

The Forgotten Cancer Cure Hiding in Plain Sight
How DMSO turns a common dye into a highly potent cancer treatment that's harmless to normal tissue

Story at a Glance
•DMSO is a safe and naturally occurring substance that is remarkably effective for a wide range of diseases including pain, injuries, and strokes.
•DMSO effectively dissolves a variety of medications and can transport them throughout the body. This increases their potency, makes it possible to administer them through the skin, and allows them to target things deep within the body (e.g., resistant infections) that other therapies have difficulty reaching.
•Through various mechanisms, DMSO selectively targets cancer cells and simultaneously mitigates the consequences of cancer therapies. It also brings conventional and natural cancer therapies to tumors, thereby significantly increasing the potency of these therapies (while simultaneously allowing a much lower and less toxic dose to be used).
•When DMSO is combined with hematoxylin (a dye widely used in pathology), it becomes a highly potent cancer treatment, both harnessing DMSO’s intrinsic anticancer properties and directly destroying cancer cells. It is also highly specific to targeting cancers while not affecting normal cells, thereby allowing it to dissolve cancers at doses that have virtually no toxicity to the patient.
•Despite its ingredients being relatively easy to procure and producing remarkable results, this therapy (like many other alternative cancer treatments) was almost completely forgotten. Fortunately, a narrow thread of knowledge has kept this sixty-year-old discovery alive, most recently through a doctor who spent the last fifteen years refining this lost therapy and successfully treating cancer patients with it.
•This article will discuss everything known about DMSO-hematoxylin, such as its mechanisms, which cancers it responds to (e.g., it’s very effective for leukemias along with their associated anemias and can often treat advanced cancers no other treatment works for), and with how to use it both at home and within a medical setting.
Over the last six months, I’ve worked to bring the public’s attention to dimethyl sulfoxide (DMSO) a forgotten natural therapy which rapidly treats a wide range of conditions and that many studies have shown is very safe (provided it’s used correctly), and, most importantly (thanks to the 1994 DSHEA act which legalized all natural therapies) is now readily available. Since I believe DMSO has an immense amount to offer to the medical community and individual patients, I’ve thus diligently worked to compile the evidence that would best make the case for its rediscovery. As such, throughout this series, I’ve presented over a thousand studies that DMSO effectively treats:
Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
While unbelievable, consider for a moment this 1980 report by 60 Minutes that corroborates much of that:
Fortunately, much in the same way DMSO’s caught on in the 1960s, providing that evidence again has allowed it to make a rapid resurgence (e.g., I’ve now received over 2000 stories from readers who’ve often had remarkable improvements from using it).
Of the myriad of uses for DMSO, the least appreciated one is its applications in cancer due to the politics around “unproven” cancer therapies:
Dr. Stanley Jacob [the pioneer of DMSO] also is acquainted with Tucker’s work. In fact, he telephoned Tucker a few days before the Mike Wallace 60 Minutes show on CBS-TV to check out progress on the cancer treatment. Jacob plays down the DMSO-cancer connection, because he has enough trouble getting the substance recognized for all of its other special uses. He doesn’t want to have to fight off the label of “cancer quackery” as well.
As such, I recently published an article on DMSO’s remarkable properties for treating cancer and cited hundreds of studies showing that:
•DMSO causes a wide range of cancer cells to transform back into normal cells.
•DMSO slows the growth of many cancers.
•DMSO allows the immune system to target and eliminate cancers it previously was unable to remove.
•DMSO treats many challenging complications of cancer such as cancer pain and amyloidosis from multiple myeloma.
•DMSO protects tissue from radiation and chemotherapy injuries.
•DMSO makes many cancer therapies (e.g., radiation or chemotherapy) more potent, thereby ensuring both a higher treatment success rate and far less complications (as less toxic doses are being used).
Remarkably, despite DMSO’s anticancer properties routinely being used in lab experiments (including those seeking to find anticancer agents with those same anticancer properties), the cancer field has a striking blind spot to DMSO’s use, so in the existing literature, it is almost never discussed as a potential therapeutic.
Of these many uses, I believe the two most noteworthy are DMSO’s ability to mitigate the challenging complications of cancer (e.g., cancer pain or protecting healthy tissue from radiation therapy) and its ability to potentiate other anti-cancer agents.
Combination DMSO Therapies
One of the major advantages and risks of DMSO is that it can bring substances through the skin and significantly increase their potency in the body. On one hand, this is quite advantageous as it makes it possible to administer things which would otherwise require injections through the skin and for much lower doses of them to be needed to get results (e.g., as I showed here, antimicrobials mixed with DMSO are often able to treat a wide range of chronic infections which otherwise resist antimicrobial therapy). However, on the flip side, it greatly increases the risk of toxicity, either by accidentally bringing toxic compounds (e.g., pesticides) into the body that were on the skin prior to applying DMSO (or that were touched afterwards), or increasing the potency of a drug taken in combination with it.
Note: it is well known that healthcare workers who routinely administer chemotherapy periodically have accidental exposures to it (e.g., via vapor inhalation), so organizations like the CDC and NIOSH have worker guidelines about it (as these exposures increase the risk for a variety of issues including cancers). Since DMSO will cause chemotherapy drugs it is mixed with to be absorbed through the skin, it is crucial to be extremely cautious when administering it with chemotherapy drugs (particularly when applying it topically).
Since natural therapies are typically much less toxic than conventional pharmaceuticals and easily available (rather than requiring a prescription) over the years, people have tried combining DMSO with many of them and frequently found significant advantages from mixing them together DMSO.
This also holds true in the field of cancer care, and from reviewing all of the ways in which DMSO has been used to treat cancer, I believe the most promising applications (and which had the strongest data supporting their human use) came from DMSO being used in combination with another natural therapy. Unfortunately, the number of substances DMSO can be combined with is almost endless, and as such, the DMSO field has only scratched the surface of what it can be combined with to treat cancer. Many highly potent cancer treatments are likely waiting to be discovered once the right things are combined with DMSO.
Note: somewhat analogously, in the hundreds of studies I identified that examined if DMSO could differentiate a specific tumor type or improve a particular cancer-related gene (or protein), most of them found DMSO did create an improvement. As such, many other aspects of cancer would likely also be seen to improve following DMSO if they were to be tested.
Hematoxylin
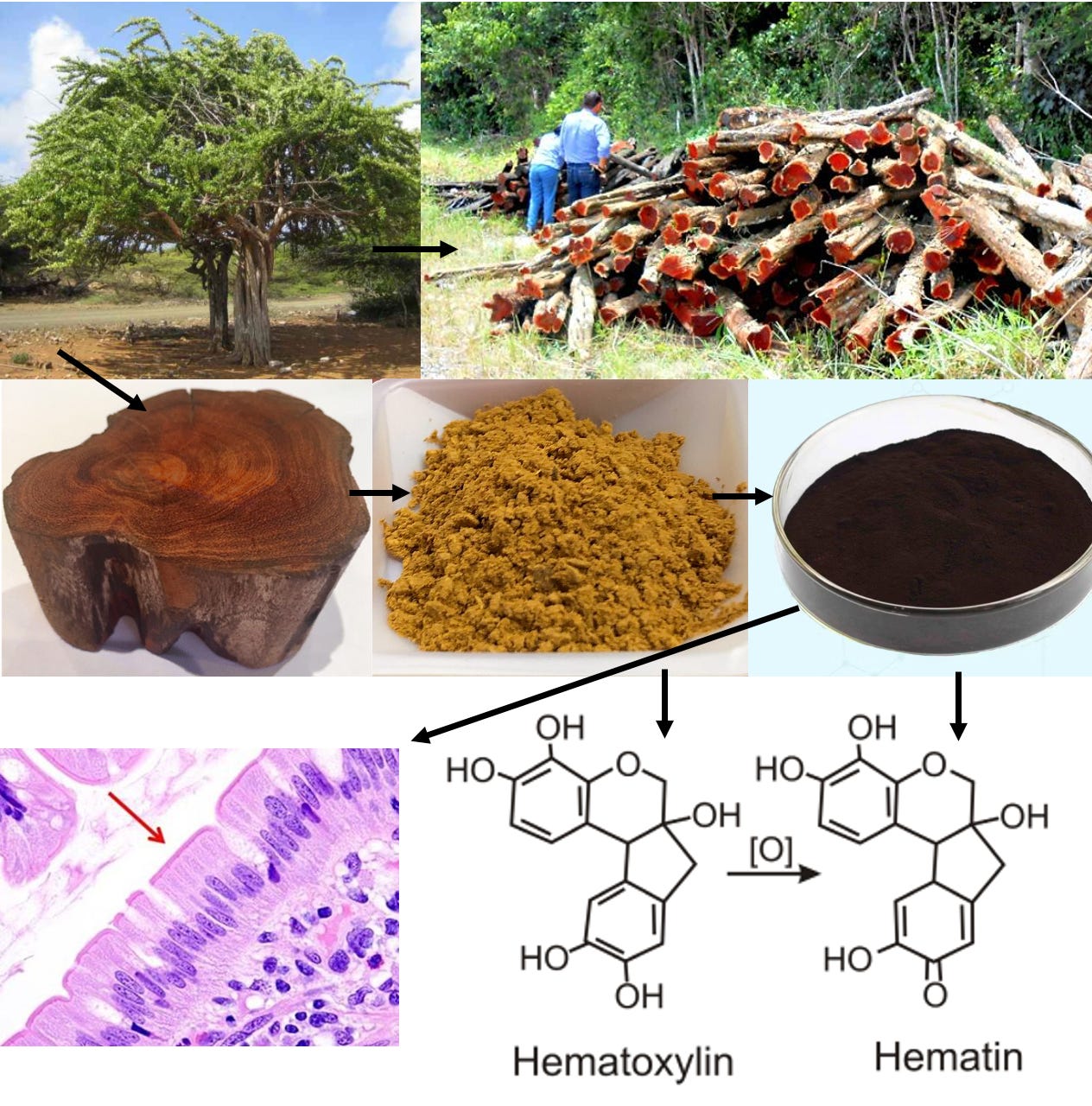
Hematoxylin is a powder obtained from the logwood tree (e.g., grinding the heartwood up, boiling it in water to dissolve the hematoxylin present, and evaporating that mixture so only the powder remains). That tree is native to Central America and was originally used by the Mayans to stain cotton and as a medicinal (e.g., to treat diarrhea and dysentery). After its discovery by the Spanish in 1502, a massive market for it quickly developed due to the textile industry’s need to establish a dependable dye. Before long it began to be mixed with a variety of metal salts so it would remain in fabric (and not wash out).
Since many cellular processes are transparent and hence difficult to see without dyes that can stain them, much later (around 1830) hematoxylin began to be used in pathology where it was discovered (once oxidized into hematein and attached to a metal salt) it was remarkably effective for staining many components of cells including DNA. In turn, because of how well it works, almost two hundred years later, it remains one of the primary stains used in pathology to evaluate tissue (it’s the “H” in H & E stains).
Note: like hematoxylin, DMSO is also obtained from trees. Because each of these compounds is so widely used, they are also very affordable.
Tucker’s Discovery
Currently, most of the drugs we use are developed by a mechanistic system where biologically relevant targets in the body (e.g., receptors or enzymes) are identified through research, then compounds are mass screened through for their ability to affect those targets, with the ones that can elicit some type of pertinent change then run through a funnel (which can involve animal and then sometimes human testing) to identify which from that large pool of candidates elicits a benefit.
Note: compounds are sometimes custom-designed to affect receptors or identified through AI systems rather than physically testing a broad swathe of them.
In contrast, previously, drug design was much more of a hit or miss process, and frequently incredible discoveries would happen either by luck or under a completely mistaken assumption.
For example, the first antibiotic was developed by mixing a substance known to be toxic to bacteria (arsenic) with a dye that stained bacterial cell walls under the theory that the dye would allow arsenic to selectively target bacteria rather than the body (with almost all the attempts failing). After decades of attempts were made to replicate this approach, another dye that functioned as an effective antibiotic was found, but before long it was discovered that the antimicrobial agent was not the dye itself but rather a colorless metabolic product of it, sulfanilamide.
Similarly, one of the most remarkable therapies I know of (Ultraviolet Blood Irradiation) was originally developed under the belief that exposing the entire circulation to UV light would sterilize the bloodstream and hence treat a lethal infection. This did not work (it killed the test dogs) but before long, the inventor accidentally only irradiated a small fraction of the dog’s blood and got a remarkable results as inputting a small amount of UV light into the circulation transforms human physiology and allows the self-healing capacity of the body to treat a wide range of illnesses (e.g. UVBI is a highly effective treatment for bacterial and viral infections, circulatory disorders and autoimmune diseases).
Hematoxylin likewise follows a similar journey. Eli Jordon Tucker, Jr., M.D. was a highly respected orthopedic surgeon in Texas (with many awards and honorary status in a numerous medical societies) who had a wealth of surgical experience and had discovered a variety of pioneering orthopedic techniques from bone research he conducted as a hobby (e.g., he gained renown for discovering how to graft bones from one species to another). Tucker’s bone research required him to purchase cattle from a meat packing company, and in the process, he noticed many of the cows butchers (and meat inspectors) were accepting for slaughter had large cancers covering their faces.
Observing those cancers made Tucker wonder if there was some type of cancer-resisting antibody in those cows, so he began administering extracts of their blood into lab rats and mice with cancers and observed anticancer activity for certain cancers. Since it was unclear how much of a change was occurring, Tucker looked for a dye that could stain the tumors, and eventually realized hematoxylin was the perfect dye because it stained the cancers one color and normal cells another color. Unfortunately, hematoxylin had poor solubility and could not dissolve in normal laboratory solvents or enter solutions, so his ability to use it in his experiments was limited.
So, once DMSO (a potent solvent), came into use around 1963, Tucker tried using it and quickly discovered DMSO not only dissolved hematoxylin but could dissolve a very high concentration of it (e.g., 25g of hematoxylin could be dissolved in 62mL of DMSO). Furthermore, this mixture was excellent for staining cancers and making them visible (e.g., they stood out under the microscope and in gross dissection) as it concentrated in the cancers, but DMSO simultaneously did not stain any other tissues in rats. Most importantly there was a “marked increase in central necrosis of the neoplasm” indicating this mixture could potentially eliminate cancers while sparing normal cells.
Note: hematoxylin (dissolved in carboxymethylcellulose), like many other compounds, had previously been screened for its anticancer activity and in the absence of DMSO, had none, which I suspect was in part due to hematoxylin rather than hematein (which hematoxylin rapidly turns into within the body) being used.
Tucker then decided to conduct toxicity studies (initially in dogs) where he found high concentrations of IV DMSO mixed with hematoxylin had no toxicity to any of the tissues or organs he examined (and did not accumulate in any non-cancerous tissue). Curiously the mixture he made was far less toxic than IV DMSO alone (which is extremely safe and only had toxicity issues at fairly high concentrations), with roughly four times as much IV DMSO being possible for animals to tolerate once it was mixed with hematoxylin.
Note: the only physiologic change he observed from D-hematoxylin was that blood urea nitrogen would typically drop by around 50%, indicating this mixture improved kidney function.
He then began treating spontaneous cancers in animals (e.g., in horses, dogs and cows), which included terminal cases with massive tumors (e.g., a large-cell lymphosarcoma, a small-cell lymphosarcoma, generalized malignant melanoma, a squamous cell carcinoma) along with an osteogenic sarcoma. In all of these cases, there was a prompt response, and the animal subsequently recovered.
Note: Tucker found that hematoxylin alone had no effect on cancer cells (as did previous researchers who tested iton a carcinoma, sarcoma and leukemia cell lines) while subsequent investigators found DMSO alone had a minimal anticancer effects compared to the mixture, whereas they could not administer hematoxylin alone (as without DMSO it is essentially not soluble in an IV solution). Going forward (for brevity) I will refer to the DMSO hematoxylin mixture as “D-hematoxylin” (which is a term I made up while writing this).
William Daniel, former Governor of Guam, one of Tucker’s friends, phoned and told the doctor: “E.J., I have a cancerous dog on my ranch who is suffering terribly. Could you do anything to help him, or should I have him put to death?”
“I’d love to try,” answered Tucker. “I’ll send my technician to pick up the dog right away.”
The technician brought the animal to Tucker’s veterinarian, Dr. Collins, for examination. The vet diagnosed that large-cell lymphosarcoma was permeating the dog’s body. “The poor animal is choking to death from the tumors in his throat, and he has large tumors all over his body,” said Dr. Collins over the telephone. “I don’t think he’ll live long enough to be transported to your laboratory.”
Tucker said, “Transfuse him, give him some blood fast, and let me have him for treatment.”
The physician took the dog, which was barely alive, into the laboratory and injected DMSO-hematoxylon solution intravenously. His technician took over the work and gave the injections daily. Within two weeks, all the tumors had disappeared. It seemed like a miracle to the technician.
Upon Tucker’s examination of the dog, he found that all the large-cell lymphosarcoma tumors had completely regressed. The huge masses in the neck and over the whole body of the animal had gone away, and the dog came out of the treatment completely cured.
The dog was thriving at the laboratory when an unlucky accident caused his death. He ate a large quantity of some meat contaminated with Malathion, an insecticide poison. Tucker performed an autopsy, which revealed no active cancer cells in the vestigial remains of the previously large lymphomatous nodules. Many ghost cells—cells that were formerly cancer but weren’t any kind of cells anymore —appeared in the microscopic sections. Not a single distinguishable cancer cell remained in the dog.
Additionally, in 2019, long after Tucker conducted his toxicity experiments, to help the Ecuador team, Roger Tapia, a veterinary student conducted his own LD50 study as a graduation thesis by giving intraperitoneal injections of D-hematoxylin to 70 mice and determined that:
•The D-hematoxylin LD50 was 1257.16 mg/kg of hematoxylin (± 159.10 mg/kg), which is very safe (and between 10 to 100 times less toxic than many commonly used cancer drugs).
Note: the LD50 of hematoxylin alone is also fairly low (e.g., the oral LD50 is over 2000mg/kg), but relatively little data exits on its actual LD50 as it is not intended for human consumption (e.g., data only exists for the oral LD50 and the actual LD50 is unknown as a high enough dose to be lethal to half of those exposed was never tested).
•At lower doses (e.g., 5.5mg/kg to 550mg/kg) low activity, tremors and accelerated breathing were observed that regressed after an hour, while at higher doses, spasms, suffocation and eventually death occurred (likely due to respiratory collapse).
Note: the authors of the study suspected these symptoms were likely due to the shock of an intraperitoneal injection and it being injected too quickly (all of which can be avoided with a careful IV administration).
•In rats that died, the presence of fluid accumulation was observed in the abdominal cavity and surrounding the lungs which was attributed to vasodilation and increased vascular fragility.
•At all doses (including lethal ones), the mixture did not produce any changes in the shape, weight, or size of the internal organs (which I assumed was due to the fact D-hematoxylin does not accumulate in normal tissues).
The full study can be read here:
Note: while Tucker found IV DMSO with hematoxylin was a fourth as toxic as DMSO alone, when I compared the IP (intraperitoneal) LD50 value this study obtained to the recognized LD50 values for DMSO, I found DMSO alone was less toxic.
Tucker’s Patients
From these experiments, Tucker gradually determined a workable dosing for D-hematoxylin and hence was prepared to administer it to humans. He began telling his hospital associates of his findings, and before long was approached by a colleague who had a comatose female patient on the verge of dying from inoperable fibrosarcoma. As she was his first human patient, Tucker gave her a very slow infusion, and over weeks of treatment, the tumor gradually receded until it was small enough to remove (at which point she had a full recovery).
Note: in our modern medical bureaucracy a treatment like this most likely could have never gotten approval.
Following this, he treated numerous patients, and due to the FDA banning DMSO research in 1965, conducted a small trial in Panama with a colleague. After much difficulty, in 1968, he got his cases published. There he reported on 37 patients he’d treated with recurrent cancers (excluding those who were terminal or those with markedly elevated BUN). Of them, 70.5% of those who were also on another treatment (radiation, surgery or chemotherapy such as 5-fluorouracil (5FU), methotrexate, and thiotepa) improved, 38.1% who received hematoxylin improved (typically only their symptoms but there was one case of a leiomyosarcoma regressing and being surgically removed) while only 5.4% of those receiving conventional therapy improved.
Younger patients with aggressive cancers generally responded better than older ones, as did those with minimal or no prior chemotherapy and those receiving higher total doses (e.g., 50 infusions) or combined topical and IV D-hematoxylin.
Note: over the decades Tucker was reported to have given his mixture intravenously, orally, intralesionally, intra-arterially, rectally, and topically (with topical applications of D-hematoxylin being particularly helpful for cervical cancer). Conversely, subsequent doctors I’ve spoken to (who found those routes of administration worked) made the obvious conclusion to try injecting D-hematoxylin into tumors, but oddly (in their limited attempts) never found that route worked.
In contrast, patients with more terminal conditions had worse outcomes (something which has held true with virtually every alternative cancer therapy—which is unfortunate since they only get approved for use in terminal cases after everything else failed). Additionally, patients with large-cell lymphosarcoma, giant-cell bone tumors, leiomyosarcoma, and adenocarcinomas of the breast or ovary showed positive responses to D-hematoxylin, while those with squamous-cell carcinomas (cervix, lung, or mouth) and adenocarcinomas (prostate, stomach) exhibited minor positive responses but ultimately succumbed to their cancer.
Note: another author reported D-hematoxylin was effective against squamous cell carcinoma, adenocarcinoma, lymphosarcoma, lymphoma, and such associated malignancies such as Hodgkin’s disease.
Many of these cases were quite noteworthy. Both large-cell lymphosarcoma cases showed complete regression with no recurrence well beyond Tucker's June 1968 report (one patient died from a heart attack ten years later, while the other remained alive decades later). Additionally, one case of malignant giant-cell tumor, affecting about one-third of the femur, experienced complete regression alongside new bone regeneration.
•Finally, in those 37 cases, complications were minimal (including in one patient who was continually assessed over the course of 72 [2mL] of D-hematoxylin treatments). The most common side-effect in Tucker’s patients were fevers in patients with large tumors (which typically lasted around 35 minutes and were less severe if smaller doses were used or the tumor had begun to shrink). Additionally, if D-hematoxylin was infused too quickly, a few patients developed shortness of breath (which immediately resolved if the infusion was stopped and Demerol was administered). Rashes could also sometimes occur (which were suspected to be due to the absorption of necrotic tumor material). The most severe complications occurred from absorbing large amounts of necrotic tissue matter (e.g., terminal patients with high uric acid levels would stop urinating once too much tumor necrosis occurred) so Tucker was much more cautious with these cases and used smaller doses so he did not eliminate the tumor too quickly. Finally, no changes were observed in the eyes (which was a longstanding unfounded concern about DMSO) or blood cell counts (which is a common issue with chemotherapy).
Note: since this paper (which includes many detailed patient cases) is quite hard to find online, I am including a copy of it.
Sadly, after Tucker published that article, the American Cancer Society (in 1971) published a bulletin it sent to all 58 of its divisions stating D-hematoxylin was an “unproven” remedy which provided very little of substance to refute its efficacy and simultaneously made no mention of any potential toxicity (suggesting D-hematoxylin is quite safe as any signs toxicity would have been used to discredit the therapy). Tucker sadly received so much pushback from his colleagues for using an “unapproved drug” (e.g., despite having earned great respect in the medical community, he was expelled from the staffs of two hospitals for administering the treatment and had a real fear of losing his medical license) so he never published anything further. Similarly, he became much more selective in who he would treat (e.g., only pre-terminal patients and those in a destitute state), and typically did so either for free or a very minimal fee (but nonetheless successfully treated many cancer patients in the years that followed).
Note: Andrew Ivy (who was arguably the most influential doctor in America at the end of World War 2), like Tucker theorized there must be a factor in the blood which resisted cancer, and eventually came across a isolate (from cows injected with a cancer causing fungus who’d then recovered) which did just that. After refusing to sell out to the AMA (who frequently tried to buy out competing therapies), he was blacklisted by both the FDA and AMA, and despite having thousands of compelling and well documented cases showing it worked, effectively had his entire reputation destroyed because he’d promoted an “unproven cancer cure.”
Some of Tucker’s other patients included:
•A 3-year-old boy with diabetes insipidus (which requires routine vasopressin injections) who in 1972 had a terminal case of metastatic endothelioma and Letterer-Siwe disease, where solid palpable cancerous lesions had spread throughout the boy’s head and body, which his doctors had given up on and expected him to die within a few years. Even worse, the father abandoned them to escape confronting the cancer, leaving the mother destitute and struggling to survive. Tucker then gave the boy’s desperate mother a dropper bottle of D-hematoxylin to take 5 drops in distilled water every morning on an empty stomach and instructed her to let her doctors know what she was doing.
Mrs. Lindsey returned the next day totally distraught. Between heavy sobs and tears, she explained how the Texas Children's Hospital staff became enraged and told her never to come back if she used Tucker's medicine for her son's cancer. This meant that her supply of Pitressin for treating the little boy's water diabetes was completely cut off, since she had no money with which to buy more.
This scene took place within earshot of other patients sitting in Tucker's reception room. They passed the hat and in a couple of minutes raised $75 for the mother to buy her child's diabetic medicine.
Fortunately, Tucker’s treatment worked, the boy fully recovered (much to the shock of his ENT doctor who’d diagnosed him as terminal) and when last checked on in 1992 was a large, strong, and healthy 29 year-old boy.
•A woman who’d a seen a three hour 1972 news program by anchorman Ron Stone of KHOU-TV Houston about Tucker’s treatments who sought him out as she had a disseminated large-cell lymphosarcoma (e.g., sizable tumors in her lungs, the common iliac arteries, and the lymph nodes around her aorta) with an expected six month survival (which she had been on high doses of radiation and chemotherapy to no avail for and eventually had to stop the chemotherapy due to a very low white blood cell count). Tucker started her on five D-hematoxylin infusions a week, she stopped experiencing negative side effects from radiation, and a year later was completely cured (and remained so after 28 years of follow-up).
Note: if anyone in Houston can get a copy of that news program from the station (which I know happened as it was mentioned by multiple DMSO authors who provided different details about it), it would be greatly appreciated.
•A 41-year old man with a disseminated lymphosarcoma which had failed treatment with maximum radiation and chemotherapy who was expected to only survive for three more months. He received IV D-hematoxylin every other day for three months, after which the tumor completely disappeared, the man stopped further treatment, and had no recurrence up to his death eight years later (from a heart attack).
•A 44-year old man with advanced lymphosarcoma (including a massive lump on his neck) who had been treated for five years with maximum doses of radiation and chemotherapy (which amongst other things left him with an almost complete absence of white blood cells). Daily IV D-hematoxylin shrank his neck tumor from 22.5 inches to 18.75 inches (which was enough for his neck to return to a normal appearance), but he subsequently succumbed to the cancer as he had metastasis throughout his internal organs.
•A 36-year-old man with terminal grade 4 Hodgkin’s disease (e.g., large cancerous nodules on his neck and face, severe swelling in his abdomen and legs, and congestive heart failure) was admitted to the hospital with a prognosis of only days to live. He received D-hematoxylin intravenously and topically over his lungs and after four days, he was well enough to return home. Without continued treatment, his breathing difficulties returned, so he returned to the hospital and had a rapid response to D-hematoxylin (e.g., initial X-rays showed on May 22 showed near-total lung obstruction, but by May 25 a slight clearing appeared, and by July 18 the cancer had disappeared entirely). Following treatment, he remained cancer free until he later died from heart failure.
•A 75-year-old man who, in 1984, had a recurrent squamous cell carcinoma on the nose (where one had previously been removed 3 year prior) applied topical D-hematoxylin and within a few weeks, the cancer disappeared and the nose was saved from a disfiguring surgery.
Later, in March 1978, Tucker was invited by a group of New York City doctors to share his treatment. En route, K.C. Pani, M.D. of the FDA, requested that Tucker share his data with Dr. Pani (Tucker had numerous records of cures, X-ray films, and slides to show).
On this trip, Tucker brought Joe Floyd, an Exxon Oil Corporate Executive, who four years earlier had had an advanced metastatic colon cancer (e.g., in the lymph nodes and liver) with a poor prognosis (particularly since it was a rare lymphosarcoma). Following surgery, he was implored to start chemotherapy (by a surgeon whose wife had the same condition) but instead sought out Tucker (as he’d seen the 1972 news program two years earlier). Tucker eventually agreed to treat him on an experimental basis (with both IV D-hematoxylin and daily oral D-hematoxylin). While Floyd’s surgeon’s wife died six weeks later, Floyd “ had no nausea or any of the symptoms usually accompanying chemotherapy” and after 18 months, his CEA levels (a marker for colon cancer) were far below normal, and in the years that followed never rebounded (and likewise over 15 years of followup did not either).
Doctor and patient flew to Rockville, where Tucker presented his case histories to the FDA.
When they came to Floyd’s record, Dr. Pani asked, “How long did this one last, three months?”
Tucker replied, “He is sitting down in the lobby.”
Pani said, “I want to see this dead man.”
They sought out Mr. Floyd, and he told his story. Then the FDA official, visibly impressed, said he would be in touch with Tucker soon. He also mentioned that he was in contact with Dr. Stanley Jacob of Oregon and that he was monitoring the use of DMSO. About one week later the drug was approved for the treatment of interstitial cystitis. Nothing further was done to follow up its use in cancer, except that Tucker received a request from the FDA for “more research.”
Note: the FDA had briefly given Tucker permission to study D-hematoxylin in 1970 but withdrew that permission later that year.
Floyd also attempted to reach many other outlets. A letter he wrote to a newspaper, for example, was published in a record of a 1980 hearing Congress held to pressure the FDA to legalize DMSO, part of which said:
While I had been taking treatments from Dr. Tucker I met many of his patients who came by for check ups that he had cured. You can imagine how excited I became over this treatment. I wanted to do something so everybody with cancer could get this drug. I preached it to my friends and acquaintances but alas when one would mention it to their personal physicians, they wouldn’t touch it, especially if it wasn't approved for general use, the hospitals would not let them use it even if they wanted to. I started writing to Congressmen, would get a Thank You letter with a Rubber Stamp signature. Even when Hubert Humphrey was dying I wrote him a letter, but back came another Thank You with Hubert’s rubber stamp signature.
Next I wrote Jimmy Carter, thinking someone in the White House might see the political possibilities and pass it on to him. But no, it was side tracked over to the FDA. Excitement, the answer did have a real signature, “Harold Davis” Bureau of Drugs (HFD—35). It was the nice “Thank You for concern but we have to protect the people from quackery etc.” He even sent me a brochure by Dr’s Tucker and A. Carrizo [the other author of Tucker’s 1968 paper], the same as I am enclosing for you that Dr. Tucker gave me.
Note: in this letter, Floyd also shared that he saw many “people that started the treatment too late but died without pain, thanks to the DMSO,” an observation also made by modern doctors using D-hematoxylin, and which was demonstrated in three recent studies where IV DMSO was combined with sodium bicarbonate.
Lastly, a few other American doctors besides Tucker also used his treatment (including a few that I know did so recently). However, the only documented case I know of where someone besides Tucker used D-hematoxylin was of a 55-year-old Texas Baptist minister who in 1982 had a tennis ball-sized mass under his ribs which was diagnosed as malignant lymphoma and began receiving large numbers of daily blood draws alongside initiating chemotherapy (chlorambucil). He quickly developed multiple significant symptoms (including the previously painless mass becoming painful), at which point a health food store referred him to a natural cancer clinic (Jasper County Medical Center) where he worked with clinical nutritionist Dr. John Meyer who placed him a mix of natural therapies alongside the clinic giving him both oral and IV D-hematoxylin and proceeded to make a full recovery (during which he quickly noticed chlorambucil made him violently ill and permanently stopped taking it).
Hematoxylin Persists
When DMSO was first discovered, due to its significant positive results, it was the most requested drug in America, and many pharmaceutical companies made substantial investments in researching to bring it to market and recruited roughly 1,500 clinicians to conduct their research. In early 1965, Merck contacted the American Podiatry Association to request their top podiatrists (foot doctors) for their trials. Morton Walker DPM was selected as he’d recently won numerous awards for his scholarship and previous clinical investigations.
He began his research in the spring of 1965 and rapidly saw great benefit in the patients he treated, but unfortunately, that fall, the FDA decided to force the pharmaceutical companies to end all research into DMSO (which, as best as I can gather, was initially due to the fact that the agency did not want to deal with a large number of applications for the myriad of conditions DMSO treated).
This podiatric study of DMSO came to an abrupt halt November 10, 1965, when a “Dear Doctor” letter arrived advising that all research on the project must cease. The FDA demanded that the used and unused supplies of DMSO and all records of patients for whom it was administered must immediately be returned to the sponsoring pharmaceutical company.
I didn’t have to mail these items because a company representative promptly arrived to take everything away—all patient reports, supplies of DMSO, even duplicates of the records. Instructions were given to report any deleterious effects from the product’s use, but there were none. No published report ever appeared in the medical literature on this four-month podiatric study of DMSO’s adaptation for a variety of foot problems. All the records of clinical trial were confiscated, and what follows are strictly the impressions of this researcher twenty-seven years later. They are based on the patients’ personal foot health histories with relation to their individual toe, foot, ankle, or leg problems.
Following this, Dr. Morton Walker became a holistic journalist, and arguably was one of the most prolific people in the genre, compiling dozens of books on the natural therapies being used around the country (many of which I read decades ago). Amongst other things, Walker felt it was critical for Tucker’s work to be preserved, and as such, much of this article was sourced from his 1983 book on DMSO (which was written jointly with William Campbell Douglass MD—a pioneer in the alternative medical field), its 1993 revision, and his 1985 booklet on Holistic Cancer care which was written with John L. Sessions, D.O. (along with a book by journalist Pat McGrady).
On an ironic note, Dr. Tucker himself came down with a form of cancer that would have responded to his DMSO-hematoxylon treatment, but before he could administer it to himself, he fell into a coma. No one had access to his formula except the author of this book, and I did not know Dr. Tucker’s attendants needed it to save his life. Dr. Tucker died [on February 7 1983] only a few months before this book was first published. Its updating and republication may save lives—I hope so!
As such, Walker was able to preserve Tucker’s formula and make a thread of it available to the next generation who chose to search for it.
Jim McCann
There were a few eclectic individuals (some of whom I studied under) who were inventors with science backgrounds who dedicated themselves to collecting many alternative technologies, some of which were medical in nature. One of these men was Jim McCann, a cantankerous Canadian engineer and Jehovah’s Witness born in 1932 who’d created a variety of inventions throughout his life (e.g., a more efficient automobile engine).
On the medical end, at 23, McCann also started researching cancer cures, and about a decade later, adopted DMSO as it hit America. After he learned about D-hematoxylin through Tucker’s 1968 paper, he tried to get ahold of hematoxylin but initially was unable to as access was restricted at that time (and instead focused on EDTA chelation therapy). Eventually, around 1985 he did, at which point he used it on a prostate cancer patient who was on the verge of death, where unsure of what to do, he used a high dose that resulted in a full recovery.
Following this, he treated a few other people in Canada (approximately five), received significant pushback from the alternative medical community for practicing medicine without a license, and in 1995, moved to Riobamba, a town high in the mountains of Ecuador.
Initially, he used DMSO (and chelation therapies like EDTA) to treat stroke and heart conditions, but eventually began also using D-hematoxylin. Since he got results, doctors began seeking him out, and ultimately directly trained approximately 20 doctors (some of whom were not from Ecuador such as a Polish doctor and a doctor from the Philippines who attracted significant attention for successfully treating many COVID patients with ivermectin) along with many patients from around the world (and many Jehovah’s Witnesses from McCann’s community). As a result, Ecuador became a hotbed for alternative therapies, and in McCann’s estimate, roughly 100 doctors there (many of whom he’d never directly trained) began using D-Hematoxylin.
Near the end of his life (at the age of 90) McCann agreed to conduct a lucid interview with one doctor who took ten hour bus rides to see him (which a few parts of can be listened to below).
In it McCann shared:
•Many of the D-hematoxylin doses he used (especially the initial ones) were on the high end because he felt the patient would die soon regardless, so it was worth gambling on a potentially toxic dose to cure them.
•McCann believed a key part of the treatment was D-hematoxylin inducing a 103 degree fever in the body, and that it was critical not to use a fever-suppressing medicine to treat that fever or be in air conditioned rooms. However, in cases where patients did experience a significant reaction, he would administer Benadryl.
Note: This mirrors a viewpoint within the integrative cancer field that fevers are often critical for eliminating fevers (to the point that some groups cure cancer by inducing high fevers) and the anthroposophic perspective that suppressing febrile childhood illnesses with vaccination increases the risk of cancer later in life (which has been shown in quite a few studies regarding measles, mumps, and chickenpox).
•McCann felt strongly that an IV infusion of DMSO should never be combined with prednisone or a blood thinner like warfarin and heparin as this could make them far too potent (e.g., he saw this cause numerous severe adverse reactions after doctors administered mixed infusions against his advice).
Note: the reactions McCann described I have never heard of occurring in patients who were taking DMSO and one of those medications concurrently (e.g., a few DMSO studies I reviewed used topical DMSO combined with heparin found it was a helpful and side-effect free intervention) and I suspect the results McCann saw were from those drugs directly being mixed together with hematoxylin in an IV.
•He felt very strongly about the necessity of chelation therapy in cancer (e.g., to prevent subsequent heart attacks following successful D-hematoxylin treatments—which occurred years later in some of Tucker’s cases) and to that you should not give leukemia patients with anemia iron as the cancer needed that to grow (to the point he would sometimes also chelate iron in leukemic patients).
•McCann was also very focused on cultivating bacteria on a target media that would dissolve specific biological targets (e.g., he cultured bacteria from a dead cow’s cataract and then found it could eliminate other cataracts; likewise, he found this approach worked for cancer).
Note: my experience with individuals like McCann is that some of their insights are spot on while others they have a deep conviction in are ultimately not correct.
The Next Phase
Like many alternative therapies, D-hematoxylin grew up in “the Wild West” of alternative medicine. This was made possible by its very low toxicity profile, which allowed it to be used in humans at widely varying doses without significant side effects.
Fortunately, the threads keeping D-hematoxylin from being lost eventually converged in Ecuador with a doctor who’d successfully treated 44 out of 45 cases of microbiologically confirmed chronic bacterial prostatitis using DMSO combined with antibiotics that were applied directly into the bladder (much in the same DMSO is FDA approved to treat interstitial cystitis) who then tested negative for any infection 15-20 days following treatment (with no subsequent recurrences), demonstrating DMSO's ability to counteract bacterial resistance.
Note: interestingly, Stanley Jacob, was still alive when these treatments were initiated (he died in 2019 at age 91). At the start of the prostatitis treatments, the doctor in Ecuador contacted him for advice, and Jacob encouraged the experiment, agreeing it was a good idea, even though he hadn't heard of anyone attempting it before.
As he’d heard of McCann through Ecuador’s medical community, these prostatitis successes inspired that doctor to try intravesical DMSO mixed with hematoxylin for a prostate cancer patient (which was administered in the same manner and frequency as his prostatitis treatments). This worked, and he gradually began using it for other prostate cancer patients and then other cancers as well, which gradually grew into a fifteen-year research project on the therapy (which he's shared with me over the course of a few months).
Note: I also know of one individual who used D-hematoxylin intrarectally over a prolonged period to locally treat a cancer there, but the data on this approach is still limited.
Recent D-Hematoxylin Patients
That project involved treating approximately 85 patients, with the cure rate in patients who had not previously received chemotherapy averaging between 80-90%. As such D-hematoxylin is an excellent cancer treatment but it is not perfect and will not work for everyone.
Note: during these treatments, no significant side effects (e.g., signs of organ damage) were ever observed from D-hematoxylin.
The cancers with a good response to D-hematoxylin (some of which are otherwise extremely difficult to treat) included:
•Leukemias (particularly acute leukemia)
•Sarcomas (including soft tissue sarcomas and osteosarcoma)
•Leiomyosarcoma
•Bile duct cancer
•Non-Hodgkin lymphoma
•Ovarian carcinoma
•Mediastinal tumors
•Bladder cancer
•Cancers with a giant cell tumor phenotype
Note: myeloproliferative neoplasms (e.g., polycythemia vera, essential thrombocythemia and primary myelofibrosis) depend upon a mutant protein for survival which was shown to be susceptible to disruption by a few small compounds including hematoxylin. While D-hematoxylin has not been tested on these disorders, this study (along with the other known effects of DMSO and D-hematoxylin) suggest it could be an effective treatment for them.
The cancers with a poorer response included:
•“Solid” tumors
•Lung Cancer
•Colon Cancer
•Gastric Cancer
•Melanoma
•Bone Metastases
•Brain Cancer (requires longer treatment)
Additionally, if there is a cancer marker associated with the tumor (e.g., CEA or PSA), it will often rapidly drop, making it very easy to track the progress of D-hematoxylin.
Note: there can be an initial increase in the tumor marker (due to the cancer breaking down and releasing its components to the bloodstream) but this quickly goes down.
As the following cases show, many of the improvements were quite profound:
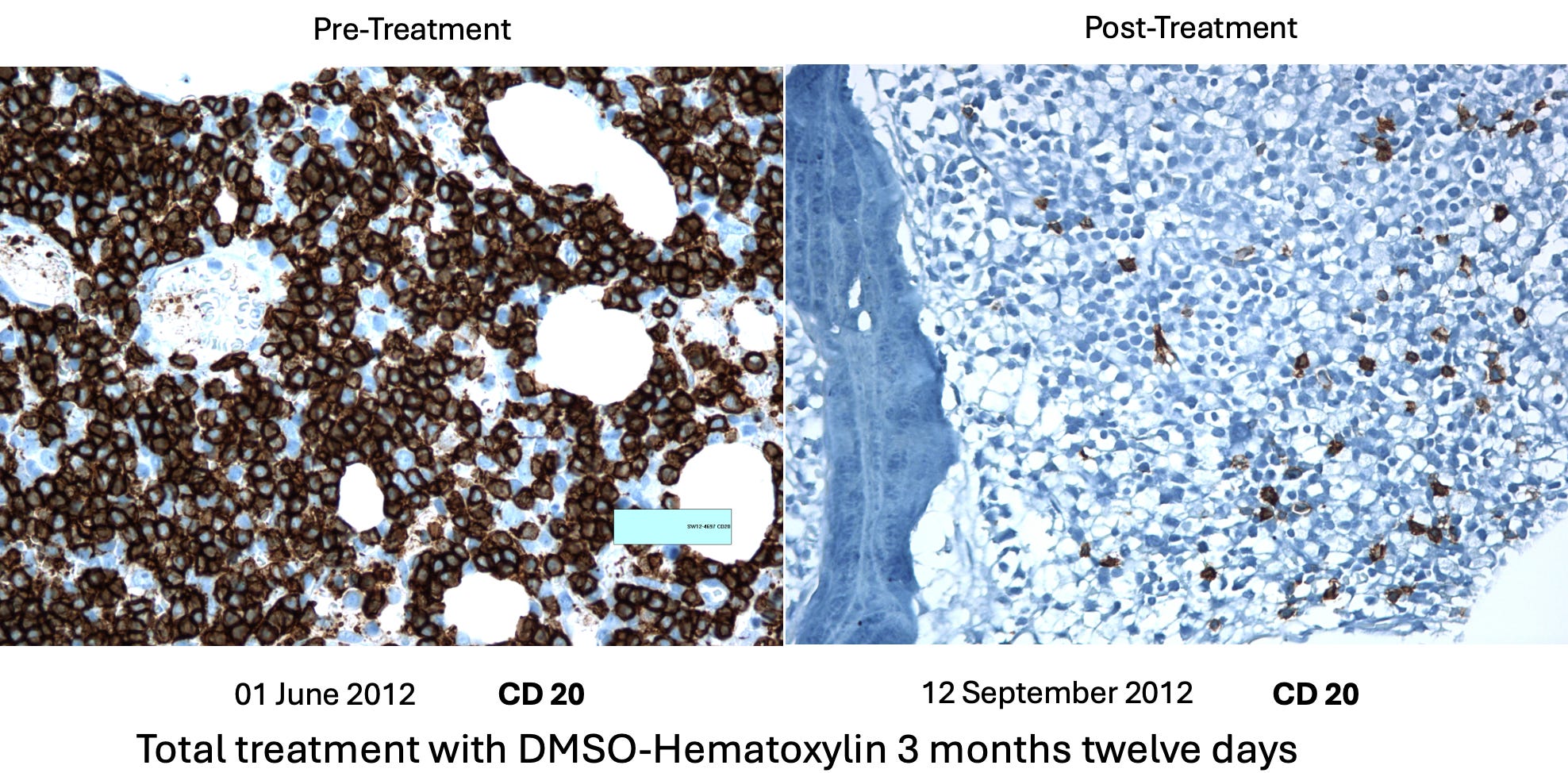
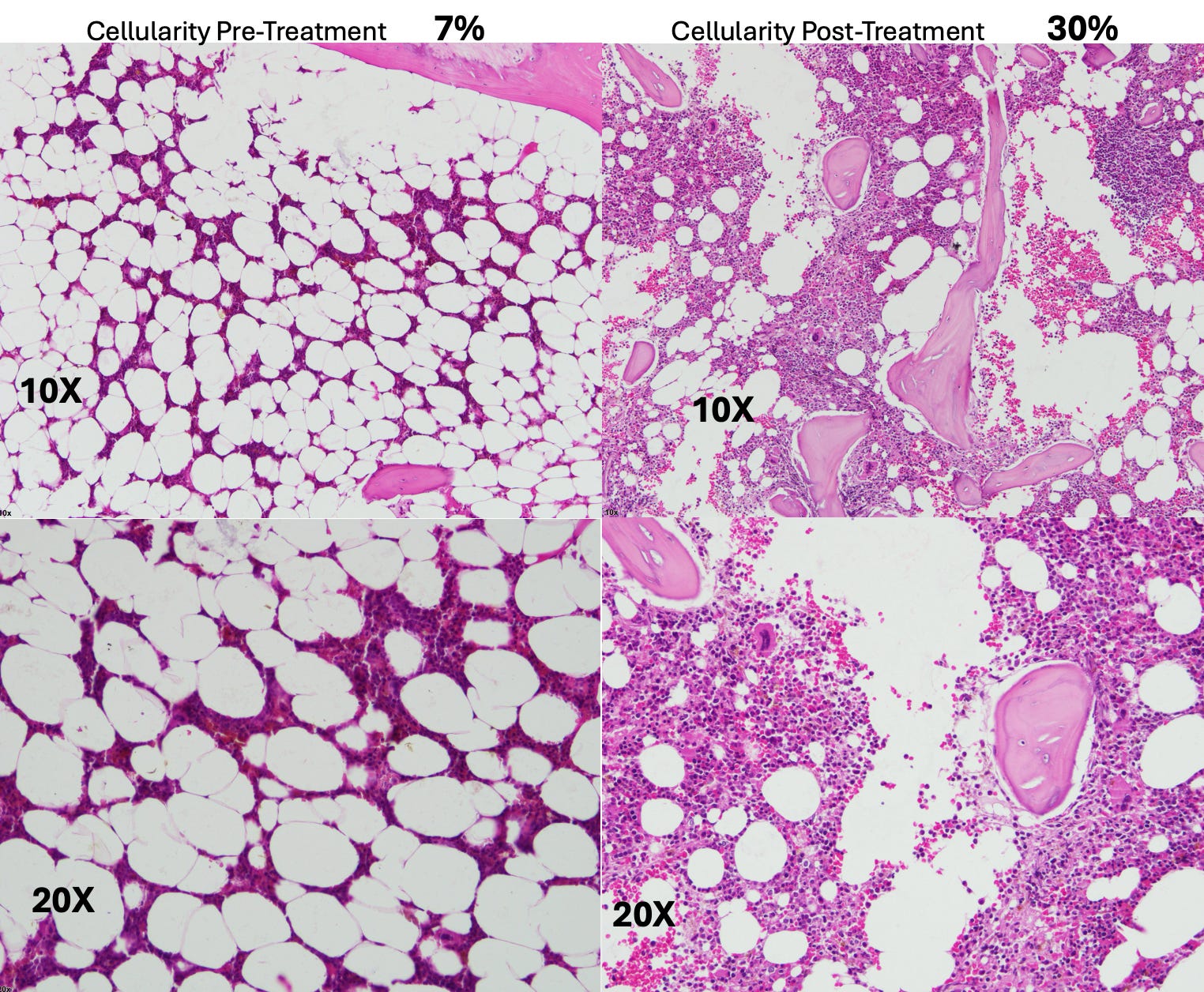
•A 54-year-old female patient with Classic Hodgkin Lymphoma which had invaded 72% of her bone marrow, with CD20-positive expression. She had a variety of symptoms (e.g., recurrent pleural effusions and anemia), but since her religion did not permit blood transfusions, she received only D-hematoxylin and EDTA and then had a full recovery (with no recurrence in twelve years of follow up). The most striking aspect of this case was the change in her bone marrow biopsy, after three months of treatment with D-hematoxylin (unlike chemotherapy) it selectively destroyed the cancerous cells, allowing normal ones to regrow and rapidly addressed her anemia.
•A 72 year old patient with leukemia who was anemic and had her anemia rapidly improve following D-hematoxylin:
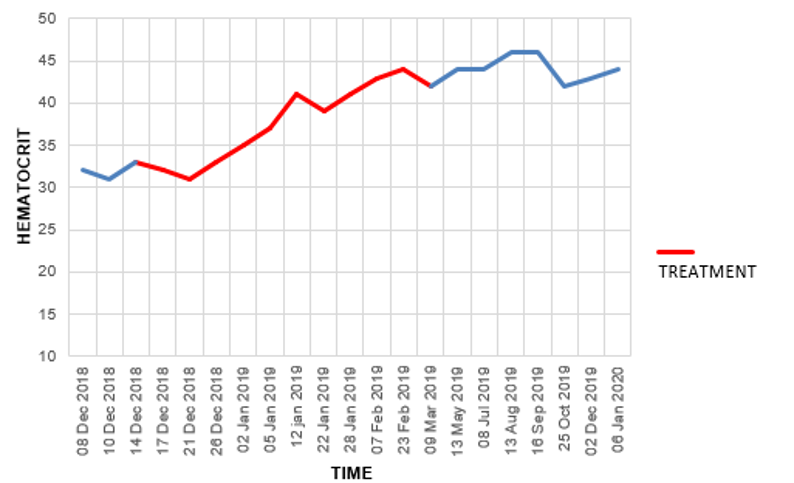
Likewise, similar bone marrow changes were seen in her.
Note: another similar leukemic patient on D-hematoxylin with anemia had no improvement. After investigating, it was determined this was due to her regularly using WD40 on a daily basis (without respiratory protection) and hence having a bone marrow intoxication which was directly damaging the bone marrow (and in turn the leukemia diagnosis may have been incorrect).
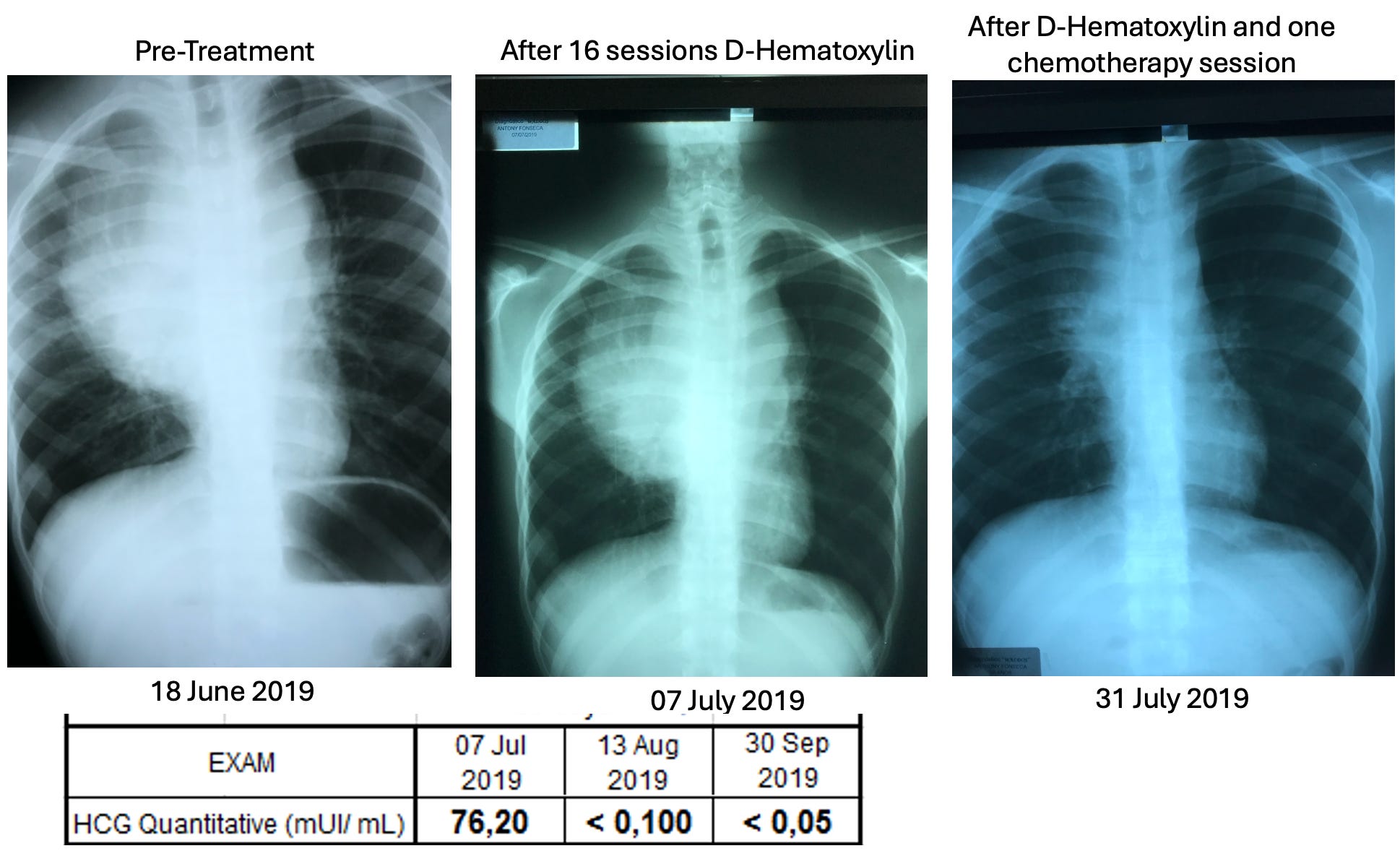
•A 16 year old male with a mediastinal seminoma that received 16 D-hematoxylin infusions, 5 IV vitamin C infusions and then one chemotherapy session (on July 7) where cisplatin and bleomycin were combined with DMSO (after which he continued chemotherapy and has recovered from the cancer).
•A 63-year-old male with cholangiocarcinoma (a rare, aggressive and notoriously difficult to treat cancer of the bile duct) who received D-hematoxylin plus chelation and vitamin C (but no chemotherapy). During his successful treatment, a drain from his bile duct was also monitored for tumor markers.

Additionally, the cancer debris could be seen in the drainage tube (an internal-external percutaneous transhepatic biliary drainage catheter)—something which the Ecuador doctors now view as essential to have if D-hematoxylin will be used in this cancer:

Note: another bile duct cancer patient (a 68 year old female) received palliative D-hematoxylin while waiting for surgery and chemotherapy (which ultimately could not be done because of how advanced the cancer was). Her cancer markers levels significantly improved following D-hematoxylin (and continued to reduce during gaps in treatment), but she eventually lost the will to live and passed after 16 months.

•A 63-year-old man with B-cell lymphoproliferative disorder who received D-hematoxylin for 10 days (with no other treatment), experienced a significant drop (normalization) of his white blood cell count during that time then stopped at the advice of his hematologists, and two years later died from COVID.
•A man who had a stable bladder polyp which became cancerous following a covid vaccination (with the initial sign being a large blood clot in the urine) which when examined had spread in a large portion of the urinary tract’s endothelium. It was surgically removed, but due to how far it had spread, the urologist told the patient he would only survive for two months. They then began five weeks of intravesical and IV D-hematoxylin, and in four years, the cancer never returned (which led to the urologist telling everyone about the “amazing” surgical procedure they had performed).
•A 55-year-old female who had a mediastinal tumor (type unknown as it was wrapped 560° around the aorta and hence could not be biopsied) which fully resolved after 33 daily D-hematoxylin treatments.
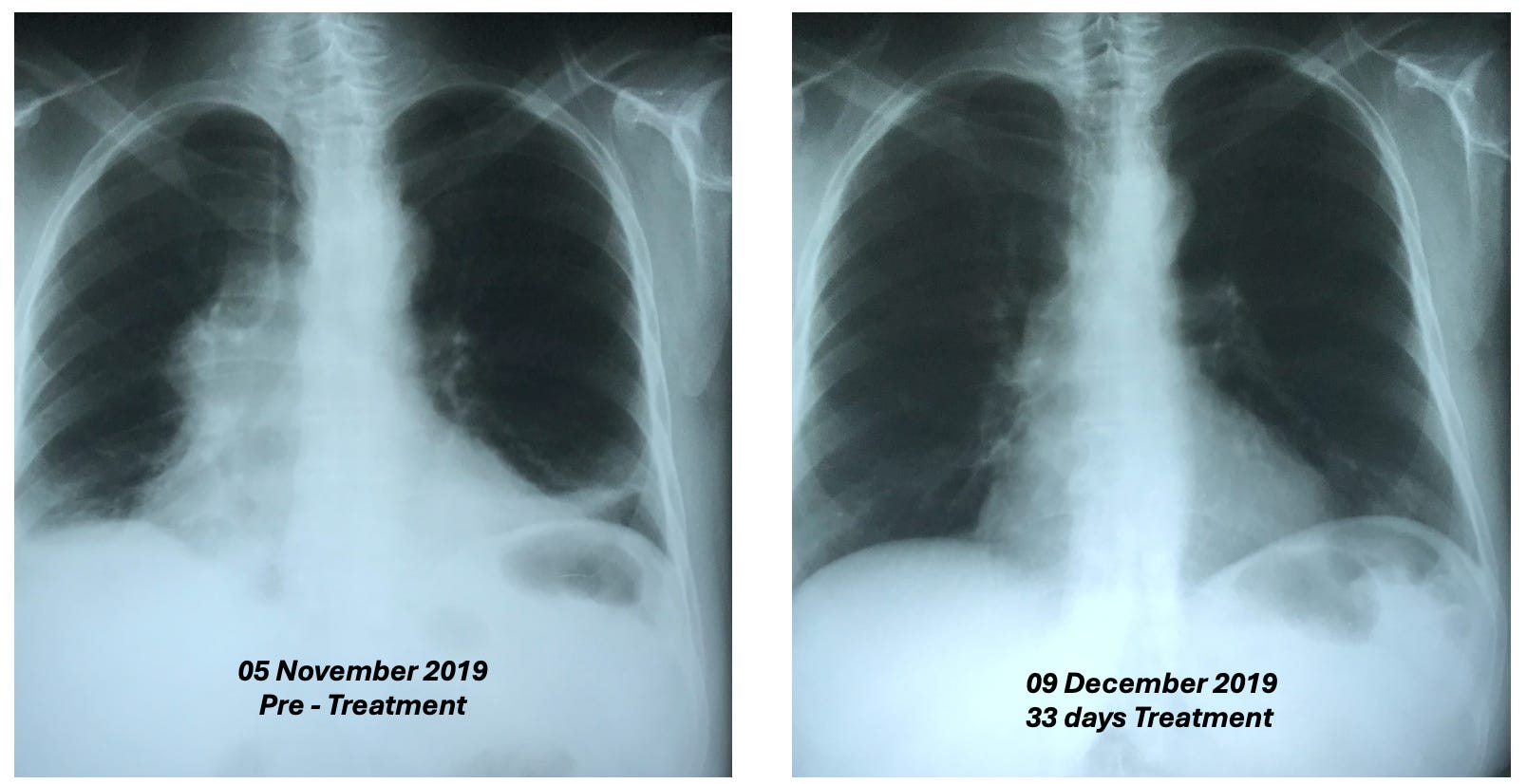

Additionally, this was the CT prior to treatment where the tumor can be seen around the aorta:
While this was the CT two weeks following the D-hematoxylin treatment:
Lastly, at five years follow up, there was no recurrence.
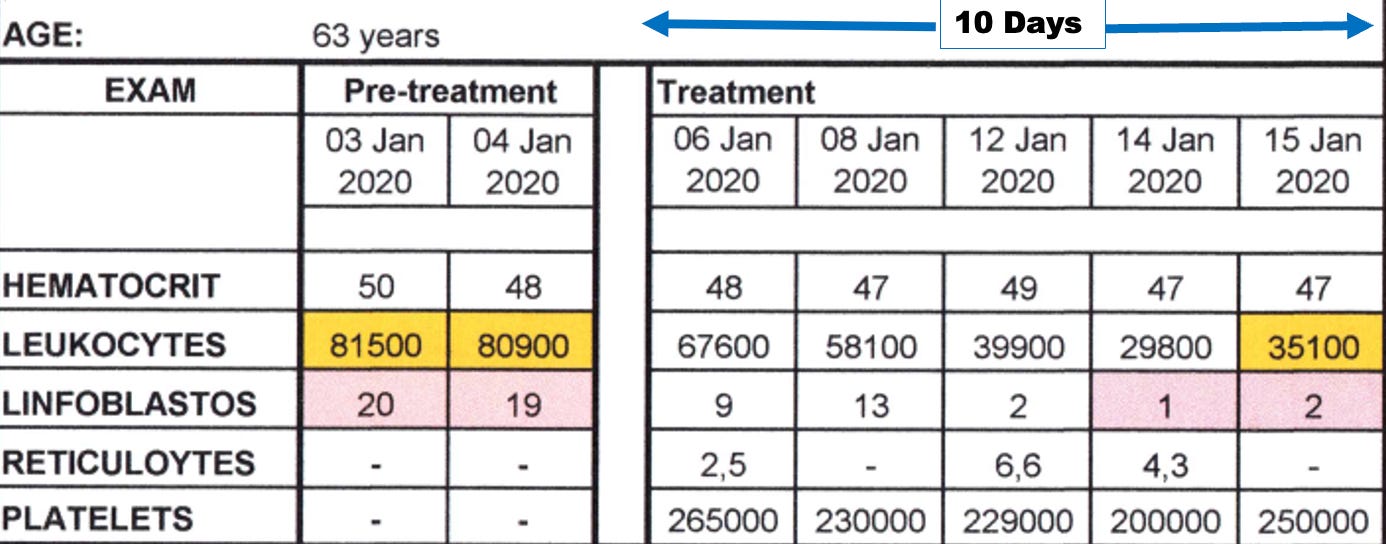
•A 27-year-old female with acute lymphoblastic leukemia reacted poorly to two sessions of chemo, was classified as terminal, and then was started on D-hematoxylin. She had a significant improvement in her cancer and simultaneous improvement in her anemia which continued long after conventional treatments for anemia were halted (which did not include blood transfusions as she was a Jehovah’s Witness).
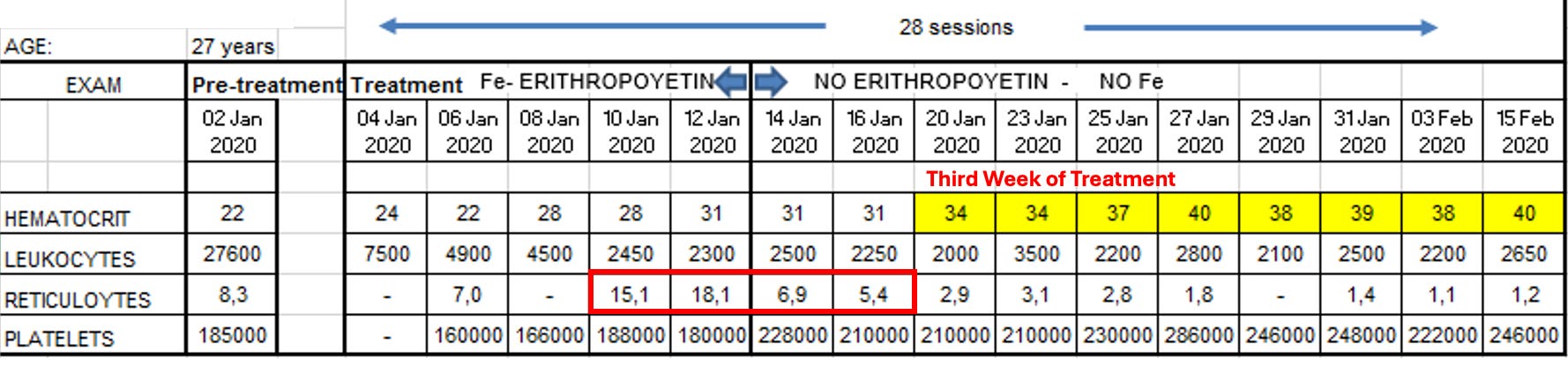
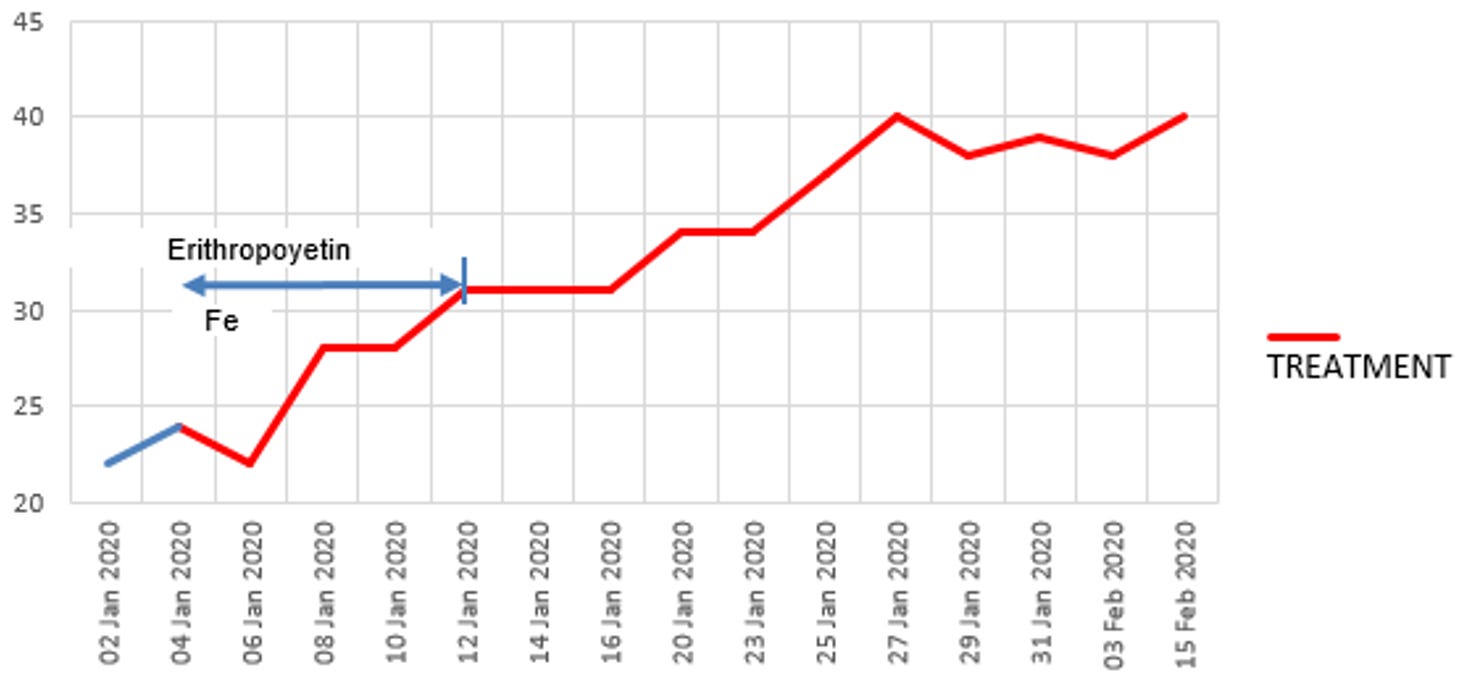
In a before (1-2-2020) and after (2-1-2020) video I saw of this patient, she initially looked very frail and had difficulty walking, while just a month later (after 31 days of treatment), she had no difficulty walking and looked vibrant and robust. Additionally, they continued to monitor her on a monthly basis, and four years later, she’d had a healthy baby, and had her hematocrit range from 42 to 48 (which is slightly above average) indicating she had no further risk of anemia (even though hematologists in the hospital had predicted her reckless pregnancy would cause severe anemia). Additionally, her ESR (which had been significantly elevated prior to treatment) normalized (and remains normal 5 years later).
Lessons from Ecuador
In addition to observing a remarkable degree of success from D-hematoxylin, the Ecuadorian team was able to discern a variety of patterns (many of which mirrored Tucker’s previous observations) that helped craft their treatment protocols. For example:
•While DMSO alone can somewhat help with cancer, the effects of DMSO combined with hematoxylin are completely different from what would be observed with DMSO alone.
•They saw many signs during their treatment protocols that D-hematoxylin selectively targeted cancer cells.
•Cancers did not develop resistance to D-hematoxylin (which is a common challenge with many chemotherapies).
•While some tumors rapidly disappear, other types frequently become avascular (which stops their growth) and dried-out, blanched, or fibrous rather than being directly shrunk (e.g., I reviewed cases where a brain cancer simply stopped growing). In many cases, those tumors are then very easy to extract surgically.
Note: to my knowledge, everyone besides that Ecuadorian team who treats with D-hematoxylin still uses Tucker’s protocol and has not tried to improve upon it.
Variations in D-Hematoxylin Efficacy
On average D-hematoxylin treated 80-90% of the cases where it was used, a figure that resulted from certain scenarios having a much better response to D-hematoxylin. For example, in patients that who are fine three months post-treatment, virtually all have maintained an indefinite remission and there have been no relapses in all patients who’d never received chemotherapy prior to a (complete) course of D-hematoxylin.
Note: patients who have received a full round of chemotherapy prior to D-hematoxylin tend to have the worst response to it.
Additionally:
•Two cancers where D-hematoxylin seems to show great promise are bile duct cancers and leukemias. While osteosarcomas historically have had a good response to D-hematoxylin, the Ecuadorian team has not yet been able to treat any cases of that cancer and hence cannot confirm that.
•Younger patients who were going through life without issue and then suddenly were struck by a cancer (either spontaneously or immediately following another sudden health issue like a traumatic injury) tended to have excellent responses to D-hematoxylin.
•Cancers that have emotional causes tend to be harder to treat and have a poorer response to D-hematoxylin.
Note: similarly, very early on, Merck realized that patients with psychological pain did not respond to DMSO and hence instructed its DMSO investigators not to recruit those patients into the pain studies.
•While hematoxylin can treat the unusual rapid cancers seen in vaccinated individuals, its highest success rate is seen in unvaccinated patients (as in COVID vaccinated patients, cancer remission, for some reason, rather than being permanent, D-hematoxylin stops working once the regular infusions of it are stopped).
•Individuals who receive D-hematoxylin and survive tend to have a stronger desire to live (so this aspect of the treatment process should be encouraged).
Note: This observation mirrors what other doctors have shared with me over the years. I believe is both due to fluid stagnation reducing one’s enthusiasm and desire for life (which is problematic as cancer frequently causes fluid stagnation—but fortunately DMSO often eliminates it) and due to the fact cancer doctors will often pronounce a death date for a cancer patient which ends up being remarkably accurate (a malignant form of hypnotic suggestion which is sometimes referred to as the nocebo effect or medical hexing).
Treatment Evaluation
Since D-hematoxylin is a largely unknown therapy, it is critical for treating physicians to demonstrate its efficacy.
Fortunately, within two weeks, D-hematoxylin consistently drops elevated tumor markers (although this may be preceded by a brief spike). This, in turn, provides a way for both a skeptical patient and physician to see that the treatment is working. As such, the ideal patients for one to first become familiar with D-hematoxylin are cancers with tumor markers that are significantly above the upper range and highly specific to the cancer.
Additionally:
•With leukemias, in lieu of using tumor markers, blood counts can be evaluated on a weekly basis (specifically absolute counts and blastocytes—which, while easy to see under a microscope, can sometimes be difficult to get through standard labs).
•The ESR is also helpful to track (particularly for leukemias).
Note: ESR strongly correlates to zeta potential, a critical parameter that DMSO to some extent improves.
•Similarly, if possible a biopsy should be conducted before and after treatment so that the D-hematoxylin induced changes can be evaluated.
Treatment Protocols
The protocols used by the Ecuador team were based on Tucker’s original one and modified as additional data became available (e.g., on Jim McCann’s advice, EDTA was frequently administered over the course of treatment and observed to improve outcomes).
Note: many remarkable therapies, including many for cancer, were developed in the early-to-mid 1900s as new technologies enabled significant advancements, but the medical industrial complex had not yet dominated medical research. Among these therapies, I found some were effective as claimed, others were exaggerated, some are too rare to evaluate, and many are less effective today, something I attribute to to humanity’s increasing toxicity burden and declining vitality over the last century that I now believe is driven by adverse physiologic changes from certain modern technologies, particularly due to the fluid stagnation they cause in the body which impairs its innate ability to heal. DMSO with hematoxylin stands out because it remains highly effective, is easily accessible (made from two widely available compounds), and I suspect in part owes its success to DMSO and EDTA enhancing fluid circulation (e.g., appropriately dosed EDTA enhances zeta potential).
Some of the Ecuador team’s key discoveries were:
•Once D-hematoxylin’s LD50 was determined to be 1250mg/kg, the investigators realized they could safely raise their initial dose (8-11 mg/kg). After increasing it by 2-3 times, they discovered that an equivalent reduction in total treatment time was observed (e.g., it took 4-5 weeks to cure a patient rather than 3 months).
•The formula they settled on uses a significantly greater amount of DMSO (relative to hematoxylin) than Tucker did. This was in part because it got better results, and because they felt DMSO rather than just being a carrier for hematoxylin, played a major role in the treatment (and unlike hematoxylin could easily have its dose be significantly raised without triggering reactions such as fevers or chills whereas the total amount of hematoxylin must be carefully adjusted to the patient’s system to avoid those reactions). Conversely, while some patients are not comfortable with the chills (necessitating a lower dose and hence longer course of treatment) others can tolerate them and receive higher doses that allow a more rapid elimination of the cancer. Given that these chills occur far below a toxic dose of D-hematoxylin, they serve as an excellent guardrail to ensure the safety of the procedure.
Note: these chills are only observed when D-hematoxylin is given via an IV.
•When D-hematoxylin is given to anemic patients with leukemia, their red blood cell counts will often rapidly improve, suggesting DMSO is either differentiating leukemic cells into ones that can produce red blood cells or providing the space for healthy bone marrow cells to begin producing red blood cells. For this reason (and McCann’s view that supplemental iron was unwise in leukemia), the doctor has explored treating anemia from leukemia with D-hematoxylin and found it works better than iron.
Note: low red and white blood cells are a major issue with chemotherapy as chemotherapy targets rapidly dividing cells, which characterizes cancer cells, and the bone marrow (which rapidly divides to produce your blood cells). D-hematoxylin hence offers a significant benefit over many existing cancer therapies as it not only doesn’t reduce critical blood cells but also reduces the dose of the chemotherapy agents that deplete blood cells, while sometimes also being able to directly increase blood cell counts (e.g., in leukemia).
•While D-hematoxylin is safe, it is important to titrate the dose, as if the dose is too high, patients can experience chills, fevers or shortness of breath. Since the “high” dose varied from patient to patient (or even sometimes for the same patient), the doctor needs to carefully monitor them during treatment and typically the infusion is continued until the patient starts feeling hot or cold. Additionally, hot-cold alternating sensations often occur during the first two sessions, while from the third on, chills are often experienced—all of which can require a doctor to walk the patient and their family through what is occurring so there is no cause for concern (particularly since the chills while harmless can be quite concerning)—which again touches upon how important patients communication is when administering this therapy.
Note: from looking through all of this data, I am relatively sure much higher (and likely even more effective) doses could have been used but were not because they were not willing to risk any possible adverse effects from the therapy (whereas in contrast chemotherapy is routinely given at doses which create significant toxicity and reactions).
Chemotherapy and Radiation
Since cancers are often treated in combination with conventional therapies, they also monitored how D-hematoxylin interacted with them, discovering:
•There were no issues combining D-hematoxylin with radiation therapy.
•Patients who had already been treated with cytotoxic chemotherapies by the time they received D-hematoxylin tended to have a much poorer response to D-hematoxylin. However, if cytotoxic chemotherapy was started at least three weeks after they’d initiated D-hematoxylin, they were much more likely to have a successful cancer treatment.
•In more difficult cases (e.g., D-hematoxylin was started too late and they’d already had significant chemotherapy), like the DMSO-NaHCO₃ studies, D-hematoxylin was not curative but rather significantly decreased their pain and improved their remaining quality of life.
How Does D-Hematoxylin Work?
In the first half of this series, I compiled the extensive volume of literature which elucidated the mechanisms behind many of DMSO’s anticancer properties. However, while compelling, those mechanisms are not sufficient to explain why this mixture is so effective in treating cancer (particularly since D-hematoxylin’s rapid elimination of cancers is not observed with DMSO alone).
Note: when D-hematoxylin is placed into the blood, it will rapidly change color, suggesting hematein (oxidized hematoxylin) is the active agent. Further strengthening this observation, when hematoxylin was sterilized by the Ecuador team through exposing it to ozone (a powerful oxidizing agent), prior to being mixed with DMSO and then infused, D-hematoxylin’s efficacy is not impaired (however exposing powdered hematoxylin to ozone did not evidently change its color so it’s unlikely ozone exposure fully oxidizes it).
Since no definitive mechanism for D-hematoxylin exists, there are a large number of possible explanations for why D-hematoxylin destroys cancer, and presently, my best guess is that for some reason, D-hematoxylin has a high affinity for cancerous DNA and either due to its persistence around the cancerous DNA or it having a specific toxicity to cancerous DNA then destroys it (which in turn eventually eliminating the tumor). However, in many cases, the damage to the nucleus of cancer cells is gradual rather than immediate, so rather than being directly toxic to cancer DNA, once there, D-hematoxylin may initiate some type of process which eventually destroys the cancer’s DNA. Furthermore, while D-hematoxylin will travel to cancers and then eliminate them, it is not effective if put directly into a cancer, which again implies a non-standard form of toxicity is occurring.
That said, I am not sure why that affinity for cancers exists or why D-hematoxylin neither harms normal cells nor even stays in them.
Note: when hematoxylin is bound to a metal salt, it (and hematein) becomes able to bind to and hence stain DNA (which is why most commercial hematoxylin are combined with an often toxic metal). DMSO likely imparts that ability to hematoxylin as well, although it does so through a different mechanism than the mordants (which are simply positively charged metals that bridge negatively charged molecules (e.g., hematein and DNA) together.
Thomas Rogers
After Tucker began having success in human patients, a graduate student, Thomas D. Rogers, saw the importance of figuring that question out and thus decided to conduct his dissertation on the effects of D-hematoxylin on tumors (which can be viewed here and has many pictures of cancers affected by D-hematoxylin).
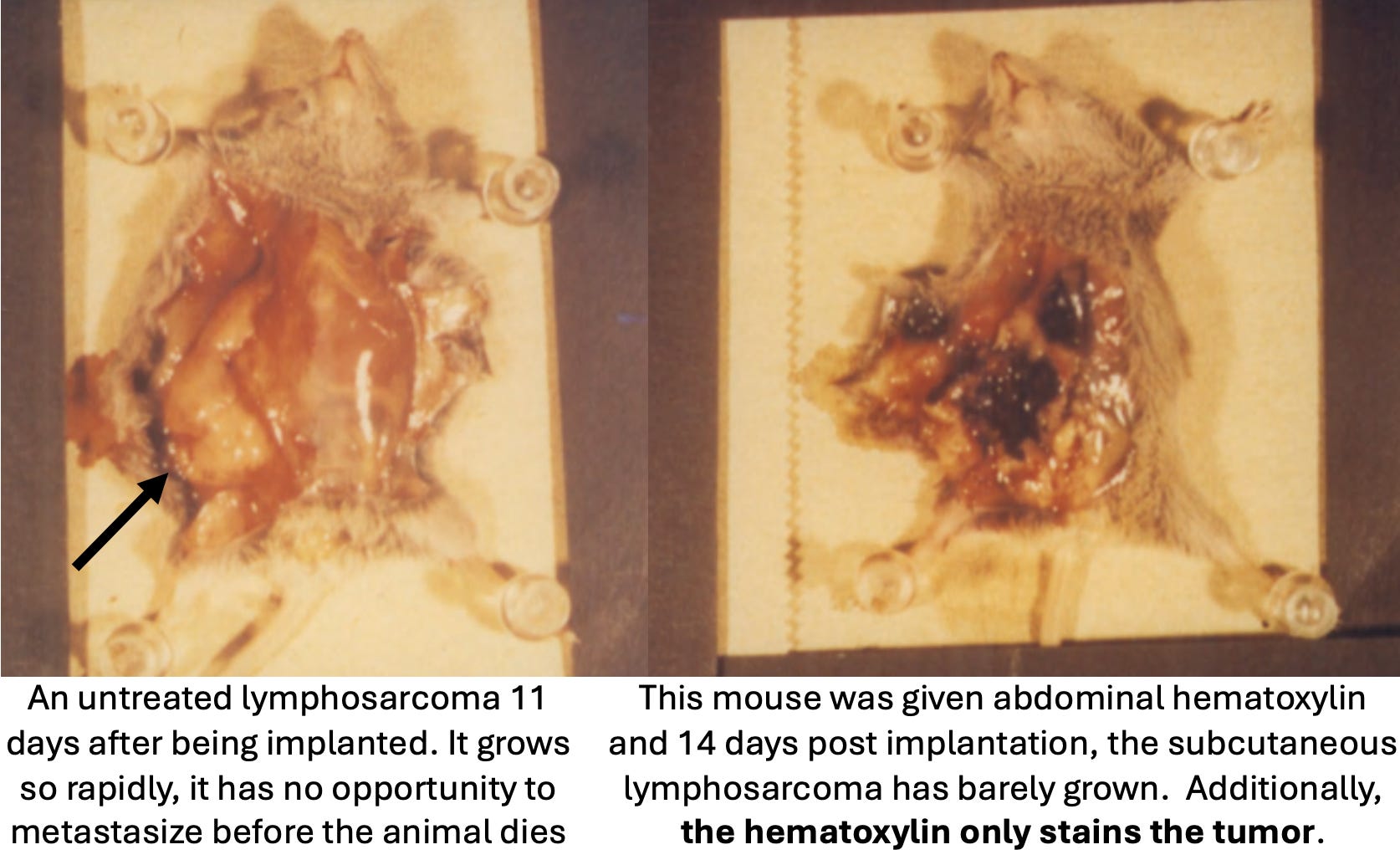
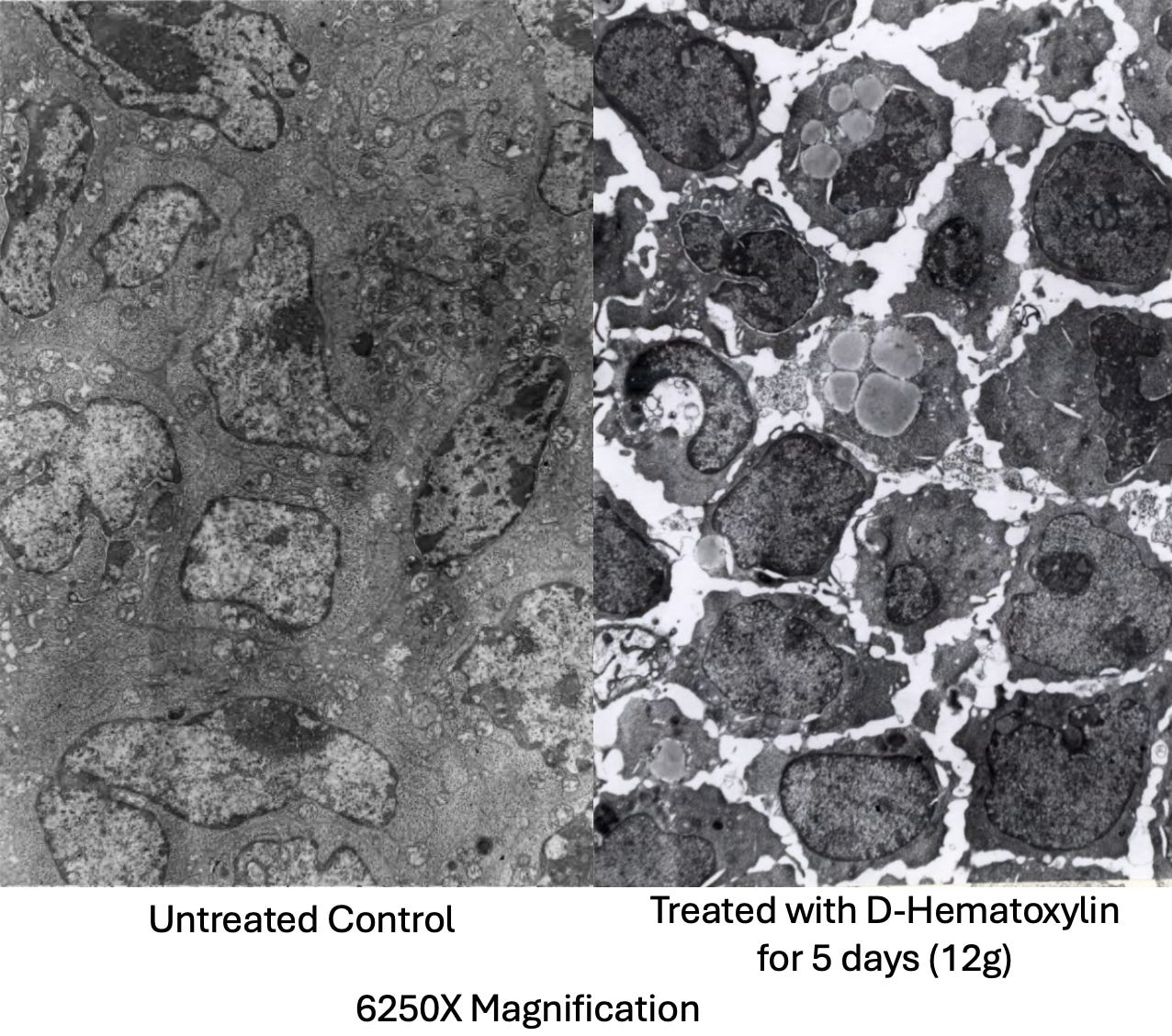
To do so, Rogers implanted mice with rapidly growing lymphosarcoma cells (which typically resulted in death 11 days), then sacrificed and dissected them shortly before their expected time of death and visually examined everything (including under both a light and electron microscope). The mice in turn received either nothing, DMSO alone, hematoxylin alone (which was dissolved in saline through heating and agitation), or varying doses of D-hematoxylin (0.2mL of 90% DMSO mixed with either 2, 5, 8 or 12mg of hematoxylin in DMSO). DMSO and hematoxylin alone were observed to have no side effects, but also do not affect the growing cancers, while D-hematoxylin inhibited the cancers in a dose dependent fashion (and did so without side effects or affecting non-cancerous tissue).
Note: since IVs (which are typically the most potent way to administer DMSO or D-hematoxylin) are challenging to give to mice, Rogers instead administered the treatments through intraperitoneal or subcutaneous injections and oral feeding (and likewise Tapia in his LD50 study only did intraperitoneal injections). There, Rogers discovered that subcutaneous and intraperitoneal D-hematoxylin gave similar notable results, while oral D-hematoxylin produced similar but less extensive results (which dovetails with Tucker’s observation he could also obtain clinical results with oral D-hematoxylin).
With intraperitoneal D-hematoxylin, the lowest 2mg dose caused slight alterations of the tumor cell morphology, 5mg caused the same changed but in a larger area, 8mg sometimes shrank the tumor, while 12mg caused a complete destruction of the tumor and shrank the tumor by approximately 33% (which extended the mice’s lifespan by approximately 27%). Additionally, while the mice were typically sacrificed four days after completing five D-Hematoxylin treatment, in one case they were instead sacrificed a day after, and there, early stages of degeneration were observed, demonstrating D-hematoxylin initiates a therapeutic process that continues long after the treatment has been discontinued.
Additionally, at all doses, D-hematoxylin was found to affect the tumor’s center first, then spread outward, sparing the periphery from the effects observed throughout the rest of the tumor. However, at higher doses (8 or 12 mg), minor changes were also detected in the peripheral regions. This pattern is highly unusual, as chemotherapy agents typically target the cancer from the periphery inward (along with a smaller number that destroy the cancer in a more scattered and heterogeneous manner). This in turn suggests D-hematoxylin is able to penetrate the barriers which normally allow cancer cells to resist chemotherapies (which as I showed previously DMSO has been demonstrated to do for other chemotherapies).
Similarly, when individual cells were observed, the damage initially began in the nucleus (with the appearance of nucleolar lesions and loss of peripheral chromatin nuclei), suggesting D-hematoxylin had an affinity for DNA (which hematein does). Following this, the cancer cells, in successive stages, began to break down and digest themselves (autolysis), a death process different from the apoptosis typically observed when DMSO alone eliminates cancers (that was potentially due to DMSO releasing digestive enzymes from lysosomes). Finally, as this progressed, debris from other tumors increased and white blood cells began to invade the tumors to eliminate them.
Note: in the mice, if cancer debris increased too quickly, it could cause kidney failure (as there was too much for the kidneys to process.
Subsequently, Morton Walker analyzed that dissertation and concluded that D-hematoxylin was dissolving the extracellular matrix (which can also been seen in many other pictures within the study) and that this matrix dissolving deprived the cancer cells of necessary nutrients, causing them to starve (which likewise could explain the gradual degenerative process D-hematoxylin initiates in cancer cells starting from the center rather than the periphery).
Note: other processes could also explain these changes (e.g., anoikis, a form of cell death triggered by detaching from the extracellular matrix rather than starvation, could trigger cell death beginning in the center of the tumor, or alternatively, the loss of the ECM could be an effect of cell death rather than a cause and not play a contributing role to the changes observed).
Sadly, other than Rogers’ dissertation (which just scratches the surface of what was happening), no one has conducted the cellular experiments to determine why D-hematoxylin works. Fortunately, a team in Ecuador (where research is fairly affordable) is presently trying to get the funding to do that research, so if anyone could help support funding that research, please let us know (e.g., in the comments below).
Note: the only other study I have been able to locate that assessed the effects of DMSO combined with hematoxylin was a study that found DMSO effectively washed hematoxylin away from starch granules in pollen cells but not from the nucleus, again implying D-hematoxylin has a special affinity for the nucleus of cells. This study, in turn, was conducted because hematoxylin would consistently darkly stain starch granules, making it impossible to see out the pollen cell’s nucleus.
Protein Kinase CK2
Protein Kinase CK2 , when dysregulated, has been implicated in hundreds of diseases (e.g., viral infections including COVID-19, autoimmune diseases, and neurological conditions). Of those, its best known for playing a key role in cancer (e.g. its activity is often elevated in various cancers, which contributes to tumor progression and poor prognosis). Some of its carcinogenic effects include:
•CK2 phosphorylates hundreds of proteins which allows it to both activate key cancer signaling pathways such as PI3K/Akt, mTORC1, and β-catenin1,2 (which promotes cancer cell proliferation, survival, angiogenesis, invasion, and metastasis).and to inhibit key tumor suppressors like PTEN and p53.
•CK2 modulates the Warburg effect, hence triggering a metabolic switch where cancer cells stop relying on oxygen for energy production (something many over the years believed is a root cause of cancer). Additionally, CK2 also preserves mitochondrial function to support the high energy demands of growing tumor.
•Cancer CK2 activity suppresses the immune system’s ability to eliminate cancer cells, while numerous studies show that inhibiting CK2 activity enhances the immune system’s ability to eliminate cancers.
•CK2 makes cancer cells resistant to programmed cell death and hence makes them continue to proliferate. Additionally, CK2 makes cancer cells resistant to anoikis (which as mentioned above otherwise should be triggered when the ECM around a tumor disappears), suggesting that beyond DMSO removing a cancer cell’s resistance to hematein, hematein might remove a cancer cell’s resistance to DMSO to eliminating it after DMSO partially dissolves its surrounding ECM.
Note: CK2 also makes cancer cells resistant to many chemotherapies—which as mentioned above, D-hematoxylin does as well.
For these reasons, CK2 inhibitors have shown promise in preclinical and clinical studies for treating cancers, and is FDA approved to treat a few cancers (e.g., bile duct cancer).
Hematein in turn, has been shown to inhibit CK2 with a high degree of selectivity1,2,3 (as a non-competitive allosteric inhibitor) via binding to CK2α, a subunit that is over expressed in many cancers,1,2,3 correlates with a poor prognosis,1,2 and when inhibited causes cancer cells to undergo programmed cell death.1,2
Multiple studies (e.g., this one, this one, and this one) have shown that hematein has anti-tumor effects and can trigger programmed cell death in cancers, and it does so in a manner that has a greater inhibitory effect on cancer cells than normal cells.
Note: CK2 inhibitors have also been shown to increase the sensitivity of cancers to chemotherapy,1,2 something also seen with D-hematoxylin.
In turn, most of the cancers which are highly susceptible to D-hematoxylin are also highly dependent on CK2 (particularly blood cancers1,2—which CK2 inhibitors have repeatedly demonstrated efficacy against1,2,3). However, some of the cancers D-hematoxylin has poorer efficacy against are also highly dependent on CK2. In those instances, one potential explanation for those discrepancies is that the centers of the tumors are harder to reach (e.g., because they are thicker or deep within bone), and as a result (at least at the lower doses which have been used so far), D-hematoxylin is not able to bring the DMSO to the center of those cancers.
Note: inhibiting CK2 could potentially explain the delay in cell death following D-hematoxylin administration, but the cancer death CK2 inhibition causes (apoptosis) is different from what was observed by Rogers (autolysis).
Lastly, since CK2 mediates many other diseases, it is quite possible that D-hematoxylin (or the fevers it induces) could cure other diseases, but to my knowledge, neither hematein (or D-hematoxylin) has never been tested on a non-cancerous condition.
Other Mechanisms
Having extensively pondered the available data (all of which you now have access to), I believe we have somewhat of an idea of what D-hematoxylin does to cancer cells. However, other than D-hematoxylin being able to reach the cancers and inhibit CK2, we have much less clarity on why those changes occur. What follows are a few other guesses I’ve come up with to explain this (that I do not at all feel confident in). As such, I welcome any other insights you can share that could explain what is occurring. My remaining theories are as follows:
1. One forgotten school of medicine (in the past known as chromotherapy and currently under the umbrella of biophysics) argues that specific frequencies of light exert different effects on the body. There is quite a bit of evidence for this, most of which was compiled through either putting living organisms in different colored rooms or exposing them to specific light frequencies (e.g., red light for the mitochondria) as biology is quite sensitive to specific light frequencies. In turn, I have long wondered if, in addition to externally applying light, if substances which create colors within the body (e.g., dyes) also have to some extent biological effects due to their optical properties.
Note: two key things helped create this hypothesis. First, many parents over the years have observed red and (to some extent yellow) food dyes worsen their child’s ADHD and many of the behavior changes ascribed in color therapy to red (and to a lesser extent yellow) mirror the changes seen in worsening ADHD. Second, a 1972 paper (which helped created the field of biophotonics) observed that two fairly molecules (one of which is a carcinogen and one of which is not) observed that the carcinogenic one would optically distort a specific frequency light which went through it, while the non-carcinogenic one did not, and then later discovered that very faint emissions of that frequency of light were routinely used by the body to communicate with the environment, hence suggesting chemicals which changed light within the body could cause significant biological effects.
Since hematoxylin (or more specifically hematein) is a strong dye, could potentially be creating an anti-cancer frequency of light within the body (which in turn would explain the gradual cell death it selectively creates in cancers). I was thus curious what type of optical properties it had so that they could be compared to the known effects of those frequencies. Unfortunately, when I looked into it, I found out hematoxylin and hematein’s properties greatly change depending on what it is mixed with. No one has ever studied how it behaves when mixed with DMSO (so it’s currently not possible to assess this theory). Likewise, its optical properties can change depending upon the pH (e.g., the more acidic environment in cancer cells). As such, it is my hope that future research will be able to elucidate the optical effects of D-hematoxylin (as it could potentially explain how D-hematoxylin affects a wide range of cancers).
2. Many potential mechanisms exist for the fevers and chills experienced from D-hematoxylin. Of these, the most probable is an immune activation, which in turn is either due to the immune system reacting to dead cancer cells entering the circulation or D-hematoxylin exposing the surface of cancer cells so that their antigens become visible to the immune system and an immune response can be mounted against it. In turn, I can see five potential reasons for why this happens:
•The immune activation is a consequence rather than a cause of D-hematoxylin cancer elimination (as once debris emerge from dead cancer cells, the immune system will be drawn to eliminate them).
•By removing the extracellular matrix (ECM) around cancer cells, it becomes much easier for immune cells to reach the tumors and eliminate them.
Note: removing the ECM increases the immune system’s ability to eliminate cancer cells and has been explored as an approach to treat cancer.
•D-hematoxylin removes the cytoplasmic barrier around cancer cells, exposing hidden antigens to the immune system.
Note: in the first part of this series I showed DMSO alone has been demonstrated to expose cancers to the immune system (which in some cases allows the immune system to eliminate cancers), and to remove a cytoplasmic barrier around cancer cells (which is likely part of the ECM) that protects them from chemotherapies. In turn, it is possible D-hematoxylin for some reason significantly enhances this exposure (by directly destroying the ECM).
•D-hematoxylin exposes tumor antigens (e.g., by damaging the membrane and causing them to leak into the bloodstream), making it easier for the immune system to primed to target them
•Rather than decreasing a cancer’s ability to evade the immune system, D-hematoxylin directly activates the immune system, causing it to then attack cancers (e.g., the energy UVBI applies to the circulation does this, and it’s possible the spectrum of light D-hematein emits does as well).
Note: the fever and chills could also be due to D-hematoxylin doing something which significantly increases the metabolic rate (e.g., via the mitochondria).
3. As mentioned in the first part of this series, many in the alternative cancer field have concluded hard to detect bacteria (resembling mycoplasma) which frequently change their morphology cause many cancers (and likewise many autoimmune disorders). Because of this, I’ve suspected DMSO’s ability to improve these diseases comes from its ability to affect those minute organisms (particularly since smaller bacteria are more susceptible to DMSO).
In turn, since logwood extracts (including from the heartwood which contains hematoxylin) have shown broad spectrum antimicrobial activities,1,2,3,4,5,6,7 including against mycoplasma.1,2 and DMSO enhances the antibacterial activity of antibiotics, this has made me wonder if D-hematoxylin eliminating those bacteria accounts for its anti-cancer properties. On one hand, this could explain how DMSO causes a delayed death in the cancers (as those changes would follow the death of the bacteria). However, I feel this is unlikely as I have not come across any other antibiotic-DMSO combination demonstrate anticancer properties (which may be because those combinations were never tested against cancer) and because most of the changes D-hematoxylin creates directly destroy cancers rather encouraging them to transform back to normal cells (something frequently seen when DMSO alone is used—although it’s possible differentiation does occur within the bone marrow as we do not yet have any data which can assess that).
Note: while hematein has some antibacterial properties, many of these antibacterial properties have been attributed to other compounds present in logwood. This touches upon another important point—since hematoxylin is an extract of everything in logwood, it is entirely possible that something besides hematoxylin is the actual anticancer agent.
4. Given how low DMSO’s toxicity is, I find it quite odd mixing it with hematoxylin dramatically decreases its IV LD50 (to roughly a quarter of what it was), particularly since DMSO IV toxicity arises primarily from osmotic injuries (created by very high concentrations of DMSO) and adding hematoxylin to DMSO would further increase its osmolarity. Presently (assuming that data is correct), I can only think of two explanations for this.
First, hematoxylin has such a low toxicity that it effectively “dilutes” the virtually negligible toxicity of DMSO.
Note: while this is unlikely, it is possible, as the LD50 of hematoxylin exceeded the doses tried and hence could be a very high value.
Second, D-hematoxylin catalyzes a process within cells which both protects cells from death and selectively eliminates cancers. If this is occurring, it is likely either a result of a change it the cytoplasm or cytoskeleton (the evidence for which was discussed in the first half of this series) or it directly increasing mitochondrial function (e.g., by providing a light frequency which increases mitochondrial function, by serving as an oxidative catalyst through its ability to transfer electrons or generate reactive oxidative species—a property of both polyphenols and quinones).
Note: another forgotten cancer therapy (I have some direct experience with and helped conditions besides just cancer) utilized quinone based catalysts to restart oxidative metabolism within the body. While not a quinone, the polyphenol hematein is considered to be a “quinone-like” and shared certain properties with them. Interesting, the few people I knew who used the Koch catalysts all felt very strongly that the user could not concurrently be exposed to solvents (e.g., by pumping gasoline) as this would inactivate the catalysts, and as mentioned above, there was a case in Ecuador of WD40 (which is full of toxic inhalable solvents) preventing D-hematoxylin from treating a case of leukemia almost identical case to one that D-hematoxylin did treat. Conversely however, DMSO itself is a solvent, and it does not interfere with hematoxylin treating cancer, so assuming this is true, D-haematoxylin (due to it being “quinone like” rather than a quinone) is much less sensitive to catalysts.
5. Since hematein can have a high affinity for DNA, there is also a possibility that it is potentiating DMSO’s anticancer properties by bringing it into the nucleus.
Using D-hematoxylin
Writing this DMSO series (which I began last May) has been an exhaustive endeavor that required many personal sacrifices. One of my primary motivations for doing this was because I felt the D-hematoxylin story needed to be told as virtually no one knows about it despite it being one of the most easily available, safe and (likely) effective alternative cancer therapies out there (particularly since it can treat a variety of otherwise very challenging cancers).
My motivation, in turn, for doing all that I could to create a robust and comprehensive case for D-hematoxylin (which first required each of the previous articles I’ve written in this series) was so that:
•D-hematoxylin would have the best chance of seeing the light of day and being rediscovered.
•Enough people would see this series, and someone with direct experience in using D-hematoxylin would contact me.
To my great fortune, that not only happened, but the doctor I connected with shares my conviction that D-hematoxylin must be something for all of humanity rather than being bought, patented, and locked away in a box.
Note: many of the therapies the AMA blacklisted in the mid-1900s were initially offered buyouts, but once the buyout was declined, a massive campaign (assisted by the FDA) was launched against them that eventually mostly erased each one from the public’s memory regardless of how strong the case was for the therapy.
In turn, that doctor has spent the last 15 years researching and refining the therapy, developing modern protocols for its use, and over the last four months, sharing everything he knew on the subject with me.
In the final part of the article I will discuss:
•What we now know about how to use hematoxylin (both for personal home use and at an integrative cancer clinic)
•How D-hematoxylin can be safely prepared for either application (including which cancers or prostate conditions like BPH and prostatitis can be treated D-hematoxylin or DMSO alone, but do not require IV administration and hence can be done at home)
•Which doctors patients can currently go to for DMSO treatments (including D-hematoxylin cancer treatments)
•General protocols for many of the other conditions DMSO treats (along with where to source DMSO).
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.
