative approaches to treating spinal pain are discussed here and here). One of the particularly frustrating things about this situation is that DMSO can be used for many of the same injuries and chronic pains the ligamentous destroying drugs are used for, but rather than further weaken them, DMSO often repairs the ligaments (along with often being far more effective at resolving the patient’s condition).
Additionally certain more toxic pharmaceuticals can also weaken the ligaments. For instance, beyond steroids, I have also frequently observed this after the someone suffers an injury from a more toxic pharmaceutical (e.g., this is well known to occur from fluoroquinolone antibiotic like ciprofloxacin but I’ve also seen it after an accutane injury).
This I believe results from the fact that the body is continually rebuilding and remodeling its structural tissues to meet the needs of the environment. For example, the bones depend on the weight of gravity to signal growth, so when astronauts are in space for prolonged periods of time, their bones significantly weaken (and may break once they return to Earth’s gravity) unless the astronauts also do special exercises in space.
In addition to bones, the collagen of the body also continually rebuilds and remodels itself. Since collagen production is an energy intensive process, if the mitochondria get injured (which fluoroquinolone antibiotics are notorious for doing), over time the connective tissue in the body will also weaken until it fails as a result of it no longer being able to accommodate a previously manageable force input (e.g., sudden tendon ruptures are very common after fluoroquinolone usage).
Constitutional Predispositions.
EDS and Marfan Syndrome are the two classic medical conditions that are associated with ligamentous laxity. Both of these conditions are considered to be rare diseases, with EDS being estimated to affect between 1 in 5000 to 1 in 100,000 patients (depending on its severity and the source of the estimate), while Marfan Syndrome is estimated to affect 1 in 5000 patients.
Note: One recent paper found that the prevalence of diagnosed EDS was 1 in 500 and many believe it is even more common (e.g., I’ve met dozens of people who have appear to have EDS or an EDS-like syndrome).
In addition to EDS, there is also a self-explanatory condition known as “generalized joint hypermobility,” (GJH) which is found to affect around 12.5% of the population and predisposes them to musculoskeletal pain and injury. At this point I suspect that both this condition and EDS are under-diagnosed and that a spectrum exists between overt EDS and GJH.
Functional Predispositions
It some cases you can watch a ligamentous laxity rapidly onset within the body. The most classic example results from the hormone relaxin (released during pregnancy), which weakens the ligaments of the body so that the pelvis becomes able to stretch and accommodate the birthing process. Because of this increased hypermobility, pregnant women become more predisposed to physical injuries (and developing musculoskeletal pain from the weight their baby).
Note: other hormones the female body secretes counteract the effects of relaxin, especially once the pregnancy is complete, and in turn, those with pre-existing hormonal imbalances are significantly more susceptible to musculoskeletal issues both during and after a pregnancy. Likewise, having pre-existing hormonal imbalances (due to the ligamentous weakness they create) can make women much more susceptible to musculoskeletal issues, particularly after menopause.
In my eyes the most important functional predisposition of ligamentous integrity is nutritional status. While a variety of things can affect ligamentous integrity, we’ve found the often forgotten metal manganese (Mn) plays one of the most important roles. In turn, it is extremely common to find people who:
•Live in areas with lower manganese levels in the soil also appear to have higher rates of ligamentous laxity.
•Have ligamentous laxity that gradually improves when they appropriately take manganese for a prolonged period.
•Have a predisposition to ligamentous laxity (e.g., EDS or a hypermobility syndrome) be tipped over the edge by a manganese deficiency, and likewise have patients with existing hypermobility significantly improve from manganese supplementation.
Since manganese deficiency is such a common issue now, we’ve put a lot of thought into why we see it so frequently. Presently, we have four leading explanations:
•First, the topsoil has been heavily depleted of essential minerals by our modern farming practices. This creates a variety of issues (and likewise significant improvements are seen in the plants grown in remineralized soil and in the humans who consume those plants).
•Glyphosate (Roundup), a toxic but widely used herbicide, has a high affinity for chelating (trapping) certain minerals, once of which is manganese. Because of this, I believe the continually increasing levels of glyphosate in the environment have contributed to the current widespread deficiency of manganese.
•Bacteria require iron for their metabolism (and in turn one of the defensive mechanisms the body has to stop an infection is to sequester iron so bacteria cannot reproduce). The bacteria which causes Lyme disease has an unusual adaptation, which to my knowledge is unique in nature (which raises interesting questions about where Lyme came from). It uses manganese instead of iron, which thereby protects it from that defense mechanism, and we have long suspected it also causes individuals infected with the bacteria (including those with “silent” infections) to become manganese deficient.
•Mineral absorption is intrinsically linked to the acidity of the stomach (as acid is needed to chelate minerals that are tightly bound to plants), so deficient stomach acid (especially in the setting of nutritionally depleted soil) may predispose one to a manganese deficiency and hypermobility.
Note: in many cases, hypermobile patients have a variety of emotional sensitivities and varying degrees of psychiatric instability. Some of these patients have remarkable responses to targeted trace mineral supplementation (particularly for anxiety or feeling “ungrounded”). This observation in turn has led me to suspect an inability to obtain sufficient minerals from the diet (e.g., manganese) plays a key role in hypermobility.
Lastly, the relationship between manganese levels and hypermobility can also be seen in animals. For example, a study (inspired by the observation manganese deficiency correlated with weak antlers that were more likely to break) supplemented half of the deer with manganese and showed those deer had thicker and stronger antlers compared to the ones which did not receive manganese.
Note: manganese is often considered to be a toxic element (as it is associated with the neurological issues that follow chronic exposure to welding gas). I always thought this was strange as manganese is a necessary cofactor for numerous critical enzymes in the body (e.g., some of those within the mitochondria). Presently, I believe this is because the toxic form of manganese (e.g., that found in welding gas) is Mn³⁺, whereas the form that helps people found in the dietary supplements (and that typically tests well for patients) is Mn²⁺. In turn, I suspect that for some reason, Mn³⁺ impairs the function of essential enzymes that depend upon Mn²⁺. Alternatively, a hypothesis has been put forward (with data to support it) that manganese, while essential, also becomes toxic at high doses.
Ligamentous Laxity and Vaccine Injuries
There has been a longstanding observation in the integrative field that ligamentous laxity correlates with a predisposition to vaccine injuries. Likewise, a lot of readers have shared this observation with me after I broached this subject. For example, this comment was left by one reader:
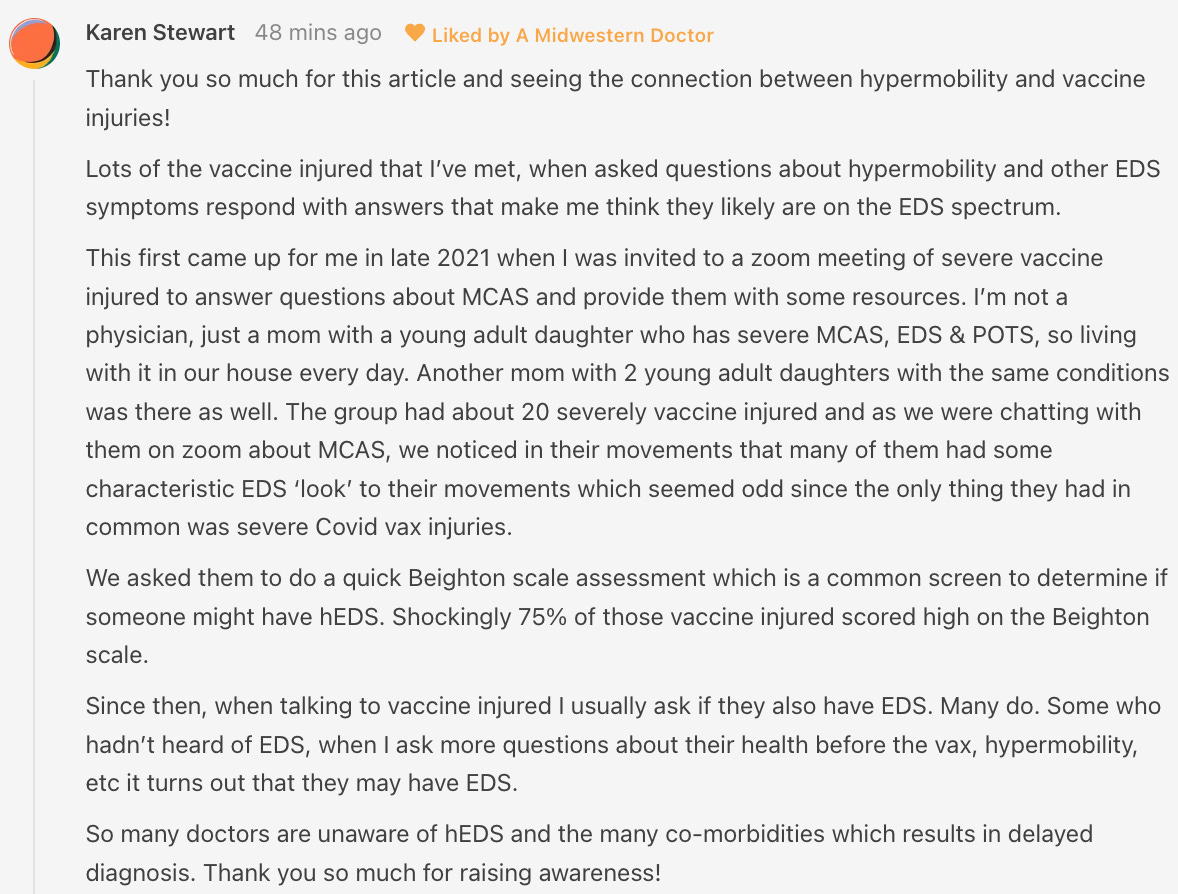
Prior to COVID, the HPV vaccine Gardasil was considered by many to be the most dangerous vaccine released upon the general population (a strong case could also be made that it was either the original DPT vaccine or the original smallpox vaccine, however by the time Gardasil emerged, those atrocious vaccines had mostly faded into memory).
Gardasil caused a variety of debilitating conditions (e.g., constant fatigue, cognitive impairment, a variety of autoimmune conditions and widespread neurologic dysregulation—things also frequently seen after the COVID-19 vaccination). At some point, holistic physicians began noticing patients (particularly women) with existing ligamentous laxity were much more likely to develop Gardasil injuries (and in turn a few researchers proposed genetic variations to account for this).
At the time, I assumed this correlation was due to:
•Individuals with ligamentous laxity also being more likely to be the more sensitive patients.
•Ligamentous laxity having a longstanding association with mast cell disorders, a condition which makes one hypersensitive to a variety of substances (e.g., drugs or vaccines).
Note: mast cell disorders are frequently observed to emerge in patients who develop COVID-19 vaccine injuries.
However, last year I learned of a novel hypothesis put forward by one of the leading doctors treating COVID-19 vaccine injuries which tied a lot of things together.
Iliac Vein Compression
The edited (condensed) twelve minute version of his presentation can be viewed here:
Dr. Jordan Vaughan’s key points (and my comments on them) are as follows:
•Many of the debilitating complications of the COVID-19 vaccine appear to result from the iliac vein (which governs venous return from the legs and pelvis) becoming compressed and its blood supply becoming significantly obstructed (which in turn gives rise to numerous characteristic symptoms that can be recognized once one knows to look for them). More importantly, this compression can often onset quite suddenly and patients remember the exact moment that compression occurred.
•The blood flow obstruction created by an iliac vein compression appears to cause a variety of conditions which could be analogized to “putrid blood,” such as blood clots throughout the body and mast cell activation syndrome.
Note: over a century ago, quite a few of the early pioneers in the medical field also noted that compression of the iliac region predisposed patients to a variety of illnesses they commonly attributed to the blood or lymph in the pelvis “fermenting.”
•A condition known as May-Thurner syndrome affects slightly over 20% of the population. In it, the (high pressure) right common iliac artery overlies and compresses the (low pressure) left common iliac vein against the lumbar spine
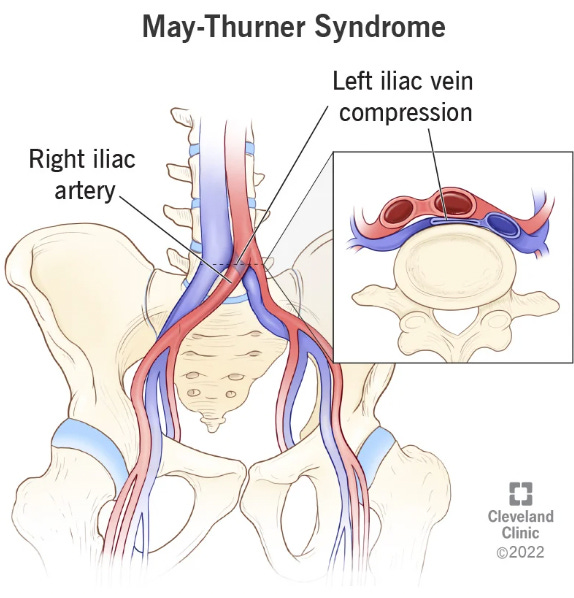
Normally, individuals with this syndrome do not notice it, but it some cases it can predispose them to unexpected blood clots (due to venous return being obstructed).
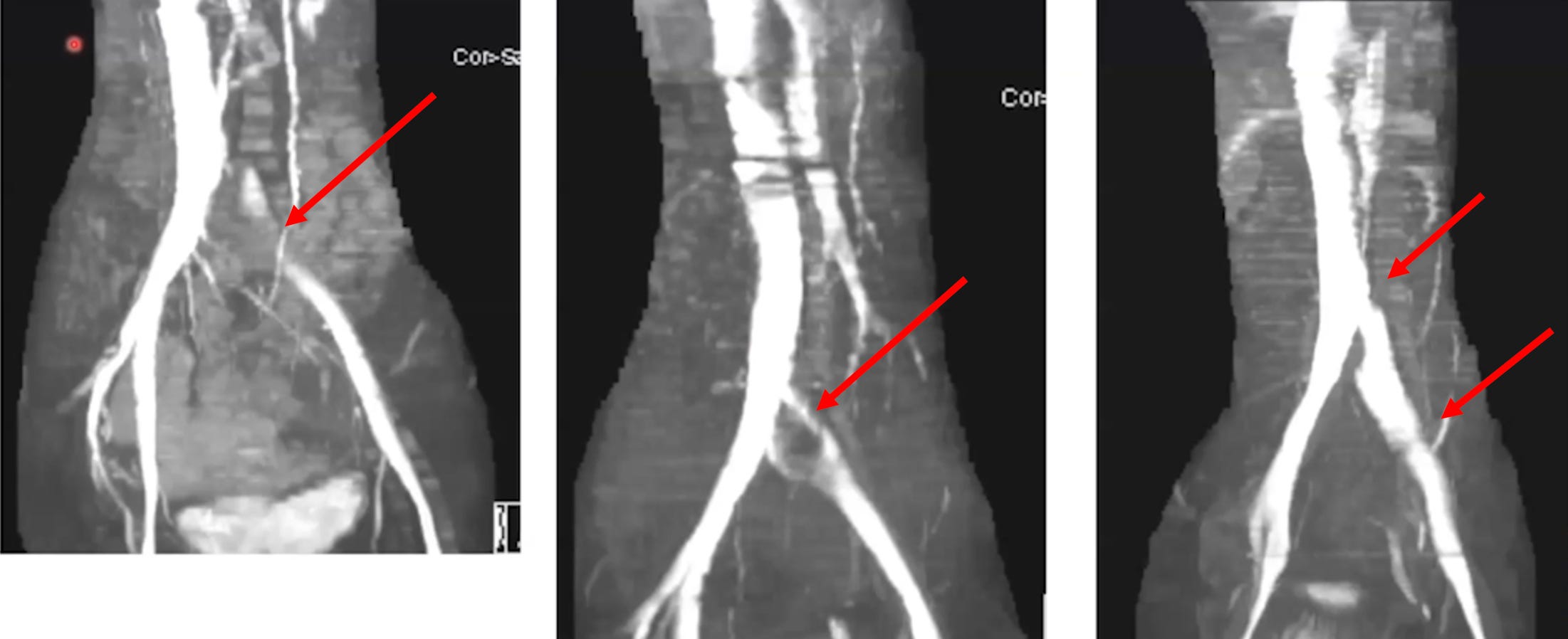
•Dr. Vaughan believes that the (well-documented) damage the spike protein causes to walls of the blood vessels weakens the iliac vein enough that pressure from the iliac artery can cause it to collapse. In turn, he has collected compelling radiography to prove it.
•If an iliac vein compression is treated with anticoagulation, this typically improves the symptoms of it, but once the anticoagulants are stopped, the symptoms return (as the source of the clotting has not been addressed). For this reason, iliac vein compressions are often treated with stenting, which Dr. Vaughan reports frequently significantly benefits patients.
Once I heard Dr. Vaughan’s lecture, I realized his hypothesis tied together many observations I’d made over the years and likewise explained many of the successes I had come across in vaccine injured patients after manual therapists after working on a patients hip socket either intentionally or unintentionally had partially (or fully) decompressed the iliac vein and created a dramatic “inexplicable” improvement in the patient’s condition.
The Hidden Life of Water
In many ways, the primary purpose of a scientific model is to create the worldview that nature is fully understood and has been “mastered,” when in reality, it often has a degree of complexity which greatly exceeds what any model can accurately encapsulate. In turn, as you begin to really look into phenomena, you’ll gradually notice inconstancies that upend the entire model.
As such, I’ve tried to draw attention to the fact water has a variety of unique properties that help explain many of life’s mysteries.
Liquid Crystalline Water
For example, I’ve written about the discovery that water ( H2O), when exposed to ambient energy source (particularly infrared) and a polar surface, will displace some of its hydrogen atoms and begin forming a hexagonal lattice of H3O2 molecules, and enter a fourth phase of matter between being a liquid and solid where it behaves like a liquid crystal.
This property is immensely consequential in biology, as much of the water within living organisms (due to them having many polar surfaces it can form from) is in this phase. For example, in a recent article, I highlighted that the hydrogen ions being displaced creates an energy gradient which allows life to transform ambient energy sources in the environment into something that can be harvested to fuel life (e.g., by creating spontaneously flows within the body).
Another critical property of this 4th phase of water is that it expands, resists compression or penetration, and is virtually frictionless when two layers of it slide against each other (in a manner virtually similar to what is seen when a skater skis on ice). This serves many critical functions for the body. For example, in the blood vessels, by having a continuously regenerating lining of H3O2 coat the inside of them, it protects them from being worn down and damaged by all the blood flowing through (while simultaneously providing a lubricating surface that allows the blood to freely flow through the vessel). Likewise, many of the joints (e.g., the knees) are lined by polar surfaces that promote the formation of this water and contain viscous proteins that further promote the formation of this water, all of which then creates a frictionless weight bearing mechanism between the bones that does not get worn down by the forces continually exerted against it.
Note: here I discuss in much more detail how liquid crystalline water creates the structure and stability of the body.
Zeta Potential
Another concept I’ve emphasized throughout this publication is zeta potential, which quantifies the electrical charge difference between colloidal particles in the liquid they are suspended within (and applies to most fluids systems in nature). This is because like charges repel each other, so when a sufficient amount of matching charges are present (which in nature are almost negative due to liquid crystalline water creating a negatively charged layer on what it coats), the particles in the solution will resist outside pressures (e.g., gravity or attracting charges) to clump together and instead stay dispersed. Conversely, when insufficient zeta potential is present, they will clump together, with the clumps becoming larger and larger as the zeta potential declines.
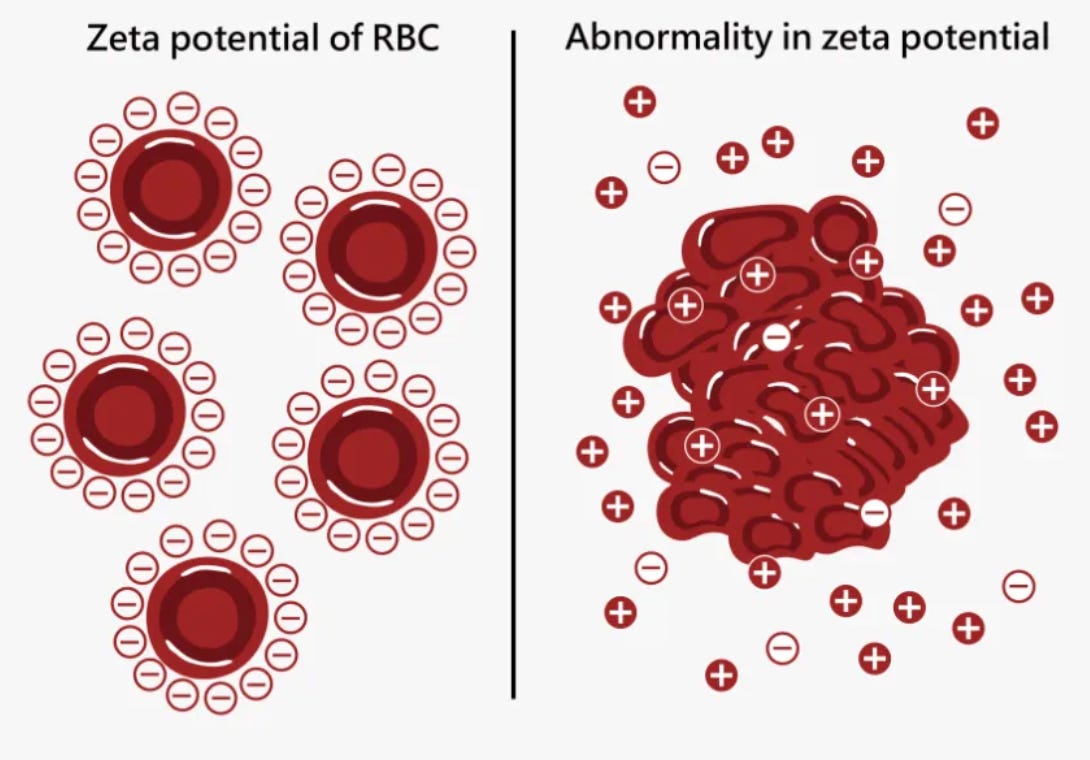
In the body, if this happens, red blood cells will clump together, eventually forming microclots which can cause either acute illness, or more commonly chronically debilitating illnesses. In turn, we believe this process underlies many chronic illnesses as agents that are well suited for restoring it often create dramatic improvements in health (which numerous readers here have reported) while conversely agents that are well suited for disrupting it (e.g., aluminum, the spike protein, and dangerous microbes such as malaria) can often cause a myriad of challenging illnesses.
Note: other fluids in the body (e.g., cerebrospinal fluid or lymph) will also clump together if their zeta potential is disrupted.
Interwoven Vessel Integrity
Because the body is so interconnected, it is often quite challenging to break it into separate pieces (which every model has to do). For example, there is a huge overlap between liquid crystalline water and zeta potential, so as one worsens, the other often does too and as one improves, the other often improves (discussed further here).
One of the key things to understand about both of these is that they allow the blood vessels to resist compression, as throughout the body liquid crystalline water creates the incompressible units that create the inherent expansion of the body and likewise, the mutually repelling charges in water (with a sufficient zeta potential) also prevent compression from occurring. Finally, the vessels themselves have an inherent tissue strength that allows them to resist compression, which in most cases can compensate for a partial impairment of the other two.
However, as these fail, it begins becoming possible for compressive forces to collapse the veins. Since hypermobility weakens the lining of the blood vessels, in practice, we find hypermobile patients have a reduced ability to tolerate impairments of the physiologic zeta potential or the liquid crystalline water within it (as the strength of the blood vessel linings can no longer adequately compensate for a loss of the expansive forces within the vessels), and as such, they often far more frequently pass a critical zeta potential threshold where issues immediately follow.
Similarly, both of these also directly influence the integrity of the lining of blood vessels. For example, in addition to liquid crystalline water (if present) providing the layer that protects the blood vessels, the blood supply for the larger vessels, the vasa vasorum is quite narrow and hence easily obstructed by zeta potential induced microclots (which disproportionately affect the smallest vessels), at which point the lining of the vessels was repeatedly observe to desquamate (fall off, allowing the deeper areas to get damaged). Likewise, many of the agents which impair the physiologic zeta potential (e.g., pathogenic bacteria or the COVID spike protein) also frequently damage the lining of the blood vessels.
Because of all of this, I hence believe the increased susceptibility to blood vessel compression and the myriad of symptoms blood flow obstructions can create helps to explain why hypermobile patients are so sensitive to certain toxins (e.g., many microbial ones) which adversely affect the physiologic zeta potential. Likewise, I believe many of the dramatic improvements certain patients see (e.g., those with COVID vaccine injuries) result from critical blood flow obstructions reopening.
To further illustrate the interconnectedness of these processes:
•In addition to stenting the iliac vein (to reopen it) other dramatic improvements have also been observed with venous stenting. For instance, for years patients with multiple sclerosis (a condition which has been found to be 10-11 times as common in EDS patients) have experienced significant benefit from stenting their jugular veins open (thereby improving the venous drainage of toxins from their head). Likewise, before this technique was restricted I heard many stories of individuals with other complex disorders (e.g., fibromyalgia and lyme disease) significantly improve following stenting of their jugular vein.
•Many of the challenging chronic neuroimmune illnesses that are associated with both poor circulation and mast cell activation syndrome (e.g., Lyme disease and mold toxicity) also have unique characteristics that directly impair zeta potential. In turn, we frequently find that attempts to treat these diseases don’t go well unless something is also done to mitigate their adverse effects on zeta potential (especially within the lymphatic system).
Zeta Potential Destroying Vaccines
To “work,” Gardasil (the HPV vaccine) used an adjuvant which dramatically impaired the physiologic zeta potential. In turn, once the vaccine hit the market, a wide range of injuries were reported from it, including many new autoimmune disorders, a variety of circulatory impairments and it triggering mast cell activation syndrome.
As it happens, those are also the exact same issues that were found from the COVID vaccines (another vaccine which is highly damaging to the physiologic zeta potential)—and as I hope this article has shown, there is a rational basis for that link.
Note: Besides the HPV vaccine and COVID vaccines I believe the vaccines which most effectively disrupted the physiologic zeta potential (and all created significant illness) were:
•The original smallpox vaccine.
•The anthrax vaccine
•The now banned DTwP (we use the DPaT now and ship DTwP to the third world).
As such, I now believe a key reason why I often see so much improvement in venous circulation after treatments are provided (e.g., for a COVID vaccine injury) to restore the zeta potential of the body is because doing so “re-expands” the compressible vessels of the body (including those within the lymphatic system).
In short, these concepts illustrate how interconnected the body is and how a weakness in one area can often predispose to a severe complication from something others would be relatively unaffected by. For example in addition to this concept we also noticed that COVID vaccine injuries would disproportionately affect areas of pre-existing injuries or inflammation (e.g., chronic arthritis or an old scar)—indicating that most of the body could tolerate the stress the COVID vaccine placed on the body, but the weaker areas could not—much in the same way the vessels can no longer tolerate a loss of the expansion within the fluids.
Note: a similar pattern of the disease first appearing in areas of pre-existing weakness is also seen in Lyme disease (another chronic inflammatory disease that adversely affects the physiologic zeta potential).
EMFs and Fluid Obstructions
These patients are also sometimes quite sensitive to EMFs, and over the years I’ve seen a variety of theories to explain why (e.g., EMFs trigger mast cell degranulation exacerbating the mast cell disorders commonly seen in these patients, EMFs mobilize heavy metals within these patients, EMFs provoke their existing infections into releasing reactive substances).
Given all of that, I’ve long wondered if EMFs affect zeta potential and the immediate responses people get from being around them (e.g., headaches) could be attributed to zeta potential shifts. In turn, some data support this:
•I have seen numerous videos of blood cells under microscopes appearing to clump together after being exposed to EMFs and I know of two studies which also showed this. The first found clumping occurred after being around a wired computer or a 2.4 GHz wireless phone with a much greater effect seen from the wireless phone, the second, in 10 subjects, found 45 minutes of cell phone exposure caused significant clumping to blood cells, and with an additional 45 minutes of exposure, also deformed their shape and the third determined polarized 1.8 GHz caused clumping (with older individuals—who typically have the lowest baseline zeta potential—being the most sensitive to these effects).
•The key problem with the previous data is that potential artifacts are introduced once blood is taken out of the body, so it may not generalize to what occurs within the body. However, one study, using ultrasound of the popliteal vein, was able to show that placing an Apple iPhone 16 (set to emit minimal data) next to the vein for 5 minutes caused significant clumping in the blood, and that after 5 minutes of walking (and no further exposure) some aggregations still existed—with these results being replicated 3 times over a 4 month period.
Note: blood sludging from impaired zeta potential, when severe, can be seen in larger veins (e.g., this has been repeatedly shown with ultrasound, and Pierre Kory, a world expert in point of care ultrasound shared that he would occasionally see echogenic blood within the largest vein in the abdomen—at which point the ICU patients soon died regardless of how stable they appeared clinically).
Presently, I know of three explanations which could account for this:
•First, zeta potential, is in part due to the layer of negatively charged liquid crystalline water which forms around cells. Pollack has reported Wifi routers shrink the amount of liquid crystalline water present by 10-15%, and similarly, this study shows that EMFs affect liquid crystalline water). Likewise, as circulation depends upon the liquid crystalline “pump” if EMFs disrupt liquid crystalline water’s formation, this could also account for rapid symptomatic losses of blood flow.
•EMFs may produce positive ions. These decrease zeta potential (which is also why negative ion therapy provides a myriad of benefits and certain environments or weather patterns create significant illness).
•Third, one study determined the polarized nature of unnatural EMFs caused oscillations within the molecules of cells that altered cell membrane potential (and hence zeta potential).
In short, given how sensitive some people are to EMFs, I believe this facet of their condition should be given consideration (particularly since to some extent it can be antidoted by restoring their physiologic zeta potential).
Repairing Ligamentous Laxity
In a previous article, I share my perspectives on neck and back pain, emphasizing essentially that the root cause of those issues are rarely addressed and instead people are routinely given extremely dangerous drugs or surgeries to “fix” that pain—even though, sadly they often just make it worse. In the second part of the series, I shared some of my perspectives on how to treat spinal pain.
A key foundation of that approach is that it’s necessary to restore the strength of the ligaments in the spine, as its ligaments stabilize it and prevent the joints from grinding each other down (at which point they become inflamed, lose their mobility and hurt). Unfortunately, the approach medicine uses to address this, injecting steroids into the joints to reduce the inflammation, in many ways is the worst thing you can do because steroids damage ligaments, and thus it’s quite common to see people who receive steroid injections for back pain progress to needing (often disastrous) spinal surgeries—something I believe in part is motivated by how incredibly lucrative those surgeries are.
Note: as you might guess, individuals with ligamentous laxity (e.g., EDS patients) frequently end up being subjected to harmful spinal surgeries, and in that article, I shared a few tragic cases of this happening.
In the final part of this article, I will discuss how many of the same approaches we use for other issues in the body (e.g., manganese protocols for spinal issues) can also be used for individuals with ligamentous laxity to strengthen their ligamentous integrity (which in addition to repairing the musculoskeletal system ofter creates a myriad of unexpected benefits).
