The FDA's War Against DMSO and America
The Forgotten History That Led to the FDA Again and Again Keeping the Things We Most Desperately Need Away From Us

Over the last month, I have been diligently working to alert the public to the decades of evidence demonstrating the remarkable therapeutic potential of DMSO. In turn, quite a few of my colleagues have shared patients are now asking them about DMSO, and a few are shifting their practice to focus on it (e.g., Pierre Kory has done so and is already having numerous amazing results).
Likewise, I’ve now received hundreds (often unbelievable) reports of it it being life changing for people (which can be read here), and it now seems there is a temporary supply shortage of DMSO because so many people (and their friends) have been buying the brands I recommended.
For those who have not read the series, thus far I have made the case that:
•DMSO treats many circulatory and neurological disorders (e.g., Reynaud’s and varicose veins) and profoundly transforms the outcomes of some of the most challenging conditions in medicine (e.g., strokes and spinal cord injuries)—to the point millions would have been spared from a life of disability or paralysis had it been adopted (discussed here).
•DMSO is a miraculous therapy for chronic pain, wounds (e.g., burns or surgical incisions), injuries (e.g., sports injuries) and all types of chronic pain (discussed here).
•DMSO is highly effective for treating a variety of challenging autoimmune disorders (discussed here).
•DMSO is highly effective for treating a variety of connective tissue issues such as scars and adhesions, collagen contractures, scleroderma, FOP (discussed here).
•DMSO is able to treat a variety of protein misfolding diseases (e.g., amyloidosis) including genetic disorders (e.g., Down Syndrome) which are classically considered to untreatable (discussed here).
•DMSO is incredibly safe, having only a limited number of known and manageable side effects alongside no risk of toxicity or death (provided it is used appropriately).
•There are thousands of studies that demonstrate both the safety and efficacy of DMSO (making it one of the most researched medical substances in history).
In contrast, most of the previously mentioned diseases have lackluster conventional options available for treating them, many of which are highly toxic, kill tens of thousands of Americans each year and simultaneously cause far more non-fatal injuries. Worse still, many of them simply are “untreatable” and have no option for what can be done with them.
In short, if what I’ve said so far is true, the fact that DMSO has been kept from us is so egregious, it’s understandably hard to believe. It’s specifically for this reason, that despite the fact I knew it could help a lot of people I really wanted to help by broaching this subject sooner, I had to wait until I had built a decent degree of credibility here before I spent hundreds of hours to begin trying to put the case for DMSO together, then once I did so, do so in a very specific order. Nonetheless, I still do not think anyone would have believed me or had the courage to try DMSO had they not just witnessed almost every medical authority in the world collude to suppress safe and widely used drugs (e.g., ivermectin and hydroxycholoroquine) so that dangerous and ineffective (but incredibly lucrative) pharmaceutical products could monopolize the COVID-19 market.
In turn, while I still desperately want to cover DMSO’s utility for a variety of other challenging conditions (e.g., vision loss, tinnitus, cancer, chronic infections, shingles, and a wide range of skin disorders), I feel I first must touch upon another question—why did the FDA keep it from us, and how were they able to do it to something so much of the public and the scientific community demanded they legalize?
In my eyes, this story is critically important to understand because it:
•Helps us to understand the origins of the mentality within the FDA that to this day continues to ruin people’s lives by burying promising therapeutics that compete with the medical industrial complex. Despite my best efforts over the last two years (e.g., with ultraviolet blood irradiation, AIDS treatments, or GHB for insomnia), I’ve still only scratched the surface of this (e.g., what’s been done with cancer is really depressing).
•Provides a window into the remarkable dedication of a group of Americans which illustrates what our scientific apparatus could be capable of doing for us if it was not shackled by politics.
•Provides some context to why this recent statement from RFK Jr. is so, so, important:
Note: a significant portion of the first half of this article is an abridged version of the history detailed within DMSO the Persecuted Drug (internet archive link here)
The Discovery of DMSO
The simple compound dimethyl sulfoxide can be found throughout nature, and is present in many fruits and vegetables. It was first synthesized by Russian chemist Alexander Zaytsev in 1866. It was essentially forgotten until the 1940s, when industrial chemists, looking for more solvents were curious if this waste product from producing paper could be used instead of being thrown away.
Note: this chronology has been compared to how fluoride (an industrial waste product from aluminum and phosphate production) entered the water supply. The critical difference was that disposing of fluoride (due to its toxic and corrosive nature) was a major expense and liability for these industries (e.g., it regularly severely injured workers). As such, the desire to get it into the water supply was done to absolve the industries from their liability (e.g., “How could it have injured a worker if it’s safe enough to put in the drinking water”). Initially, due to its evident toxicity, the government opposed this. Still, due to fluoride being necessary to produce original atomic bombs and destructive leaks of it creating immense damage to the surrounding areas, for national security purposes, the government relented (all of which is detailed here). In contrast, DMSO was simply looked at as a potential source of revenue that was being erroneously thrown away.
In the 1950s, Crown Zellerbach, a large American paper manufacturing company, began producing DMSO and soon became the world's largest producer. Curious if uses existed for DMSO besides being a highly effective solvent, Zellerbach assigned Chemist Robert J. Herschler to research it and other tree derived chemicals. Through a lab accident, he discovered that DMSO mixed with a dye would bring the dye into the skin, and before long verified it could be used to bring antibiotics and antifungals into plants.
Eager to share this discovery in 1961, he connected Stanley Jacob MD, a renowned surgeon with dozens of publications (in hours, he could produce first-rate papers that took others months to write) and professional memberships who taught at Oregon Health Sciences University (located across the river for Herschler). Jacob (whose brief biography can be read here), was searching for ways to preserve organs and had recently learned of DMSO’s ability to function as an anti-freeze agent. After Herschler shared DMSO’s unusual property, Jacob decided to test it by mixing it with iodine, noticed he could taste it, and realized that not only did DMSO bring things into the skin but also spread them throughout the body.
As this delivery method revolutionized pharmacology, Jacob immediately shifted his focus to it, and the next day topically applied it to his lab staff (the 1960s were a different time), many of whom then developed its characteristic odor. As DMSO dried the skin and wet skin often causes burns to become infected, he decided to test it on rats that were burned and saw a potential therapeutic effect, which then inspired Herschler to try it after a subsequent significant chemical burn. Since it gave immediate relief, Herschler then tried it on a sprained ankle in a lab assistant (where it also gave immediate relief) and then for an arthritic thumb (where it also gave immediate relief).
This early data convinced Jacob to put all his focus into DMSO (which was possible since his intellectual capacity allowed him to rapidly produce the high quality lectures required for his actual job). In turn, after many sleepless nights, and many tests on himself, Jacob became certain DMSO would revolutionize medicine. In turn, he began carrying DMSO on him to give to anyone in need (the 1960s were a different time), and quickly had numerous miraculous cures (e.g., headaches, sports injuries, cold sores, sinusitis, crippling rheumatoid arthritis), Simultaneously he also realized making a standardized dose was almost impossible because people’s response to it was so variable and the timing often was critical (e.g., it only prevented adhesions in rats if given before surgery but not after).
Once Jacob had exhausted his personal funds on DMSO (e.g., he often treated people for free) another remarkable serendipity happened—rather than shoot his research down (as physicians at the medical school had predictably already begun complaining about Jacob doing something unorthodox), his dean decided to approve funding for Jacob’s research (which almost any other dean then and particularly now would have rejected).
Note: it’s hard to describe how extraordinary this confluence of events was. Had a single piece come together like it did, we likely would have never heard of DMSO.
The Thalidomide Era
As Herschler now puts it, “If there is such a thing as a Murphy’s law of new drug development, DMSO proves it. Everything that could go wrong did go wrong.”
Discovered in 1952, thalidomide began being marketed in 1957 (initially over the counter) by a German company (Chemie Grünenthal) as a miracle cure for morning sickness, insomnia, colds, and headaches, and before long 14 pharmaceutical companies were selling it in 46 countries under at least 37 trade names. Reports soon emerged of infants born with defects, in 1959 it was observed to cause peripheral neuritis, and at the end of 1961, it was taken off the German market in November and then globally in December after an Australian Obstetrician was able to get a letter published in the Lancet about it causing birth defects (after having unsuccessfully tried to sound the alarm since June of 1961).
Note: during its brief availability in Germany, thalidomide was estimated to have caused over 10,000 birth defects and the deaths of approximately 2,000 children.
Thalidomide’s adoption in America was slower since the initial company Grünenthal approached (GSK’s predecessor) found it lacked any efficacy in their preliminary trials and hence didn’t want to market it. By the time a second company began testing it across America at the end of 1960, concerns existed about thalidomide. This led the FDA reviewer assigned to thalidomide, Frances Oldham Kelsey, to repeatedly stall its approval (despite it already being approved in Canada). As a result, roughly American 20,000 women received it during the extended clinical trials (with many injuries being observed throughout that period by the FDA). Still, it was kept away from the general population (excluding doctors who gave it to their personal circle because the manufacturer had not told them it was still experimental).
Kelsey’s actions resulted in only 17 American birth defects occurring (from the preliminary testing done across America) and earned her a presidential medal from Kennedy on August 7, 1962. More importantly, it got Congress to unanimously pass the 1962 Kefauver–Harris Amendment to address the concerns about the FDA’s inability to block dangerous drugs (Kelsey had instead stalled thalidomide’s approval) by requiring drug manufacturers to prove their drugs were “safe and effective” and accurately disclose each drug’s side effects.
While well intentioned and necessary (e.g., it gave the Secretary of Health and Human Services clear authority to deny the approval of any drug which had not adequately proven its safety), the act also allowed approval to be denied (or for it to be pulled from the market) if:
There is a lack of substantial evidence that the drug will have the effect it purports or is represented to have under the conditions of use prescribed, recommended, or suggested in the proposed labeling thereof.
The term 'substantial evidence' means evidence consisting of adequate and well-controlled investigations, including clinical investigations, by experts qualified by scientific training and experience to evaluate the effectiveness of the drug involved, on the basis of which it could fairly and responsibly be concluded by such experts that the drug will have the effect it purports or is represented to have under the conditions of use prescribed, recommended, or suggested in the labeling or proposed labeling thereof."
All of this led to a few major problems.
First, Kelsey’s actions dramatically increased the prestige of the FDA, both emboldening the agency and simultaneously leading to many other jealous officials wishing to get the recognition she did for stopping the next thalidomide (which DMSO conveniently fit the profile of). Because of this, the pace of new drugs entering the market dramatically slowed, and ever since then, a consistent complaint of Congress has been the FDA blocking medical therapies the public needs.
Secondly, it galvanized the FDA into rapidly establishing its authority and creating numerous divisions to “police” questionable drugs without the organization being structured to effectively or appropriately administer that authority (which led to perpetual mismanagement, chaos, and frequent abuse of that power).
Third, the FDA chose to define “well-controlled” as a double-blind trial (to the point they clung to this specific argument in 1980 when Congress and the Senate grilled them over their decision to stonewall DMSO).
This was a huge issue because:
•I believe it was what enshrined the scientific supremacy of randomized controlled trials (RCTs).
•RCTs are extremely expensive. As such, most can only be done by the pharmaceutical industry, which due to their cost, consistently frames them (presented in favorable ways, ignoring or adjusting harmful data) to protect the company’s investment (which leads to RCTs frequently being highly inaccurate). This in turn, rapidly increased the cost of drug approval, effectively turning drug approval into a pay-to-play type situation (e.g., currently, the cost to bring a new drug to market is estimated to be between 0.98-4.54 billion dollars, which makes it impossible for any unpatentable product ever to get FDA approval).
•RCT fundamentalism is highly misguided as smaller observational unblinded trials will typically yield the same results as large (non-corrupt) RCTs (proven by this 2014 Cochrane Review), especially if the effect of a drug is significant (rather than a tiny one that can only be detected in a large controlled study and hence is likely inconsequential).
•It was impossible to test DMSO in a blinded fashion because it immediately produced a significant benefit everyone (including the patient) could see; it irritated the skin (to some extent this could be worked around), and it had a characteristic odor. Furthermore, since it was absorbed systemically, it could not be tested on only one side of the body (which would then be compared to the other side, that got a placebo). Additionally, the dose of DMSO patients required greatly varied (and hence made it difficult to standardize trials).
Note: somewhat analogously, I’ve had numerous frustrated patients ask me to find them a seed-oil free infant formula. I eventually discovered that the Infant Formula Act of 1980 (which was virtually unanimously passed by Congress in response to more than 100 infants becoming seriously ill from nutritionally inadequate soybean oil-based formulas), due to outdated science from the 1970s (specifically these 1976 AAP recommendations which did not exist in the AAP’s 1967 recommendations), required infant formulas to have at least 2.7% of its calories (300mg per 100 Kcal) comes from linoleic acid (the problematic ingredient in seed oils). Beyond this making it illegal to sell infant formula without them, I and many others believe this is a root cause of the childhood obesity epidemic in America as seed oils impair mitochondrial metabolism and cause you to gain weight (e.g., this systematic review shows infant formulas cause excessive and rapid weight gain).
In short, while it was necessary to give the FDA the power to block dangerous drugs, giving in the ability to block “ineffective” drugs was a huge issue as “ineffective” is immensely subjective and often becomes a completely unreachable standard.
The ABC-TV program "Good Morning America", on February 5, 1981, where David Hartman interviewed Robert Herschler, helps put all of this into context:.
Herschler: ... the toxicity of DMSO is very low. It's not true that it is dangerous. Compared to aspirin, DMSO is a much safer drug. People are killed taking aspirin; no one has ever been killed taking DMSO.
Hartman: If this is the case and you are so sold on it, why has the FDA not approved its use?"
Hershler: In 1964, the FDA complained bitterly about DMSO because it was both a commercial solvent and a drug. They could not control it. Beyond that, we had a meeting with Francis Kelsey of the FDA where she raised her hands and said, 'We simply cannot cope with a product like DMSO. We envision hundreds of applications [NDA's] coming in, and we simply don't have a budget or staff.'
From then on they took a hard line against DMSO . . . There are many controlled studies that prove it is both effective and safe. And the FDA knows it! The FDA has at least 100,000 clinical [patient reports], and if they statistically evaluate them, and they have, and if they try to prove it is not safe and effective, they simply cannot do it. They have been using this gambit of 'double-blind'—being able to use the 'double-blind' as the reason for rejecting it.
Note: I believe one of the strongest proofs that the thalidomide disaster was nothing more than a tool for the FDA was how quickly they abandoned the fundamental foundational principle it had enshrined and which the FDA’s authority originated from (do not give pregnant women experimental medications) during COVID-19—which has sadly created entirely predictable fertility impairments that precisely mirrored what had been done with the HPV vaccines.
The Early Days
Stanley [Jacob] is a generous man who lives only for others. He has not the slightest desire for money. He is the complete genius. He can turn off all his personal troubles and give himself completely to what he feels must be done for others. In this case, DMSO had to be made available to sick and suffering people.
His motive is that simple…He has no hobbies, no sports. He has no time to play. At parties, he'll toy with a drink for a while and then take off. When he comes to dinner, he eats, sits on the davenport, falls asleep, gets up and goes home—or, more often, back to the lab.
As it so happened, Rosenbaum was the initial discoverer of chloroquine’s utility in rheumatology, but since he took the time to do a meticulous double-blind trial to prove it, while he was awaiting publication, another team got a rushed investigation published and all the credit for the discovery. As such, Rosenbaum recognized he could not be too hesitant to promote DMSO. In the summer of 1963, he and Jacob submitted foundational papers on DMSO (which Science, Nature and Surgery rejected as they were understandably skeptical something like DMSO could exist). Then in October 1963, Jacob simply presented it at the prelude to the annual meeting of the American College of Surgeons.
Note: the first investigational new drug application for DMSO was submitted to the FDA on October 25, 1963 and quickly approved.
Simultaneously, as word of DMSO’s remarkable therapeutic potential began to spread through word of mouth, Rosenbaum and Jacob tried to delay it getting into the mainstream press (as the scientific community disdains “charlatans” making claims to the media before the community has been allowed to scrutinize those claims). Unfortunately, due to their initial attempts failing and Crown Zellerbach deciding to publish a joint patent with the University of Oregon on the medical uses of DMSO, a front-page news story was published in Portland on December 10, 1963. A few days later, on December 18, The New York Times published a front-page article by Robert K. Plumb about DMSO "creating a stir in medical circles in Portland, temporarily spiking Crown Zellerback stock from $5.50 a share that day to $60.25 and leading to newspapers around the country continually cover this wonder drug for the next two years.
Jacob then presented his work before the faculty at his medical school, where he was predictably met with widespread hostility by his peers (e.g., some of them yelled out, "Liar!" "Quack!" "Charlatan!"), with a few subsequently requesting for his dean to fire him (who fortunately did not). Eventually, in February of 1964, Jacob got his paper published in a less popular journal (due to a sympathetic editor intervening)—unfortunately (due to the NYT article) was three months too late.
This was followed by a March publication on DMSO and bursitis, thanks to another sympathetic journal editor, and an April publication in the same journal on DMSO and arthritis and gout. Those three publications, in turn, made some of the scientific community open to DMSO, but they further polarized those who resented Jacob bypassing the scientific community with the popular press (despite the fact he never did that).
While many of the early adopters were cautious, others with minimal experience began engaging in “an epidemic of wild, senseless, irrational experimentation on humans,” further unsettling many of Jacob’s colleagues (who did what they could to get the University to renounce it and stop patients from using it). Jacob in turn, began being scorned by his peers and longtime colleagues and went from being one of the most desirable members for many medical societies to one few would accept (and likewise medical schools completely stopped trying to recruit him and research grants that had previously always been approved without effort became quite hard to get).
One particularly illuminating exchange happened with Dr. Dunphy, Jacob’s friend and immediate superior (they had both been prestigious professors at Harvard before moving to Oregon), who attempted to provide a helpful warning to Jacob by saying, “This smacks of Andrew Ivy.”
Andrew Ivy
Andrew Ivy, at the end of World War 2, was the most famous and influential doctor in America (to the point the American Medical Association [AMA] sent him as their representative to Nuremberg, and he co-wrote the Numerberg code). In 1951, he was introduced to Krebiozen, a promising cancer therapy. He became its leading proponent, but as he was testing it, someone who felt the public needed to know about it leaked a sensational press release, which turned the medical community against him. Following this, the AMA (recognizing its value) threatened the inventors to sell the rights to them, and after they didn’t conducted a fabricated study to debunk it in the hopes of bankrupting them and getting ownership of it (which was later proven by examining the actual records of the AMA study and a co-conspirator plus another witness testifying in front of the Illinois legislators about the criminal conspiracy AMA leaders had shared with him).
Note: the AMA used this same playbook against many other promising therapies. For example, here I discussed how the AMA buried ultraviolet blood irradiation as its miraculous results spread through America’s hospitals with a doctored study after the inventor would not sell it to the AMA and here I discussed how the AMA’s original business model that brought the organization to prominence was using its reputations to monopolize the entire medical marketplace by having the press vilify anyone who did not sell out to them.
Ivy continued to collect data (including miraculous results for key politicians), eventually showing in over 4200 patients that Krebiozen had a 50-70% success rate (depending on the metric evaluated). Nonetheless, the AMA (and then the National Cancer Institute) were allowed to continue with impunity. When Ivy applied for approval to use Krebiozen, the FDA stonewalled them and eventually produced spectrographic data asserting Krebiozen was a common worthless metabolite in the body. Before long, it was revealed the FDA had fabricated that data, leading to Senator Paul Douglas telling the Senate on December 6, 1963: "It is a terrible thing that we cannot really trust either the Food and Drug Administration or the National Cancer Institute.”
Nonetheless, the FDA used their newfound authority from the 1962 Kefauver–Harris Amendment on June 7, 1963 to prohibit Krebiozen from being shipped across state lines, leading to many protests in front of the White House, but unfortunately, as they were on the verge of winning over Kennedy, he was assassinated on November 22, 1963 and Johnson could not be persuaded. Unable to get Krebiozen, many of those patients died, and in 1973, Krebiozen was eventually outlawed in Illinois, and not long after (like many of the other alternative cancer treatments of that era), forgotten. Fortunately, William Kronick (a well known television producer) created an impartial program about Krebiozen that documented this forgotten history and the FDA’s gross malfeasance throughout it.
Note: Mike Wallace also interviewed Dr. Ivy in 1957 (but I have not been able to find a copy of this TV program). Krebiozen was also featured in national magazines like Pageant, Argosy, and Inside Story.
In the future, I will write a more detailed account of this story. The key point here is that the FDA director was just as nasty to DMSO as he was to Krebiozen and that no amount of political influence could stop the AMA’s monopolistic juggernaut (e.g., beyond his personal prestige, Ivy had miraculous results for US Senators with cancer and a Senator who fought for Krebiozen but they were all essentially unable to do anything).
DMSO Gets Caught in the Crossfire
By 1964, Jacob had discovered DMSO treated a myriad of challenging conditions (e.g., poor vision, baldness, many infections, gangrene, disc issues, diseases of the digestive tract from glossitis to hemorrhoids, skin issues, psoriasis of the scalp to athlete's foot and a variety of internal organ disorders).
On March 18, 1964, he and DMSO’s stakeholders attended a meeting at the FDA, where Frances O. Kelsey told them they wanted to do everything possible to permit further testing of DMSO, but simultaneously were worried about being overwhelmed by a large number of DMSO drug applications (particularly since DMSO could be combined with so many other drugs). Yet, once they provided animal data showing animals had no side effects from large doses and that humans had had no side effects from prolonged courses of small doses, the FDA still said the human doses must stop because there was insufficient animal data to warrant them and suggested a month-long dog study before applying for a permit to restart human studies.
Note: At the start of 1964 no fewer than 30 different pharmaceutical companies were approaching Zellerbach for a DMSO license, but rather than go with 1 or 2 as advised, Zellerbach went with 6 of the world’s largest companies (Merck, Sharpe and Dohme, E. R. Squibb & Sons, American Home Products, Syntex, Geigy and Schering), leading to a chaotic situation where they all wanted to be the first one to get a product to market and poured millions into it, which created an atmosphere of urgency the FDA had never dealt with before and hence was not comfortable with. Likewise, Rosenbaum had used his personal connections to reach out to numerous pharmaceutical companies and had convinced many of them to make massive investments to bring them to market. Many hence felt that if DMSO had only had a narrow number of uses, it would have almost certainly been approved, but because of how well it worked, the regulatory system simply did not have the ability to handle it.
By spring 1965, the data for the FDA was there (and looked excellent), but due to DMSO having been prematurely released to the press, immense public demand for DMSO was building. For example, in February 1965, Merck had told Jacob they were getting more requests for it than anything else they’d ever developed, and many professional athletes and movie stars were endorsing it (likewise this 1981 Sports Illustrated article discussed how professional athletes around the country were using it). On April 3, 1965, the New York Times published a front-page editorial calling it “the nearest thing to a wonder drug the nineteen-sixties have produced.”
By this point, over 100,000 members of the public were using the unapproved drug (e.g., by buying it from chemical supply sources or getting it from doctors who were giving it to patients outside clinical trials—which the FDA also really did not like.
“We knew the FDA was getting edgy,” Jacob says, “but we also felt the data we were getting from the various drug company investigators were solid enough that DMSO was safe and effective. What we didn’t know was the FDA at this time was more concerned with its regulations than it was with finding out the human benefits of the drug.”
Note: in 1965, Merck, Syntex, and Squibb all felt there was enough data for DMSO to become a prescription drug and submitted new drug applications to the FDA, but were all turned down (as was Gibb Pharmaceutical Company’s 1971 NDA). By 1983, the NDAs tossed aside by the FDA included 1,500 medical studies performed on approximately 120,000 patients with a variety of health problems.
As miraculous results (and attacks from their colleagues) continued to mount, Schering’s director invited Jacob and Rosenbaum to a July 1965 symposium on DMSO in Germany, where unlike America, the 150 European participants were incredibly interested and open-minded about DMSO, which Rosenbaum felt helped to explain why their DMSO research was ahead of America’s despite them having started later.
Research continued to grow throughout America on every aspect of DMSO in both humans, plants and animals (e.g, it was shown to have remarkable utility in treating cancer), and on September 8, 1965, Merck sent its investigators a glowing review of the safety and efficacy DMSO from their data over the last 18 months on 4,000 patients (which I have excerpted parts of throughout this series).
Unfortunately, the next day (September 9th), the Wall Street Journal published a headline that quickly went across the world:
DMSO MAY HAVE CAUSED DEATH OF WOMAN MAKERS OF WONDER' DRUG WARN DOCTORS
This death occurred in a Squibb research subject (in Ireland) who had continued to take DMSO after suffering allergic reactions and eventually died from anaphylaxis. However, despite it never being conclusively linked to DMSO (she was on many other drugs which could have caused the allergy) or this ever happening again (e.g., I reviewed all known DMSO deaths here), for decades afterward the FDA continued to reference her death.
The pharmaceutical companies immediately warned their investigators to watch out for anaphylaxis, but on September 22, 1965, the FDA terminated Zellerbach’s IND (and ability to conduct human studies) and charged that the number of doctors testing DMSO throughout the country was far greater than the maximum the FDA had permitted.
Note: since DMSO was “safe” investigators would often use it as a last resort in otherwise futile cases where a patient was expected to die—and in the process discovered DMSO has a wide range of uses they could have never conceived of (e.g., feeding a starving infant through the skin who could not receive oral or IV nutrition or saving the limbs of someone with extreme frostbite). Once the FDA put strict restrictions into place over exactly when and where DMSO could be used, this plethora of discoveries from unusual cases ended.
Then in November, due to a few animal reports that high doses of DMSO could alter the refractory index of the eyes (which at worst could make someone need glasses), the FDA summoned representatives from each company testing DMSO to Washington, where Dr. Joseph F. Sadusk, Jr., (the medical director of the FDA) read them a telegram saying DMSO testing was being suspended, after which the FDA immediately sent out telegrams to the WHO and each embassy stating that DMSO could blind its recipients—successfully halting research globally.
Note: this ban was lifted for small numbers of patients with severe illnesses a year later, and then further lifted for a wider range of less severe illnesses (due to a study providing DMSO’s safety), but it was not until September 1979 that the FDA published a regulation abolishing its 1965 regulation banning general research in DMSO. This freeze essentially destroyed almost all the interest in researching DMSO clinically.
As I showed in this article, the FDA’s claim DMSO damaged the eyes was not at all supported by the existing evidence (e.g., at the time of their ban, it hadn’t been seen in any of the 100,000 people who used it—including 37,000 trial participants from Merck, Squibb, and Syntex). Since that time, DMSO has consistently been shown to improve rather than worsen eyesight. Nonetheless, the press immediately parroted the FDA’s line and gratefully thanked the agency for saving us from a thalidomide like disaster which would have caused much of America to go blind (and for decades, FDA officials repeated this concern even when trials designed to detect it all agreed it did not happen).
The investigators were understandably confused since they had no evidence in their research of DMSO affecting the eyes (which many other drugs were known to do) and before long had to start telling all their patients who had come to depend upon DMSO that they could no longer receive it. Doctors like Jacob advised those patients to contact their Congressman, but sadly, the pharmaceutical companies, despite knowing there was no eye risk and having already made a large investment in DMSO, quickly submitted to the FDA’s ban (to the point Jacob was requested to stop telling his patients to complain to the government).
Nonetheless, the patients knew what the FDA had done to them and immense protests began against the FDA (alongside a thriving black market for DMSO being created).
Shortly after (late November) FDA agents began showing up to copy Jacob and Rosembaum’s records, and as time progressed became more hostile and accusatory to them and bold in what they copied (e.g., going to areas they did not have permission to explore, obtaining personal information of patients, or covertly copying his personal correspondences and then refusing to surrender it once they’d been caught obtaining it). After about a month of this illegal activity, they contacted an attorney, who explained to the agents at their next visit that they needed an explanation in writing from their Seattle superior to continue, which led to an interaction quite similar to many others the FDA conducted in the ensuing decades:
Two days later one of the inspectors called from Seattle to complain that Rosenbaum was delaying the work of the FDA. Rosenbaum suggested the inspector talk to his attorney and pointed out that Crown Zellerbach and Merck had duplicate records of his DMSO treatments. A few days later both inspectors again appeared in Rosenbaum's office and gave him a slip of paper threatening to invoke a federal regulation unless he surrendered the records.
"What regulation?" Rosenbaum asked. The inspectors said they didn't know.
That was the last Rosenbaum saw of them
While debating whether or not they should hire at attorney, Rosenbaum was contacted by a disgusted FDA agent who shared that:
Two weeks after DMSO testing was stopped, almost every FDA inspector was called back to Washington for a briefing. It was the biggest call-back of inspectors that ever occurred. The inspectors were told that there was serious question as to whether the FDA had been right in stopping DMSO because of toxicity . They were told to go out in the field and find some "pigeons."
The inspectors were interested in proving that the DMSO investigators had been dishonest. They were also very interested in finding the names of any patients who had had side effects or bad results and who would testify to the damage before congressional committees.
The purpose was to try the original investigators in the press.
There was considerable jockeying within the agency for positions of power and for promotions. Everyone was jealous of Dr. Kelsey, who had received a medal for stopping thalidomide. And everyone was in hopes that they had another thalidomide or Krebiozen story to glorify the FDA and win promotions.
He told me the smartest thing I could do was get myself a lawyer," Rosenbaum said.
Rosenbaum had another visit from the friendly FDA agent. "He told me that FDA inspectors, in the guise of having me sign a permit to examine a chart, had me sign a blank sheet of paper," Rosenbaum told me.
He quoted his informant as saying, "The inspectors are down in the office now, laughing and wondering how to use your signature” and “that the inspectors were copying Jacob's personal correspondence, and he gave Rosenbaum a copy of one personal letter of Jacob's which had nothing whatsoever to do with DMSO, Rosenbaum said.
Following this, their lawyer sent a cease and desist letter to the FDA and a request for the FDA’s unauthorized photocopies to be returned which received a response directed to Jacob rather than his attorney from James Goddard M.D., the recent head of the CDC who’d just become head of the FDA It stated "very few exceptions, the copies of the documents were pertinent to the FDA investigation of DMSO,” that Jacob’s constitutional rights had been honored "with very few exceptions" and that he wanted to meet with Jacob to discuss which of the documents Jacob felt should not have been in the FDA's hands.
As it turned out, Goddard had just been appointed head of the FDA and had zealously prioritized getting Congress to expand the FDA’s police enforcement powers, which was a political challenge since scientists and doctors had not previously been subject to extensive legal scrutiny. As such, the widespread (black market) distribution of an illegal and dangerous substance across America being abetted by reckless scientific investigators was perfect for his agenda.
Goddard served notice that "we are investigating possible criminal violations." This remark was headlined throughout the United States
In turn, he did all he could to cement that narrative about DMSO in front of a house subcommittee meeting on March 9, 1966 with the support of FDA officials like Kelsey. This required significantly distorting the actual information (e.g., they cited the eye issue as a justification for their war against DMSO without mentioning it was a small reversible effect that only showed up in certain animals at over 100 times the human dose and alluded to non-existent reports of it causing visual damage in humans) while simultaneously have Goddard, like any other tyrant, try to sound magnanimous:
"I have, however, permitted continued use for a few investigators to administer to specific patients—about 50 having the conditions scleroderma, tic douloureux, Raynaud's phenomena, and multiple sclerosis," Goddard said.
Note: a few days later at the March 14-16, 1966 DMSO research symposium, one of the FDA’s doctors (Arthur Ruskin) was asked to explain their Congressional testimony DMSO had already damaged the eyes of 24 patients, to which he acknowledged that while there were a few reports of DMSO patients complaining of eye symptoms, no cause and effect relationship had been established.
Remarkably, Sadusk, the FDA scientist who testified to the dangers of DMSO, also complained about the "very extensive publicity appearing in the popular press, representing DMSO to be a wonder drug for the treatment of a variety of diseases." Then a few minutes later didn’t see any issue with glamorizing the FDA using a press release to warn ' 'of the dangers of DMSO.” Soon after he left the FDA and not long after published an editorial in the Annals of Internal Medicine explicitly warning against the dangers of FDA overreach and the FDA controlling how doctors practiced medicine (.e.g., by not letting them use a repurposed drug for another use—something which 54 years later resulted in hundreds of thousands of COVID-19 death). Simultaneously, he ironically also complained about experts and the press exaggerating the dangers of birth control pills (they in fact weren’t; and in reality those pills are infinitely more toxic than DMSO).
The next day, the pharmaceutical representatives of the companies testing DMSO testified before the committee and acquiesced to Goddard’s position. Remarkably, Jacob was not allowed to testify, and simultaneously, the Telegram he sent in defending DMSO was ignored by the committee.
Note: in private heads of pharmaceutical companies shared with J. Harold Brown (an influential doctor) that they had stopped sending DMSO drug applications to the FDA because they were afraid of embarrassing Dr. Goddard and having their other drugs blocked.
In short, Goddard’s ploy worked, and cemented his position as a tough commissioner with the necessary power to keep medical professionals, the drug industry, and the public in line (e.g., by burying Krezbiozen).
A few years later, in January 1968, with a growing disaster having overtaken the nation's introduction of new drugs, the FDA relaxed its rules somewhat, for all drugs but two—LSD and DMSO.
Ten days later, Goddard admonished doctors in a luncheon address at the annual meeting of the American Society of Internal Medicine to practice better medicine and assume their responsibilities ' 'The Food and Drug Administration is a third party in the practice of medicine," he said. He urged his audience to consider the FDA's "recent experience with DMSO."
He was even more hard-boiled with the drug industry and with those who wrote the advertising. He charged industry executives with "excess in advertising," "misleading statements,"an overabundance of information available to the physician," in the industry's free books, periodicals, direct mail letters and other means of reaching the doctors. Some editorial writers charged that Goddard was following the familiar course toward imposing censorship.
And more and more commentators asserted that the role of the FDA, "the third party in medicine," had become that of Big Brother.
Goddard continued to pay his visits to congressional committees, each time with new success . . . and more power.
Goddard in turn, used the public’s fear of hallucinogens to greatly enhance the FDA’s policing powers through convincing the subcommittee that the FDA’s authority should be tied to the recently passed Narcotic Control Act.
"The backbone of our field staff will be composed of criminal investigators," Goddard reported. He said 175 of them—almost all former federal enforcement agents—already had been hired, some as gun toters.
It became evident within the first few months after the FDA had been armed with unprecedented police powers that the agency had scored instant and almost complete success against one "dangerous drug"—DMSO. Most physicians returned their stores of DMSO to the supplier or destroyed them.
To have DMSO on the premises was to court raids by FDA agents and criminal prosecution. To continue to use it in the clinic was to invite malpractice suites as well; complainants could cite the FDA attitude to indicate that the physician was in the wrong.
Note: Goddard’s FDA initiated the practice of no-knock raids that had neither a warning nor a warrant, and over the years courts began to throw out those prosecutions (e.g., this frequently happened with GHB).
The FDA soon began targeting doctors to intimidate the entire profession into compliance. For example, after finding some errors (which were likely inconsequential mistakes) in one DMSO’s researchers records, without letting him present his side of the story, the FDA charged him with falsifying his records, had both him and his co-workers banned from any future research into new drugs (e.g., the FDA sent a letter to 30 pharmaceutical companies advising them to recall all drugs under his investigations), and vilified him in the press.
Note: this tactic worked because the press would treat news leaked from the FDA as having equal value to something that leaked directly from Congress or the Supreme Court. In turn, this was also a key part of how the AMA was able to monopolize American medicine (as the press would consistently attack any competitor the AMA decried as quackery and most recently, it sensationally promoted an innumerable amount of anonymous leaks from “important” government officials who said anything negative about Trump).
Following this, public humiliation, the FDA let that doctor present his case (which showed he was not at fault), apologize, and have the FDA notify the pharmaceutical companies a month later so he could resume researching drugs (although henceforth he stopped receiving the critical NIH grants he had depended upon).
Note: one of the most damaging things Fauci later did was weaponize the grant system against America by cutting anyone who did not support his narratives from public funding and diverting our research dollars to creating new unnecessary pharmaceutical products.
Science Fights Back
Over the summer of 1965, work had been in progress to make a DMSO research symposium, and over the summer Jacob had written to every person in the world who had studied DMSO, and by September had collected 100 abstracts for a research symposium. Following the FDA’s September DMSO crackdown and the cancellation of Zellerbach’s IND (investigational new drug application), they then pressured Zellerbach to pressure Jacob’s medical school to cancel the symposium.
However, two weeks later when Jacob’s dean informed him of this, he made it clear he did not support this violation of academic freedom and asked him to have Rosenbaum be the official organizer so the symposium would not adversely impact the school.
As the New York Academy of Sciences had a reputation for advancing the best science regardless of whose toes it stepped on, Rosenbaum went to them to negotiate a symposium the following spring. The academy was supportive of this idea (they were already fully aware of the DMSO situation), but indicated there would be a significant number of logistical hurdles to pulling it off, which the Academy eventually elected to take responsibility for addressing (e.g., they used their special funds to pay for the costly symposium).
"I wondered about this, and I still do," Rosenbaum said years later. "My guess is that the FDA tried to 'persuade the New York Academy to call off the meeting. The officers were not men who can be intimidated."
Note: Dr. Chauncey Leake, one of the most influential and respected figures in the medical education field agreed to chair the program.
At the same time, Jacob desperately wanted his program to be balanced (something I can sympathize with as I always try to show both sides of an argument fairly), but unfortunately, despite his best efforts, could not find a researcher who held a negative opinion towards DMSO or had obtained concerning data on it.
Not yet aware that the FDA’s goal was to make an example out of DMSO, Jacob also invited Sadusk to send FDA researchers to the symposium so the science could prevail. In turn, on November 9 (the day before Sadusk gave an FDA order banning all DMSO research) Sadusk replied he would be delighted to oblige, "but rumor has it that the symposium never will be held." However, neither DMSO being outlawed nor the other approaches the FDA took were sufficient to stop the Academy.
Leake [the symposium’s chair] then received a call from a drug industry leader whom he chooses not to identify. After the conversation, Leake told Rosenbaum, "My friend asked that we drop plans for the symposium at this time—said it would be very embarrassing to both the drug houses and to the FDA.'
He decided to call Dean Baird [Jacob’s dean]. After hanging up, Leake turned to Rosenbaum. "Know what Baird said? He said, 'Chauncey, when have you or I, as deans and educators, ever let political or economic considerations compromise the search for scientific truth?'
Leake didn't talk about it then. As they got up from the dinner table, he said, "Okay, Ed. Let's give the committee our program.
When Leake announced their decision, the committee applauded. "They seemed to have a special interest in this," Rosenbaum said. "It was as though a tenet of scientific morality had been tried—and triumphed."
The March 14, 15 and 16, 1966, symposium under the auspices of the New York Academy of Sciences was held in a large hall of New York's Waldorf Astoria Hotel. More than a thousand researchers came from all parts of the United States and from overseas. After the FDA had cracked down on DMSO, Jacob had written to every person who had submitted an abstract; he said that now that DMSO had been branded toxic and dangerous by the FDA the paper could be withdrawn. No one canceled.
Note: I quoted this because something like that would never happen now.
The 1966 symposium (detailed here) was a success and a wide range of fascinating research was unveiled, much of which transformed the existing practice of medicine. That symposium in turn was compiled into this summary of the studies presented (which I often reference and I believe should be read by anyone seriously interested in DMSO)
Note: the NY Academy of Science’s willingness to publish this research is also why many of the articles I cite come from their journal. One of the studies presented there (later published in 1975) contained the results of an ambitious project that tested how DMSO enhanced the efficacy of a variety of anticancer drugs. Yet, despite consistently proving successful in animals, human trials were halted right before they started by a jurisdictional dispute within the FDA.
At around the same time [as the symposium], Dr. J. Harold Brown presented a report of a double blind-type study of DMSO before the Washington State Medical Society, in which he told his fellow physicians that as far as he was concerned DMSO was so effective a treatment medium for soft-tissue injuries that he had abandoned what he termed “antedated treatment.” “I have discontinued all analgesics, muscle relaxants, tranquilizers, corticosteroids and physical therapy,” Dr. Brown told the astonished group. “My results with DMSO were dramatic and striking.”
Following this, a third international symposium was held in Vienna on November 8 and 9, attracting 150 scientists from twelve countries and covering data from over 10,000 patients (which Stanley Jacob summarized here). There they keynote opened with:
Rarely has a new drug come so quickly to the judgment of the members of the health professions, with so much verifiable data, from so many parts of the world, both experimentally and clinically, as to safety and efficacy
Fortunately, members of the health professions through- out the world are not all bound by the bureaucratic regulations and judgments of the U.S. Food and Drug Administration.
At this conference, the lack of eye toxicity was again confirmed. Still, it was noted that DMSO at concentrations greater than 30% could injure arteries when injected intravenously. At the same time, many of the benefits other investigators found were corroborated (e.g., pain relief, accelerated healing, the treatment of sports injuries, arthritis and scleroderma). Additionally DMSO had been found to:
•Overcome edema and other effects of trauma.
•Carry the heparin through the skin and into the bloodstream (which is very useful due to heparins effects on zeta potential) and the anticancer drug 5-FU.
•Sharpen tests for kidney and liver function.
•Reduce body water and both sodium and potasssium (90% DMSO, topically, increased urine volume ten-fold).
•With another compound, prevent the calcifying effect of metal salts like lead acetate.
•If given to mice ten days before infection, prevented typhus.
•Make tuberculosis lose its resistance to antibiotics.
•Treat pain associated with blood clots.
•In one study, benefit 77% of patients with rheumatoid arthritis and 84% with osteoarthritis.
•Clear benign skin growths of the eyelids and necks by dissolving the oils which cause them.
Scores of scientists had confirmed the majority of the claims Jacob had made; and some had added new and original claims of therapeutic values. Jacob felt vindicated at the end of the symposium. The distinguished scientists clustered around him, shook his hand, congratulated him for what some called a classical contribution to science and medicine.
Following this, another symposium (where these papers were presented) was again held in New York in January 1974 (and covered by the New York Times) and then again in September 1982 (parts of which can be read here).
Like the previous conferences, all these reported favorable results for DMSO.
Note: I could not obtain a copy of either the Vienna or Berlin conference or one the 1974 New York conferences. If any of you are able to access the information and links I provided, please send me a copy so I can review it and add it to this article.
Following this conference, Germany began quietly returning DMSO to the pharmacies, and other countries also disenchanted with the FDA, followed in legalizing DMSO.
Sadly, as strong and consistent scientific evidence of DMSO’s safety and efficacy had no relevance in the FDA’s decision making process:
As the [1966] New York Academy sessions were drawing to a close, an FDA agent turned to Ann Sullivan of the Portland Oregonian, and said, "DMSO is through."
Ann looked at the man in amazement.' 'Where did you ever get that idea?' Miss Sullivan asked. '
"My boss told me," the agent answered, according to Miss Sullivan
At the symposium, Jacob was notified that Goddard would see him the next day in Washington. He reported the following:
I met with Dr. Goddard at 5:00 p.m. on the 17th of March, 1966. After a few pleasantries I sat down.
Dr. Goddard looked at me sternly and tapped his hand on the desk, saying, "Dr. Jacob, there are two very serious matters I have to discuss with you The first is you violated the hell out of these regulations. We gave you permission to treat a couple of hundred patients, and before that circus was over 50,000 patients were treated. I just don't know what to do about all of these violations. We have never seen anything like it. One of the things that bothers me, however, is that I can't find a motive. We know you didn't make any money from your activities.
Note: because of how fast and efficient Jacob was at working, he was not only able to fulfill his duties as a professor of surgery and coordinate the global DMSO research battle but also by 1972 had given more than 4000 DMSO treatments—including numerous miraculous results I’ve detailed in other parts of this series.
The second serious point is your accusation that my inspectors went into your personal correspondence files without permission. That isn't the story they told me.
I then related the story of the inspection. His answer was, "That's 180 degrees off the story my inspectors told me.”
I said, "Dr. Goddard, did you look over all the material that was photocopied?'' He said,"Yes, with the exception of 40 or 45 sheets of paper, everything seems relevant." My answer was, "Do you think that there would be anything that was not relevant if I had given them permission?"
Dr. Goddard shook his head and said, "I just don't know what to do about you, Dr. Jacob. Your violations were terrible."
I had the feeling that Dr. Goddard was saying to me, you forget about the correspondence and I'll forget about the violations, although these words were not actually spoken.
Note: From what followed, Pat McGrady determined Goddard had wanted Jacob to submit to the FDA and apologize and was not expecting Jacob to threaten to fight Goddard in court if the science would not be heard. Because of this, he pivoted to finding innumerable ways to harass Jacob.
Goddard’s Vendetta
Following this encounter (and the FDA’s newfound policing powers), there also began being strange noises on the telephones indicating Jacob and Rosenbaum were under surveillance. However, they eventually decided rather than be intimidated and lay low they needed to fight back. Likewise, patients from the around country began writing letters to Congress and the President (or their local news paper editors) protesting the FDA’s actions.
Likewise, Jacob received many letters similar to the comments I’ve received here such as:
I am a victim of arthritis. For many years I had not known what it meant to be free of pain. I experienced that wonderful feeling when I was treated with DMSO and improved greatly in my ability to move about with normal freedom.
I cannot but believe that FDA has usurped power which rightly should be in the hands of medical researchers. It not only deprives victims of disease from blessed relief but it retards the work of dedicated researchers, and our country inevitably will lag behind other countries .
During my career as a medical specialist and medical officer for my country, I have seen many "miracle" drugs—penicillin, streptomycin, para-amino-salicylic acid and isoniazid. Also promazine and chlorpromazine. None of these had the immediate and spectacular results shown by DMSO. Nor did any have the future potential as a solvent and vehicle for other drugs.
My brother Bob was unable to walk and was bedridden when he read about DMSO. He was being treated for hemophilia, but the doctor, not being sure of the drug and its use, would not prescribe it for him. Squibb referred Bob to an orthopedic man. Because Bob couldn't walk, he went to the doctor's office in a wheelchair. After using DMSO daily for three weeks, he was on his feet again and able to go back to work.
Early in 1964 my doctors treated my head with DMSO. The treatments, ten in all, healed the severe head pains which I had endured for more than nine years. Up to this time I had been given many drugs and treatments with no relief at all.
When I think of all the arthritics—including my mother—and when I think of my sitting at the New York Academy of Sciences Conference on DMSO and seeing the vastly successful indications (medical, industrial, agricultural) presented there, I can't believe what has happened to this drug. FDA did not attend that conference to find the truth.
I have wrote the FDA, Dr. J. Goddard, about my case [FOP a terminal and incurable disease] asking them to please release to my doctor some DMSO [as it was only the thing that helped]. Since the ban my ailment has progressed to a much more distressing condition than in 1964, before I started using DMSO. They have made no attempt to try and help my case.
To preserve my life, I was forced to become either an expatriate or a smuggler. Since I could not earn a living abroad, I was compelled to adopt the latter course. It cost me a fortune.
I have been a law-abiding citizen, having been charged with nothing more serious than about six traffic violations during 40 years of driving. Because of the unconstitutional actions of the FDA, I have been forced to violate valid and necessary Federal laws in order to preserve my life. I believe this constitutes a very serious infringement of my constitutional rights, and, as such, is a matter of concern to the ACLU.
I attribute all of my success to DMSO for not having to go through with the amputation of my right leg. For two long years this wonderful drug has been kept away. How many people have lost their limbs during this time? Tying the hands of Dr. Jacob in my estimation is an unforgivable sin. Please, please let DMSO come back to us.
On, October 5 1966, a journalist attempted to solve Jacob’s challenges with the FDA by persuading Oregon’s Congressmen to organize a conference in Washington where both DMSO advocates (numerous respected physician scientists) and opponents (e.g., Goddard, Ruskin and the HHS Secretary’s representative) could debate the issue in front of the press. Unfortunately, the press was not allowed to attend the event, and Goddard aggressively controlled the discussion by discussing DMSO’s supposed toxicity and cutting off Jacob whenever he tried to present evidence of its efficacy by stating he was “biased.” Jacob in turn didn’t challenge Goddard so he could save face.
Jacob gave me this account: "I suggested that some of the differences between the scientific community and the FDA on DMSO could be resolved by the National Academy of Sciences. Dr. Goddard replied that the suggestion was very similar to one advanced by Dr. Andrew Ivy during the Krebiozen matter."
After the event, the press was allowed to meet with Goddard alone, but Jacob was able to briefly talk to them after Goddard left.
Later Pat McGrady (from whom much of this article is sourced) on May 1967 interviewed Goddard for two and a half hours.
Within the first few minutes of our interview, in his impressive presentation, Goddard was inconsistent himself at a time when scientists committing comparable mistakes were wrongly threatened with criminal action and disgrace.
I pointed out that scientists at the New York and Vienna DMSO symposia were almost unanimous in citing the drug's fine therapeutic effects and minimal side effects.
"This is not our information," Goddard said. "I think we hear from different parts of the scientific community and I think this is quite natural. Advocates of a position often tend to go to meetings and present their experiences with a drug.
Goddard reported with a straight face that there was substantial criticism of DMSO at the New York Academy and Vienna symposia. I covered both meetings. His word was hearsay and wrong.
In their interview Goddard also repeatedly discussed the importance of a new study the FDA had discovered which “showed eight out of ten DMSO subjects had developed leukopenia” but could not give specifics of the study (after which after McGrady located the study, he discovered what Goddard said was completely different from what it actually said—and likewise leukopenia, has to my knowledge not been found in any other DMSO study). Following this, Goddard stated that since only 60 humans had been observed for eye toxicity, so it was quite possible DMSO’s eye toxicity hadn’t been caught (when in reality over 600 had been studied for this side effect).
Note: Goddard promised to send McGrady a copy of the FDA’s extensive documentation of DMSO’s toxicity immediately after the meeting but never did.
When asked why they’d frightened investigators around the country to death with their police like tactics Goddard both denied they were “police like,” insisted the FDA was being merciful by blacklisting the scientists rather than taking them to court (which later the FDA began to do) and stated:
Let's put a little of the responsibility on the people who acted in an irresponsible fashion. We had a tough job of taking the action, that's true. But by the same token, those who acted so irresponsibly caused this action to take place.
Goddard also gave a variety of excuses to explain why patients that were in desperate need of DMSO (and had sent many letters to the FDA) were being denied permission by the agency to continue using it on an experimental basis.
Note: the FDA’s ban created numerous compelling cases histories where a seemingly impossible recovery (e.g., from being fully paralyzed) happened while the patient was on DMSO, completely stopped while DMSO was banned, and then resumed when DMSO was restarted a few years later.
One of the most notorious ones happened with the Jack Ames, a wealthy and politically connected banker whose daughter was born with severe neurologic illness that left her with a life of severe disability and anguish nothing helped until he tried DMSO in 1964. Following the ban, regardless of his daughter’s suffering (much of what was heart-wrenching to read), when he tried to get the FDA to allow his daughter to resume DMSO, he kept on being stonewalled for “patient protection” (even after he got numerous Congressmen to plead his case).
The enclosed correspondences I am submitting is a sample of the frustrating experiences I have had with the FDA. It is one thing to administer a law and another to completely, for all practical purposes through evasive replies, ignore an individual with an obvious critical problem.
He charged that FDA officials had dodged his telephone calls. He said that DMSO had proved safe and helpful in his daughter's case, and he blamed the FDA's feeling of "vengeance" toward Jacob for its unavailability for seventeen months.
Yet, when asked if he’d made any mistakes, Goddard simply said that he would have handled the vitamin controversy differently. For context, the FDA had wanted to mandate labels on vitamin bottles saying the National Research Council had determined Americans already got enough vitamins from their diet, when in reality they never had and with the public’s help forced the FDA to retract that regulation.
When asked why they were being so strict with DMSO when at least 80,000 people had already taken it without a single serious side effects being reported:
Goddard: Not so far as is known . Who followed up on the people? Who checked up on them? There has been reported at least one instance of anaphylactic death.
McGrady: The lady in Ireland?
Goddard: Yes
McGrady: She was taking several things. Are you familiar with the circumstances?
Goddard: Yes
McGrady: And you still say that?
Goddard I say there is one case reported. Now look, this is why facts are needed.
Finally, when asked if the agency’s new stringent rules were responsible for the pace of necessary drug approvals slowing to a crawl, Goddard denied it and promised that within six months of receiving an IND for scleroderma, it would be ruled upon and most likely approved…which to this day still has not happened.
Note: Goddard also glossed over the fact the requirements the FDA had put in place for scleroderma studies were unreasonable to the point it was almost impossible to conduct them.
Among the points that struck me as especially noteworthy were Goddard's defense of his police and their methods, his unsmiling reference to the poor, dead "lady in Ireland," his denial of enormous influence over the professions [due to the FDA making public examples out of dissenting physicians], his exculpation of the FDA in the personal and professional reputations it had destroyed, his rape of the—it must be said willing and consenting—press, and his readiness to put the power of the government against aggrieved citizens in costly and time-consuming litigation, his minimizing of the disastrous trend in drug development and his optimistic prediction that things would soon pick up.
Later Grady shares:
Periodically over the years, the FDA has announced that DMSO research will soon resume—or, indeed, that it already is under way. Few centers have the specialists and equipment needed. Consequently, there were very few such studies. When I called this to the attention of FDA officials, they explained, "Well, we can't force doctors to undertake the studies, can we?" Or, "We can't compel pharmaceutical houses to handle DMSO; if they're afraid of a visit from our inspectors, there's nothing we can do about it." Or, always, "We're only enforcing the law."
Finally, since the multitude of animal studies showing DMSO had negligible toxicity and the lack of adverse reports from human volunteers had not persuaded the FDA, a Merck DMSO researcher who’d been forced to stop due to the FDA’s ban set up a plan to conduct a comprehensive human toxicology study that he eventually convinced Squibb to support. Squibb then proposed to conduct the study jointly with the FDA, and eventually after two years, convinced the FDA to permit the study.
Note: during this period, the FDA repeatedly promised to test DMSO “properly” and simultaneously said investigators were finding severe toxic effects from DMSO but refused to ever list what they were.
The study began on October 1967, and involved covering prisoners entire bodies in DMSO gel to give them 3-30 times the normal dose of DMSO for either 14 or 90 days and then continually exposing them to an extensive battery of tests. This study (which I reviewed in detail here) was an unusually comprehensive toxicology evaluation and found DMSO was extremely safe, but nonetheless it did very little to change the FDA’s position on DMSO (leading me to assume they had actually agreed to do it in the hope it would have revealed something harmful with DMSO)—rather it took 13 more years for the FDA to lift their harsh restrictions on testing DMSO.
Note: the absurdity of this entire situation is highlighted by Lyndon Johnson (who was president from 1963-1969) reaching out to Jacob in 1971 for guidance on how he could use DMSO.
Oregon’s legislators likewise tried to address DMSO in both the House and Senate. For example, they got the Library of Congress to reproduce and translate the scientific papers on DMSO that had been produced oversees and many of their attempts to legalize DMSO (alongside harsh criticisms of the FDA’s conduct) can be read here (1967) and here (1968) in the Congressional record (search for DMSO). Some of those remarks included:
Thousands of people in this country are needlessly suffering because of the FDA's arbitrary holdup of clinical testing of DMSO. The holdup is pure futile arrogance on the part of a Government agency.
In thousands of documented cases, suffering has been alleviated, pain reduced, and symptoms have disappeared; but in not one single case had a serious side effect been discovered. Restrictions on its use make companies and doctors alike shrink from even filing an application to test this drug. FDA actions have been so harsh, in fact, that drug companies refuse to make DMSO available in medically acceptable grade. The FDA has been accused of bludgeoning the medical community into submission ... of forcing submission to its orders by blacklisting investigators, threatening scientists with unwarranted court action, conviction by press release and, in general, using questionable methods to control the actions of the medical profession.
Fortunately, Goddard’s actions generated more and more pushback from both the public and medical professionals, and just 28 months after he started, he resigned for “personal reasons,” (or possibly the challenges his presence was creating during an election year), after which he gave a defiant speech defending his actions before fading into obscurity (and much later dying from a hemorrhagic stroke—ironically one of the conditions DMSO is the most valuable for).
Sadly the FDA’s harassment of Jacob did not end with Goddard. For example, after the FDA learned Dr. Jacob had loaned the FDA officer who was overseeing the interstitial cystitis drug application money (that was paid back) to pay for his wife’s cancer care, the FDA accused him of bribery and referred him to the DOJ. After pleading not guilty in 1981, a mistrial occurred due to a deadlocked jury in 1982, a second trial occurred in October. On the fifth day of that trial, he not only was acquitted of all charges, but the DOJ dropped them and apologized to him (but did not refund the hundreds of thousands Jacob had to spend defending himself that put him into bankruptcy).
Still, the prosecutors seemed to be aboveboard. I developed respect for both United States attorneys. I had the feeling that they were going through the motions of prosecution but that they almost wish they hadn’t gotten involved in the case. Their hearts weren’t in it.
Assistant United States Attorney Richard E. Dunne III said that the Justice Department wasn’t after Dr. Jacob as a profiteer because of his early financial connection with Research Industries Corporation, the producer of Rimso-50, but the case was pursued because DMSO could be considered the Laetrile (an anti- cancer drug) of the eighties.
Note: laetrile was another promising cancer therapy (with evidence strongly supporting its use) that the FDA and the NCI nonetheless buried.
The Post-Goddard Era
McGrady then met with Goddard’s successor Herbert Ley Jr. MD on February 14, 1969, who promised to be more fair and less confrontational than Goddard (e.g., no more FDA shakedowns).
When pressed on DMSO’s toxicity, Ley stated he believed the FDA had data on (rare) fatal hypersensitivity reactions that had occurred but could not cite specific instances (when in reality, from millions of people taking DMSO, they hadn’t).
I left the Ley interview, as I had the Goddard interview, perplexed that these high officials seemed so lacking in solid information about the most spectacular and the most controversial drug of our time and, as Congressman Wyatt had expressed it, a "persecuted drug."
Not only did the FDA lack data to support its charge that DMSO was forbiddingly toxic but it was proving amazingly uninformed on the results of laboratory and clinical studies At this time, the proceedings of the New York Academy and the Vienna meetings had been published and many papers were being republished in various journals. There also was a strong surge of scientific reports, mainly from abroad, flatly suggesting that DMSO was indeed a "wonder drug," and one without great toxicity.
Note: December 22 1970, after 7 years of waiting, patent 3549770 (for DMSO) was issued to Jacob, Herschler and their respective organizations for a wide range of uses for DMSO that attorneys involved said it represented the broadest approval ever given to a medical advance by the U.S. Patent Office (along with another one to Herschler for DMSO’s antimicrobial properties). Despite the detail and demonstration of efficacy in this patent, the FDA still refused to approve DMSO.
At this point in time, when FDA officials were asked questions about DMSO, they would typically reference their “white paper” (which ranged from 2,000-10,000 words) or its abridged “fact sheet.” Neither listed an author, or provided any references to verify its claims and was full of overt falsehoods (e.g., “The data disclosed serious toxic signs in some animals, appearing at dose levels which suggested little or no margin of safety in humans”) and misleading statements that implied a toxicity and a lack of efficacy which did not actually exist (nor did the FDA actually state was there). However, because of the paper’s tone and it being the first thing most patients or doctors who asked about DMSO saw, it many highly reluctant to use DMSO. Likewise, many doctors (who had no direct experience with DMSO) became convinced it had to dangerous based on this paper and stated as such to any patient who raised the subject.
Note: around the same time, a doctor and director of The Arthritis Foundation of Western Washington wrote a handout titled: “DMSO ANOTHER MIRACLE' DRUG EVERYONE SHOULD AVOID NOW” which begrudgingly admitted DMSO worked, but claimed that there was some evidence it caused cataracts in animals (which is not accurate).
By late 1968 (even though DMSO was still being sold medically in Europe), DMSO research had largely stagnated globally due to the FDA’s constant stream of white papers warning against it (resulting in a Schering Executive stating:
The expectations we placed in DMSO regarding its use in acute inflammatory conditions of the musculoskeletal system have been fully realized…much to my regret [German] DMSO sales have not come up to my expectations. It may be that DMSO will not regain its original popularity unless completely new fields of application, such as cancer, for example, are opened.
Note: at this time, the number of new drugs brought to the market dramatically declined but industry profits were sustained by selling more and more of the older drugs.
Once Nixon replaced Johnson, Charles C. Edwards became the new FDA commissioner. Edwards soon had a long meeting with Jacob that went in the evening where he conveyed that his hands were tied and he could not take back any of what the FDA had done to DMSO, after which Jacob remarked “You know, Commissioner Edwards is a very good man.”
Note: in 1972, Edwards asked the National Academy of Sciences (which typically sided with the FDA) to review all evidence of DMSO, but after two years, they concluded there was insufficient evidence of DMSO’s safety or efficacy, and that it needed to remain an investigational drug until “well controlled trials” were completed.
At this point (as best as I can gather) the FDA became a bit less stringent on DMSO use and permitted its use in laboratory research which was done without the intent to treat an illness (e.g., to preserve cells).
Note: many researchers I’ve spoken told me they were trained to view DMSO as a deadly solvent they could never touch, but none of us could figure out when this started (e.g., it has to be extremely safe if cells can survive and be preserved in high concentrations of it). As best as I can gather, this was likely originated from the mixed messaging from the FDA at this time about DMSO (or may have been done to prevent lab accidents where DMSO caused lab workers to absorb another toxic chemical through their skin). In turn, some PhD’s I know told me started using DMSO due the safety they observed with cells in the lab while others (who don’t know many DMSO containing pharmaceutical products already exist) are convinced anyone who tells people to use DMSO is a murderer.
Simultaneously, DMSO (which was approved for veterinary use and easily available for industrial uses) began being widely bootlegged and sold throughout the country. For example, in the 1970s, numerous gas stations in the Midwest would have signs advertising “we sell DMSO” without making any medical claims.
At the same time this was happening, immense public criticism was building towards the FDA both for their inability to perform crucial regulatory steps (e.g., taking something bad off the market) and them simultaneously taking things away American’s wanted. This in turn led to numerous committees investigating the FDA (which went far beyond Commissioner Lay’s Kinslow report) and and key officials like Lay being kicked out in 1969, all of which were encapsulated a series of scathing articles that were published in the New York Times in 1977 (e.g., this, this, this and this one), which included passages such as:
But the agency, a bureaucratic waif that is responsible for overseeing a staggering $200 billion worth of products yearly, is not only whipsawed by the public controversy, it is so demoralized that a number of its top positions long go unfilled, so burdened that it cannot keep up with the explosion of consumer goods and so battered by lawsuits and outside pressures that its power to make its decisions stick is sometimes undermined.
Its bureaucratic problems have been so vexing that in just the last three years the agency has been the target of more than 100 Congressional investigations, 50 highly critical reports by the General Accounting Office and a series of internal inquiries despairing of ever setting the place right.
“The Congressional hearings in the last couple of years just about destroyed the agency,” an agency official said privately. “The staff has been torn by dissension and strife, the morale is bad, there's no direction and stagnation has set in.”
Indeed, after his departure as Commissioner of the agency in 1969, Dr. Herbert E. Ley said that “what the F.D.A. is doing and what the public thinks it's doing are as different as night and day.” He complained further that during his 18‐month tenure he had been under “constant, tremendous, sometimes unmerciful pressure” from drug industry officials.
As problems arise the agency becomes embroiled in thousands of cases, some of which develop into national controversies, and at times it seems that the agency lurches from crisis to crisis.
A year ago the Ford Administration was on the verge of releasing an economic‐report containing scathing criticism of the agency's utility and effectiveness. The comments were later deleted for unexplained reasons.
Key administrative positions at the agency have sometimes gone unfilled for years and as a result various departments have been allowed to drift and founder through lack of leadership and authority.
Groups of dissident employees have trooped to Capitol Hill to testify against their superiors, plunging the agency into name‐calling internal squabbles that remain unresolved.
The internal complaints have also concerned lower level employees, with some agency officials privately describing members of the F.D.A.'s professional staff as “retreads” and “has beens.” In testimony a year ago dealing with low morale at the agency, Dr. J. Richard Crout, director of the Bureau of Drugs, said this about the chaos in which he had found the agency:
“There was an enormous documents room . . . where some people said fights went on and there was absenteeism. There was open drunkenness by several employees, which went on for months. There was intimidation internally. I tell you that in my first year at F.D.A., even lasting longer than that, 1972‐73, going to certain kinds of meetings was an extraordinarily peculiar kind of exercise.
“People—I'm talking about division directors and their staffs—would engage in a kind of behavior that invited insubordination. People tittering in corners, throwing spitballs—I'm describing physicians. People who would, let me say, slouch down in a chair, not respond to questions, moan and groan with sweeping gestures, a kind of behavior I have not seen in any other institution as a grown man.”
In summing up hearings of the two subcommittees, Senator Kennedy said last summer: “During the past two years these subcommittees have received testimony from 30 F.D.A. employees about the practices and internal management of the agency.
“These accounts included serious allegations of undue industry influence, improper transfers, details or removals, alteration of files and forced withdrawal of memoranda, bias toward drug approvals, improper manipulative use of advisory committees, disappearance of critical agency action memoranda into what the F.D.A. Commissioner termed ‘a mysterious bottomless pit,’ and incredibly slow moving ineffective enforcement and compliance programs with years elapsing between the discovery of a problem and the initiation of a solution, and inappropriate use of medical officer recommendations.”
Such disputes wear and divide further an agency that in recent years has been accused in lawsuits of incompetence or wrongdoing, has been investigated more than 100 times by Congressional panels and has had its intent challenged by liberals and conservatives. All the while, new products continue to be spewed out by the score, while the agency says it cannot monitor those already on the market.
The 766‐page report of the group, headed by Norman Dorsen, a professor at the New York University Law Center, cited detailed cases of harassment of staff by F.D.A. officials, insubordinate behavior by professional staff and inordinate delays in making recommendations on the quality of new drugs.
Fortunately, at the same time the FDA was under intense scrutiny, DMSO’s advocates were able to continue making progress getting it to America.
DMSO in the 1970s
•In the early 1970s, Neurosurgery centers across America were desperately seeking new treatments for the rising incidents of head trauma (e.g., from falls or car accidents since seat belts were not in common use yet) and more than a dozen head injury centers were being funded by the NIH to find a cure. Since those deaths typically occurred afterward due to brain swelling and there was no good way to lower intracranial pressure, Dr. Jack de la Torre at the University of Chicago proposed trying DMSO in 1971.
However, that March morning, only one thing was on my mind. Will the animal survive a severe brain trauma when given a new drug that had never been tested for that purpose? The odds were not good. We had already tested, as part of being one of seven Head Injury Centers in the U.S., dozens of worthless treatments reputed to benefit this usually lethal injury.
And, we would keep on searching when…on that morning, “looky, looky, look at that…!!” my technician’s eyes rolled off the animal as I finished my intravenous administration of the drug. She pointed excitedly to the monitoring charts. The charts were going crazy, instead of cardiac collapse, respiratory arrest, a flat EEG and sure death, the heart rhythm stabilized, breathing returned, at first in gigantic gasps, then in steady, normal, breathing pattern. The electroencephalogram, monitoring brain cell activity, returned in full force and blood flow to the brain, which had ceased in the final stages of the injury, began flowing again and reviving the almost dead brain.It was, as if the hand of God had somehow touched the animal’s forehead. ‘I don’t believe it’, I stammered. But it was true. I felt a tingling in my spine because this reawakening of a virtually dead animal had all the markings of a medical breakthrough.
The drug was dimethyl sulfoxide or DMSO for short, used years earlier as a pain lotion and anti-inflammatory agent.
What we would discover and publish about dimethyl sulfoxide in the next 8 years at the University of Chicago laboratories, would be pharmacological actions of a simple molecule that should have sent shock waves through the field of medical therapeutics as one of the most important drug discoveries of the century in treating devastating brain and spinal cord trauma. Instead, the discovery, the potential for saving lives and the continued research that should have uncovered other uses for dimethyl sulfoxide and similar agents was quietly laid to rest in the coffers of forgotten medicine. It was a baffling paradox that defied a reasonable explanation and to this day still remains unclear to me.
Jack de la Torre then authored over 200 publications and 6 books, spoke at hundreds of conferences and testified to Congress in 1980 about his experiences. As I showed here, if his work had been listened to, millions of people would have been spared a lifetime of disability (or death) from strokes, spinal cord injuries, and head injuries.
•As covered here, research in South America demonstrated that DMSO with amino acids could treat Down Syndrome and a variety of other developmental disabilities in children. The incredible potential significance of the results prompted the FDA to send a delegation, including Stanley Jacob, and a physician from the NIH and Frederick Grigsby MD, an acting director at the FDA. Dr. Grigsby concluded remarkable improvements had definitely occurred and authored a 1972 report urging preclinical studies be conducted to investigate this potential medical breakthrough. Eventually, his report was referred to the National Institute of Child Health and Human Development Mental Retardation Research Committee, and during their August 4, 1977 meeting, they voted unanimously to begin funding those studies. Unfortunately, months later another committee somewhere in the government’s health bureaucracy vetoed the first committee. As a result nothing was ever done to investigate this, despite the lead investigator from Chile (who cared deeply about helping these children) doing everything he could to assist the NIH in conducting those studies.
•Public outcry over the FDA’s actions eventually prompted state legislatures to begin bypassing the FDA and legalizing DMSO in their state (e.g., Florida did this in 1977, and Oregon in 1979), which in turn led to many patients from across the nation flocking to these states for DMSO.
Note: I was unable to locate the Oregon law (or the Nevada or Oklahoma ones), but I found the Florida law, a Louisiana law, a Montana law, a Texas law, and a Washington law that all protected the right of doctors in their state to prescribe DMSO (but not necessarily to publicly advertise that they did that). Additionally, legislators in other states (e.g., Connecticut) tried to legalize DMSO but were not able to get the laws passed. Likewise, at least 6 (unsuccessful) resolutions were introduced to Congress to legalize DMSO.
•In 1978, DMSO was approved for interstitial cystitis (painful bladder inflammation)—which to this day is the only thing it is FDA approved for. This approval was quite unusual, as a nice FDA committee was assigned to it and DMSO was not subject to the impossible standards it had been held to in other trials (instead a trial was composed of patients with chronic interstitial cystitis who had failed all other forms of treatment and their subsequent improvement on DMSO was deemed satisfactory to demonstrate efficacy).
Tragically, after the approval, it was discovered that the trial was poorly conducted (e.g., necessary records were missing, there was never IRB approval for it, informed consent was never obtained). However, after an investigation, the FDA concluded the investigators were careless rather than fraudulent, and the core things necessary for an approval had been done, so the approval was not revoked (as the FDA does not like going back on any decision it’s made). Later when Senator Kennedy discussed that trial at a hearing, he emphasized that there were a series of collective failures amongst several people involved with this NDA—including the FDA medical officer and the drug sponsor’s president (who admitted as such at the hearing).
Because of these embarrassing events, the FDA became even more resistant to DMSO research being conducted, and as such, very little research into new applications of DMSO was conducted henceforth.
•The March 5, 1979, issue of Medical World News reported that at least seven DMSO clinics have opened in Mexico to treat arthritis patients, (e.g., one in Tiajuana in 1979 treated 30,000 Americans who were bussed across the border each day for treatment, and charging $800 for three days of treatment, grossed over 20 million dollars).
Note: one reader shared: “My parents went to Mexico in the early 70s to get DMSO for my grandmother who had debilitating RA. Only thing that brought her relief.”
•In September 1979, the FDA published a regulation abolishing its 1965 regulation which had banned general research in DMSO.
The Tides Shift
Mike Wallace (who had previously covered the Krebiozen on his show that preceded 60 Minutes) put together a segment about DMSO which aired on CBS on March 23, 1980 and again on July 6, 1980.
Note: after that show, well-known Governor George Wallace traveled across the country to find pain relief from DMSO administered by Dr. Stanley Jacob on July 1, 1980, and since it worked, the nation became even more aware of DMSO’s incredible promise. Likewise, over the years many other TV programs (e.g., 2020 and the Donahue show) also hosted Jacob.
Because of how compelling this segment was (and the fact that DMSO could treat a variety of incurable pain conditions many suffered from) it ignited a national firestorm—which was likely deliberate on Wallace’s part as the next day, a Congressional hearing took place to at last address why the FDA was stonewalling DMSO.
Note: after it aired, Jacob’s University had to hire 12 phone operators to deal with the influx of calls. Likewise, over the years many celebrities (e.g., Muhammad Ali) came out to Oregon for Jacob’s care.
That entire hearing is fascinating to read through (as it shows how much remains the same to this day). The key points from it included:
• The roadblocks the FDA had put in place for the scleroderma approval were unconscionable, and the bar had long ago been met with adequate evidence from one of the top scleroderma researchers in the country (who testified).
•The FDA (e.g., Director Crout) kept on repeating the “not-controlled” studies line to justify their blockade on DMSO, while admitting their definition of “well-controlled” (needing a double-blind trial) was a regulation they created, not what the law required.
•That the “well-controlled” argument was absurd with DMSO because if there was a sprain or bruising, you would see DMSO’s effect within minutes and likewise absurd since the FDA had now rejected IND’s supported by 1,300-1,500 studies and over 100,000 patients.
I just wonder how much longer it is going to take before FDA listens to reason—Congressman Don Bonker
•That it was unacceptable the FDA had already dragged out legalizing DMSO for 16 years (especially since some of the representatives there had been working at this that whole time). The FDA of course promised they were treating DMSO fairly and would soon approve it if acceptable evidence was submitted to them—but when confronted with the fact they’d treated the scleroderma and interstitial cystitis applications entirely differently, refused to commit to having a new committee evaluate the scleroderma application.
•Despite not being approved in the US (except recently for interstitial cystitis) DMSO was in many other countries. Those included Canada for scleroderma, China for psoriasis, Great Britain and Ireland for shingles when mixed with idoxuridine, topically for many conditions in Germany, Austria, and Switzerland, through a variety of routes in many parts of South America, and since 1971 in the Soviet Union.
Note: not all of these countries were mentioned in the hearing.
•That many more dangerous drugs remained legal and had never been targeted by the FDA.
•Many compelling cases were presented (e.g., severe spots injuries having miraculous recoveries, fatal head injuries recovering, a child with Down Syndrome whom both her teachers and dentist testified had improved dramatically) along with many of the more typical cases of crippling arthritis or chronic pain experiencing a life changing improvement with DMSO and begging the government to legalize it.
Note: recently a reader who decided to try the DMSO protocol for her two year old Down Syndrome daughter shared a similar story (e.g., in two weeks she became a different child, started to verbalize, started crawling and is getting close to sitting on her own).
•The committee surveyed doctors for professional sport’s team doctors, veterinarians, and rheumatologists, and found a significant portion of each group used DMSO and believed it was safe and effective for human use.
•That there was minimal concern DMSO would be abused and overused because the odor it created made patients only take it when they really needed it.
•That the current design of the FDA encourages them to deny drug applications, that the time involved for new drug approval has risen from 2.5 years to 10 years and that in 1958, one new drug needed 430 pages of submissions while in 1968, a new anesthetic require documentation totaling more than 72,000 pages and 176 volumes.
•The vice president of the Arthritis Foundation stated that (despite having testified against Florida legalizing it) they were open towards DMSO, but it was an “unproven remedy” and that it was important to protect the public from quacks (e.g., they’d aggressively criticized DMSO because it caused patients not to use “proven” remedies). When pressed, he admitted they had not done an independent study of DMSO and also stated they wanted to do everything they could to support that independent study being done. However, if you look at their website (45 years later) nothing has changed on this and that study never got done.
Note: as I illustrated here with the National Multiple Sclerosis Foundation, many “non-profits” for patients with specific diseases are primarily focused on helping pharmaceutical companies produce drugs and in many cases will actively block economical therapies which treat the disease and hence undermine their business model.
Following this hearing, the Inspector General of the Department of Health and Human Services began conducting an investigation into the regulatory procedure DMSO has undergone at the FDA but nothing changed on the FDA’s end.
On July 31 1980, a second hearing was held by the Senate. There many of the same themes were echoed (e.g., the FDA containing to stonewall DMSO, the issues with the FDA claiming there still “wasn’t enough evidence, the need to balance keeping dangerous drugs off the market with allowing important drugs to enter the market and many compelling DMSO testimonials such as those from professional athletes). Because of that, I will only quote Senator Kennedy’s opening statement:
Today, the Senate Health Subcommittee will hear the story of DMSO. It is a sad story, sad because hundreds of thousands of Americans suffering from a variety of painful and often disabling diseases have placed their hopes in this drug, and yet after 18 years we still do not know whether or not those hopes are misplaced. It is a story of failure—failure of the bureaucracy at the Food and Drug Administration to handle the drug appropriately, to expedite a complete and timely review, to detect serious deficiencies in scientific data submitted on the drug's behalf, to satisfy the public that it is doing all it can to develop definitive answers; failure of the private sector to conduct competent and acceptable scientific research on the drug, to adequately monitor the quality of work being done, and to cooperate fully with the FDA investigations of possible wrongdoing. This failure of both Federal and industrial responsibility has had a very high cost: the erosion of public confidence in the ability of government—in this case, the FDA to work, to respond to human suffering, to meet people's needs.
As a result, over 100,000 Americans use DMSO each year. They get it however they can: in some cases legally, in some cases not; in some cases in forms designed for human use, in some cases not. A tiny minority of these people use DMSO for its one legitimately approved purpose, but in most cases they use it for unapproved purposes. Some rub it on their skin; some drink it: some are treated intravenously. By the tens of thousands. Americans are making individual judgments to try DMSO for arthritis, for ankle sprains, for neurological trauma, and for a variety of other reasons. Others are desperate to try it. And many of those who use it believe that they are helped, and tell their friends. and the use of the drug spreads. We will hear some of these case histories this morning, and they are impressive.
•On January 11, 1981 a Florida newspaper report [page 6] discussed a doctor in San Diego stating DMSO saved the lives of 11 people with severe brain injuries who would have otherwise been expected to die.
•On January 15 1981, the New York Times discussed two Johns Hopkins researchers intent on testing DMSO for the treatment of myasthenia gravis because of extremely promising discoveries they’d accidentally made in the lab.
•On February 5, 1981, ABC’s Good Morning America had a segment on DMSO (I have not been able to find a copy of) which where David Hartman interviewed both Robert Herschler and Richard Crout (the Director of the FDA’s Bureau of drugs). In addition to what I quoted earlier in the market, Herschler stated that DMSO was being stonewalled by a "bureaucratic Mickey Mouse" that was hurting America. Crout in turn objected to this and stated:
It's true that there's been quite a bit of initial inquiry—scientific dabbling—certainly a lot of patients have used DMSO.
There's no question about that! But it hasn't gone through the rigorous, disciplined, controlled kind of evaluation that all the drugs do.
I think there are probably two main reasons. One is that it has really not attracted the attention of a number of experts. It's not dramatically effective, and a number of people have recognized that. Secondly, I think the manner of its promotion has tended through the years to scare off the establishment in science. Regrettably! A lot of people who ordinarily would be engaged in drug research and study new drugs simply have neglected DMSO.Those tests are to be done by the promoters or sponsors of the drug. We are in the position of approving the work once it’s done. Carrying the ball on behalf of the drug is what the drug companies ordinarily do. And, indeed, some work is going on for DMSO today that is of high quality. We look forward to having those data in a year or so. I think there won’t be much change in the coming year from what you see now, but the current fad [for bringing DMSO to the people] will wane and a year or two from now we’ll have the data we need.
Then when pressed on if DMSO was dangerous, Crout stated
It's really quite safe when put on the skin. I don't believe I would raise scare tactics about when people put it on and use it for a few days. Anybody who uses it for a month or more in doses of an ounce or more is getting into the unknown. There simply is not much experience with its toxicity there.
•On February 14, 1981, Otis Bowen MD (a popular second term Indiana governor) who “illegally” used topical DMSO to treat his wife’s pain from terminal multiple myeloma and then publicly denounced the FDA’s absurd embargo on it at a national AMA meeting. Remarkably, a few years later, Bowen became Reagan’s Secretary of Health and Human Services, but even then, with this highly ethical doctor at the helm of the HSS, DMSO was unable to overcome the FDA’s prohibition of it.
Note: Bowen was also the country doctor of a reader’s grandmother.
Reagan’s advisors had searched for highly qualified scientists who understood the problems with regulations. But they wanted regulators who were people-conscious first, then regulation-conscious. They didn’t find them. Neither did George Bush. Instead, David Kessler, M.D., J.D., [1990-1997] has turned out to be the most restrictive enforcer of Gestapo-like rules coming out of the FDA.
•On April 27, 1981 an appeals court upheld a 1978 ruling that the FDA’s attempts to stop a doctor from using chelation therapy to treat heart disease (an effective but “off-label” use for EDTA) were not legal as (despite what bureaucrats like Goddard wished) the FDA did not have the statutory authority to determine how doctor’s practice medicine. More recently, the FLCCC was able to prove in court that the FDA exceeded their statutory authority by pressuring doctors to not use ivermectin off-label to treat COVID-19.
•In 1986, the band Dead Kennedy’s made a song about the government’s oppression of D.M.S.O.
•By 1991, over 3,000 clinical studies had been carried out with DMSO involving over 500,000 patients. DMSO has the widest range of therapeutic applications of any single chemical.
•On May 6 1992, 1992 F.D.A. agents, dressed in bulletproof vests, burst into Jonathan Wright’s natural clinic during normal business hours and commanded clinic employees to freeze. The agency said the clinic was raided because it made illegal drugs, including "vitamin-mineral concoctions," that were being injected into patients. A patient caught the incident on video, and that video became a national news story (partially because of how highly regarded Dr. Wright was in the natural medicine field).
Note: I periodically reference Jonathan. Wright’s work here (e.g., for acid reflux) as he was one of the leaders in natural medicine who was responsible for much of what now exists.
These events in turn, created the legislative pressure to pass the Dietary Supplement Health and Education Act of 1994 (DSHEA) which exempted naturally occurring substances from FDA regulations. As DMSO was a natural substance, this effectively ended the FDA’s ability to prohibit the use of DMSO. Sadly, while it is now widely available, most of its uses are entirely forgotten.
Note: in a previous article, I discussed the incredible properties of GHB, a naturally occurring sleep aid that induces restorative sleep that was transformative for many individuals (e.g., with insomnia, chronic fatigue, fibromyalgia, or a general weakening of the body with age) and widely used by body builders (since was both safe and effective for building muscle).
The FDA targeted it with the same police-state tactics they used against Wright (presumably because it was vastly superior to any sleeping pill on the market and thus would have destroyed that billion dollar market), but gradually were shut down by the courts because they did not have the legal authority for those raids. In turn, to get around the restrictions DSHEA put on them, they created a campaign to portray GHB as a date rape drug (despite the fact it didn’t really work for that and there was no evidence of it being used in that way) which the media then amplified into a national hysteria. That in turn, was used to get Congress to pass a law outlawing GHB in America (except for patients with narcolepsy). While abhorrent, this story illustrates how important DSHEA was in preventing the routine abuses committed by the FDA.
Finally, while the FDA still has not approved DMSO (except for 50% DMSO injected directly into the bladder for interstitial cystitis), a variety of pharmaceutical products exist that use DMSO as a “vehicle” or “additive” such as Pennsaid (45% DMSO plus 1.5% diclofenac), a Lupron DMSO implant used for prostate cancer, Onyx (a polymer used to patch ruptured blood vessels) and DMSO preserved umbilical cord blood stem cells.
What Can Be Done?
Based on what happened, I believe the FDA’s war against DMSO went through the following stages:
•It began out of laziness (because they didn’t want to deal with all the drug applications for DMSO).
•It transformed into a state of fear they would lose control over medicine in the United States (since so many people were using it for everything imaginable).
•It was taken advantage of to justify a power grab.
•This significantly escalated by connecting it to the war on drugs in the 1960s.
•Eventually, there was so much inertia behind the policy that by the time reasonable people took over the FDA, they had no power to reverse the precedent previously put in place (as people in the government will never admit they were wrong).
So, while I believe the pharmaceutical industry would not want DMSO to enter widespread use now (as it would cause them to no longer be able to sell many of their unsafe and ineffective drugs like NSAIDs), the pharmaceutical industry wasn’t actually responsible for all of this.
From thinking this over for the last month, I’ve concluded the following (much of which matches many of those who came before me thought):
1. While I disagree entirely with the conduct of the FDA commissioners discussed here (and many others), I feel all of them did want to do the right thing (e.g., Kessler did a variety of very good things while at the FDA and after he left), but for either personality reasons or the sheer challenge of the task they were confronting, they simply did not act appropriately in their position. In turn, I believe their actions highlight why you simply cannot give people too much power as it will always be misused.
2. Getting a good balance between keeping dangerous products off the market and not cutting the public’s access to questionable products they want is a very challenging task—especially if a large lobbyist will immediately vilify that action in the press and get the White House on Congress to pressure the FDA to rescind that action.
Note: the very first FDA commissioner wrote an illuminating book about how despite his best efforts it was impossible for him to protect the public safety by removing dangerous products from the market (e.g., he felt many of the additives in our food were not fit for consumption).
3. Fundamentally, the FDA's task (ensuring all food and drug products on the market are safe and effective) is simply too much for them to do properly. Because of this, a “selective prosecution” type situation is created where the FDA will prioritize its focus on what’s the easiest to do (e.g., attacking natural health products that do not have a large corporation behind them or delegating the responsibility for evaluating drugs entirely to a large pharmaceutical company).
4. The FDA’s justification for existing (and having all its power) is that it protects the public from harmful substances. The fact they could not do that with the mRNA vaccines (or the HPV vaccines) when it was abundantly clear those vaccines were not safe. They should have never been released. Both indicate that the justification for the FDA’s power is gone and that the “selective prosecution” situation it’s been forced into (which prevents it from criticizing products from large corporations) makes it impossible for the FDA to do the core function it exists for.
5. Situations like this illustrate why the recent Chevron defense Supreme Court ruling (which took away Federal Agencies ability to have courts support them interpreting ambiguity in Congressional laws as they saw fit). For example, the FDA’s declaration that a trial for a drug approval must be double-blind to “well controlled” could now be challenged in court, and likewise, many of its other regulatory overreaches could as well (in addition to those that were so egregious courts already overturned them).
In turn, beyond a protracted battle in the courts, I can see four solutions for the FDA’s conduct.
The first is to pray someone with the political support and the will to do it will clean out the agency. I always felt this was impossible, but due to a very unusual confluence of events and many brave people stepping forward to do it, that once in a lifetime opportunity exist.
The second is that the FDA cannot be the sole arbiter of efficacy as there are so many therapies that have decades of strong evidence behind them (e.g., ultraviolet blood irradiation, chloride dioxide or DMSO) that the FDA simply will not look at—while in contrast highly dangerous and totally ineffective drugs frequently get approved (e.g., the recent Alzheimer’s monoclonal antibodies). Rather, some type of parallel approval track needs to be created (e.g., if a petition gets at least 100,000 signatures, physicians can begin a community based trial for a therapy which then is approved by an entity separate from the FDA that must adhere to objective standards for granting that approval). Put differently, as the years have gone by, the FDA has gotten more and more powers, but simultaneously its failing have magnified. In contrast, passing the DSHEA act (which directly reined in the agency’s power) was one of the most useful things Congress has ever done to fix this situation.
The third is that the FDA’s responsibility needs to be shifted to safety, not efficacy as efficacy is simply too subjective (i.e., an effective drug can easily be made to look ineffective while an ineffective one can almost always be made to look “effective”).
The fourth is that the responsibility for monitoring safety has to be shared with the public (and likely competing AI systems which routinely analyze publicly available datasets). One of the key lessons we have gotten from COVID is that the regulators did not have the ability to accurately monitor a relatively small number of COVID-19 related products (e.g., remdesivir or the vaccines) for safety signals, which in turn means they absolutely do not have the ability to accurately monitor the thousands of foods and drugs on the market.
Conclusion
Now the difference between a therapeutic principle and a drug is that a drug is useful in treating a disease or a dozen diseases or even 100 diseases. But a therapeutic principle is an entire new means of treating illness. The basic therapeutic principle of DMSO is that one can treat disease by altering what normally goes into and comes out from cells. Because we are not dealing with a drug in the conventional sense, this is one of the reasons that DMSO is not available today. The people at the FDA, unfortunately, do not understand this concept. I fear that if the situation continues the way it is with people in charge at the FDA and the current division in charge of it, with this group not really understanding this compound, we will not see DMSO available for a fraction of its potential within this century. — Stanley Jacob at the 1980 Congressional Hearing
When I study the history of medicine, I am always struck by the fact many of the most remarkable medical discoveries were found at a time when science and technology was much less advanced than it is now.
This I would argue is in large part due to the fact a very different scientific culture existed in the past; one where people had the freedom to explore unorthodox ideas and those that worked had a real chance to take off.
In contrast, we now exist in a society where anyone who deviates from the established narrative is quickly cut off from their economic livelihood (e.g., dissidents simply cannot get the grants they depend upon for research and doctors will often lose the ability to practice medicine), and like Goddard envisioned, they are all frightened into compliance.
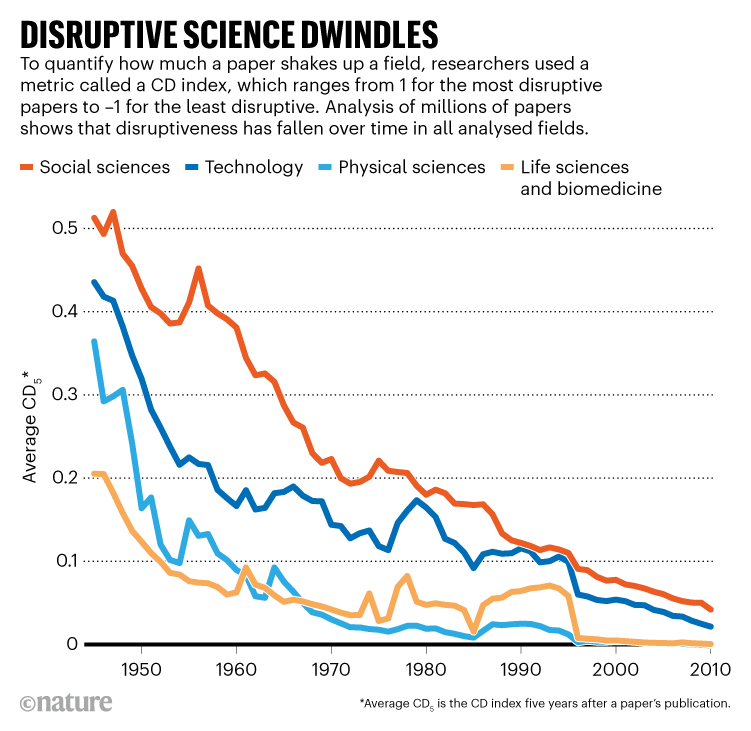
In turn, much of the science we create now isn’t that useful; rather its just small refinements of an existing paradigm (which won’t upset anyone) rather than a new therapeutic (or scientific) principle that radically improves our lives.
Note: famous scientists have said that the discoveries they made which changed the entire world would simply not be possible in today’s research climate—and given how rare paradigm shifting discoveries are now, I am inclined to believe that (e.g., most of the really useful new ideas I come across now arise from observant colleagues discovering them in practice rather than from large research endeavors) .
Similarly, many doctors believe the biggest mistake their profession made was giving their power away to corporate medicine where they are forced to prioritize how their employer wants them to treat their patients over what’s actually it their patient’s best interests (e.g., consider what we saw throughout COVID-19). Here, I would argue that shift actually began with Goddard’s work to whip the entire medical profession into line, and that what we saw throughout the pandemic was simply the next escalation in a multi-generational plan.
I thank you for making it through all of that; this is an important story to be told and it just incredible the pieces came together as they did both then and now. I will be releasing a shorter version of this in the future and will resume covering many of the other uses of DMSO I am sure many of you are quite curious about.
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.
Your conclusion reminded me of an undercurrent that most of us who were born in the 1950s recognize: there is so much less freedom now in so many ways. It is a huge change, and i guess has happened gradually. I think it is partly due to mass programming, and it is why most young people don't even seem to want to be free. Most of them believe the mainstream media via tech or TV. Like my late 30-ish stepson said, masked and vaxxed-up in 2021: I don't make the rules, i just follow them". Chilling. . . . . and Orwellian.
“… and it now seems there is a temporary supply shortage of DMSO because so many people (and their friends) have been buying the brands I recommended.“
I think this amazing occurrence exemplifies the kind of transformative power we can have when we unite around, and amplify, something that is truly beneficial. The ripple effect is enormous.
AMD, God bless you for being a catalyst, and tip of the spear in this journey towards reviving healthcare.
PS- I think the compassionate, level-headed, and non-vitriolic approach that you express via your writings is sorely needed in all areas of resisting the elites. … It saddens me to see how many people are at each other’s throats on social media, especially when it occurs between prominent voices within the resistance. … I truly believe that uniting around the mindset of how we can help empower our fellow human beings is our most potent ticket for defeating the aspiring tyrannical technocrats, as well as for creating a society that restores autonomy to (and empathy between) the people… and I think your Substack embodies exactly that.