

Spiritual Considerations in Medical Ethics and Abortion

In the first part and the second part of the series, I have attempted to make the case that our culture has a concerning deficiency in ethics and morality (henceforth morality will refer to both), and this deficit negatively impacts many areas of our society including the financially driven practice of medicine. Because abortion is such a complex topic that touches on the core of life itself, it provides an excellent perspective for cutting to the essence of the fundamental decisions that guide our lives.
Before I go further, I must emphasize that I do not consider myself to be an expert in this area, and I am simply sharing what I have personally discovered from periodically examining this issue throughout my lifetime. As such, it is very likely I am missing important points from this discussion and that in the next 10 years I will hold a different perspective from the one I held at the time of writing this.
The problem with morality is that to some degree it is always subjective and likewise as the post-modernist movement has shown, almost any viewpoint can be argued for or against. My possibly naïve belief is that one true system of morality does exist, but since I am not omniscient, I will never be able to know for certain what it is; rather the best that I can hope for is to gradually approach that universal truth.
When looking at this subject, it is helpful to recognize two forms of morality that I will term “practical morality” and “universal morality”. Practical morality encompasses a system of rules designed to create the optimal situation for everyone bound by those rules, while universal morality represents the elusive system of divine truth each of us searches for that is in accord with the will of the universe.
Sensitivity and Specificity
In medical school, we quickly learn in soundbites about many complex subjects that are easily books unto themselves. One concept, sensitivity versus specificity, provided one broadens its meaning, appears to be the underlying issue in most of the challenging questions of practical morality.
Sensitivity is defined as the likelihood a test will detect what it is looking for, while specificity refers to the likelihood the test will not have a false positive when attempting to detect something. There is always a give-and-take relationship between these two concepts because as you become more able to detect something, it is more likely that you will spot something that was never there.
For example, with someone who is paranoid and assumes everyone is out to get them, they are much more likely to identify someone who is trying to take advantage of them than another person who is not paying attention to each potential enemy around them. At the same time, a paranoid person will continually accuse individuals who meant them no harm or even wanted to help them of malice and ill intent and be absolutely certain they observed subtle non-verbal signals that proved this ill intent.
Much like a paranoid individual, the PCR tests for Covid have played a pivotal role in creating the “pandemic“ because, through being calibrated to an excessively high number of replication cycles, had a high sensitivity and a low specificity. As a result, the tests gave a large number of false positives that would have never occurred if the test had been calibrated to an appropriate number of replication cycles that created a lower sensitivity and higher specificity.
Within medicine, many medical decisions are made based on sensitivity and specificity (although they are rarely described by this terminology). For example, the reason why a doctor checks your cholesterol and your blood pressure is because if either of those is too high, it may increase your risk of dying over time. However, the risk dramatically varies as different human beings have different ideal cholesterol and blood pressure levels. For example in older adults, their arteries tend to calcify and thus require more pressure to move blood through their system. For these patients, higher blood pressure is thus a necessary physiologic compensation of the body, and commonly when their blood pressure is lowered with medications to bring it into the “ideal range,“ the reduced blood flow to the brain will cause those patients to pass out and seriously injure themselves (this is a very common pharmaceutical injury in the elderly).
Medical conditions also exist where an individual develops a much higher blood pressure and the need to address that blood pressure becomes more definitive. When this is seen in the emergency department, stronger blood pressure medications are immediately injected into the patient to address the perceived risk that the patient may experience a critical or fatal complication from their high blood pressure in the immediate future. Rarer still, in a condition known as malignant hypertension, an even higher blood pressure spike can occur which is almost always accompanied by significant neurological symptoms and if it is not addressed rapidly, is likely to become fatal (almost all patients with malignant hypertension will die within two years if the high blood pressure is not addressed).
The question with blood pressure and many other things then becomes exactly where you make the cut-off and if sensitivity or specificity is more important, something that is supposed to result from a consensus between independent experts following careful deliberation of the issue. In this recent article, I showed that the horrifically bad pandemic response was the result of three career scientific officials lacking basic competency to evaluate scientific evidence or craft basic policy. Had the appropriate procedure been followed (where the pandemic response was created through an international team of independent experts), completely different thresholds for pandemic mitigation measures with appropriate sensitivities and specificities would have been chosen that likely would have saved a lot of lives and not destroyed the economy for the working class.
In modern medicine, there has been a consistent bias to continually lower the cut-off points for sensitivity and specificity, and over the years using blood pressure as an example, the acceptable threshold has been repeatedly lowered. As a result, many individuals who are told they absolutely must take blood pressure medicines or have an immediate risk of dying, fifty years ago would not have even been considered candidates for blood pressure medications.
As you might have guessed, this bias is a result of pharmaceutical corruption within medicine, because as thresholds are lowered, this makes more individuals eligible for drugs and thereby causes more and more to be sold. One of the best examples is statins being recommended for everyone to lower healthy cholesterol levels on the basis of non-existent evidence voted through by committees composed of scientists taking money from statin companies. The continually increasing sensitivity for requiring “preventive” medicines leads to the curious tradition we have now where the majority of the population is on multiple medications, many of which do not benefit the patients and in combination significantly increase the likelihood of death or disability for the patient.
One of the more depressing things in medicine is continually seeing older adults who are on five to ten prescriptions you know are harming them and do not have a good justification for being prescribed. Unfortunately, it is very difficult to stop the patients from taking these medications because none of the involved doctors wish to be responsible for something bad happening as a consequence of a drug being withdrawn (as the legal system is only set up to penalize them for this but not penalize them for a complication to an approved usage of a medication).
Much in the same way the doctors have calibrated their sensitivity and specificity for terminating a drug to prioritize prevent their own personal liability, that same issue can be found in every facet of our society. This is because the tools we use to address each problem (regardless of the problem's scale), will always have imperfect sensitivity or specificity for accomplishing their goal (sensitivity) and not creating collateral damage in the process (specificity).
For example, our legal system has the principle of innocent until proven guilty; this decreases its sensitivity to convicting a dangerous perpetrator and increases its specificity to not wrongfully convict someone. Comparatively, Mexico follows a principle of guilty until proven innocent, which trades an improved sensitivity for a decreased specificity. The sensitivity versus specificity issue is particularly important in regards to the death penalty because it is a horrendous sin to execute an innocent person (which does happen), but if the death penalty has too low of a sensitivity then it no longer serves its purpose to scare criminals out of committing murder.
To use another contemporary example, the Black Lives Matter movement argues that police have too high of a sensitivity for targeting African-American criminal suspects and using deadly force when the officer perceives a threat to their own life. Commentators on the conservative end of the spectrum, citing the Ferguson effect, instead argue the police have too low of a sensitivity for addressing African-American criminal suspects and believe this reduced sensitivity also costs black lives because it fails to prevent the violent crime and homicides that are common in certain African-American neighborhoods.
When you begin to break it down, you can see how the issue of sensitivity versus specificity is wrapped up in nearly every aspect of our lives. For example, when considering a potential romantic partner, there will always be signs they are an amazing fit you do not want to miss the opportunity to become close to, but there will also be warning signs or red flags the partner should be avoided. Depending on one’s life experience (such as previously receiving significant abuse and trauma from a past relationship) the threshold of sensitivity and specificity each human being will use for evaluating a potential romantic prospect will vary immensely and often heavily influence the course of their life.
With the Covid vaccines, aggressively vaccinating the entire population and not allowing exemptions regardless of pre-existing medical conditions significantly increased the perceived sensitivity of this intervention (the theoretical likelihood that cases of Covid would be prevented and lives would be saved) at the expense of decreasing the specificity of this intervention (those individuals who die or suffer debilitating vaccine injuries). Although many evil people have been involved in the entire vaccine roll-out, I believe that the majority of officials who pushed for the vaccines while being fully aware they had potential side effects did so because they referenced fraudulent data that erroneously overestimated the sensitivity of the vaccines and underestimated their specificity, leading to it being justified in the eyes of these administrators to choose a public policy threshold that prioritized sensitivity over specificity.
One of the fundamental reasons why I am such a strong advocate for individual liberty is because regardless of how well-intentioned administrators and bureaucrats are, they will always make “tough” policies based on erroneous data which leads these administrators to overestimate the sensitivity of their approach and fail to recognize the poor specificity they are utilizing. As a result, the threshold for interventions they choose often end up becoming more likely to harm than benefit, and in most cases when this happens human beings default the doubling down rather than admitting they made a mistake in the first place. The only way to prevent these inevitably flawed assessments from greatly harming the citizenry is to provide them with blanket protections against excessive government interference in their lives.
In many ways, this problem is identical to the situation doctors are in where their decisions are guided by the fact they have no penalties for following FDA approved guidelines as elected officials are likewise protected from liability for harming people through bad public policies. One group, Make Americans Free Again (MAFA) has been exploring a range of legal strategies to stop the mandates. MAFA in turn has found filing notices of liability with the elected officials promoting the pandemic response (which removes their legal protection for the known harms that result from bad policies) has been the most effective strategy for making these officials rescind the mandates. I suspect removing the legal protection doctors have for prescribing drugs with known harms would likewise be the most expedient method to stop the high rate of injury that accompanies the unquestioned usage of dangerous vaccines and pharmaceuticals.
Recognizing Risks and Rewards
Within ancient China, there was an adage that said it is easier to raise an army of ten thousand men (since the world was simpler back then, ten thousand was commonly used as a metaphor for a very large number) than to recruit a single general to lead them. I believe this is because on the battlefield, there are an immense number of variables and factors you must pay attention to, and if some of these are overlooked, it can result in a catastrophic loss for an army. The default mode of perception for most human beings however is not to have this broad awareness of the whole picture (the view of a general) but rather to hyper-focus on certain things they have a pre-existing emotional draw towards. As a result, people rarely can comprehend the sensitivity and specificity for each policy they advocate for; instead, they can only recognize the half of the coin they have been prime to focus on.
In societies like ours where nearly every immediate threat to your existence has already been addressed by someone else, this mode of perception is unlikely to get you killed. However, in a merciless environment like a battlefield (which was very common in ancient China), or the chaos that occurs in a country when the government falls (something that is very difficult to even comprehend unless you have seen crowds of people suddenly snap in front of your eyes), failing to understand the risks and benefits of each choice you make can often be fatal.
I hold no ill-will towards peace-loving hippies, but when I have visited extremely liberal and affluent areas populated by these individuals (often termed limousine liberals), I have felt that if a war were to ever occur, they would most likely be the first to die because they would lack the ability to prioritize focusing on what was essential for survival and instead become paralyzed by trivial details that provoked their existing emotional fixations.
This may seem like an odd tangent to mention, but as increasingly dangerous events have been thrust upon the population (with the Covid vaccines thus far being the most dangerous) I have a genuine concern about many of these individuals who cannot clearly recognize the sensitivity and specificity of their choices given the significantly elevated risk of death that is likely to occur in the future we are moving towards. This blindness is likely why many individuals took the Covid vaccines and were then boosted despite clear warnings it was a bad idea to do with many long-term consequences.
Within medicine, this blindness to seeing both the risk and the reward of each choice is also present and many doctors cannot fully comprehend either for each medical decision that they make. Since I follow the philosophy of “above all, do no harm,” I will choose to not address a problem if I feel the approach I would use has a real risk of creating problems for the patient. As a result, my prescribing habits are very different from my colleagues because I will choose specificity over sensitivity when choosing medical interventions and I have made it a point to find medical approaches that I feel have acceptable risk profiles.
Somewhat similarly, the precautionary principle represents a mode of thought that is widely used throughout Europe which believes new technologies that interact with the human body should be viewed as harmful until they have been proven to be safe. The US holds the opposite philosophy, and by not following the precautionary principle can rapidly innovate and get new technologies to the market much faster than Europe, where significantly more safety testing to prove safety must be done before the technology is allowed to enter the market.
Like the Europeans, I follow the precautionary principle, and this has repeatedly saved me (and my patients) from being harmed by something that was prematurely brought to the market and later discovered to be quite harmful. Because discarding the precautionary principle significantly accelerates economic growth, it is unlikely the United States will ever adopt it as our accelerated economic capacity is a cornerstone of our status as a global superpower.
Unfortunately, failing to follow the precautionary principle also frequently results in a large number of deaths, disabilities, and injuries, that up to this point in the United States has been able to absorb the costs of. It is entirely possible the economic costs we will accumulate from the Covid vaccination campaign will be on a completely different scale and sufficient to displace the US as the top economic superpower and in the future trigger a major reevaluation of the value of following the precautionary principle. Likewise on a more personal level, since I often end up caring for the forgotten Americans who have been injured by these things, my life experience has created a bias for me to prioritize specificity over sensitivity when considering any new technology or pharmaceutical drug.
In summary, when considering a complex issue fraught with contention, there is almost always a risk-reward trade-off to each action or policy that is being proposed, and in most cases, individuals will tend toward prioritizing either sensitivity or specificity leading them to come into conflict with those holding the opposite prioritization. Because the nature of each problem and the currently existing tools for addressing it frequently make it quite difficult to develop an approach that has a suitable sensitivity and specificity (in cases where it is possible, the issue stops being an issue and actually becomes “settled science”), a situation is created where the two opposing camps fight over the issue, and eventually, a threshold is established that has a sensitivity and specificity most of the population can agree with.
The nature of this human dynamic leads to a few commonly repeating problems:
First, most individuals who are ideologically attached to a position or policy, due to the human tendency to not see the whole picture, will fail to recognize that there is always a risk to the reward of what they advocate for and more importantly not empathize with the fact their political opponents are sane individuals who are instead focusing on the inherent risk that accompanies their position or policy.
Second, most people fail to recognize that there is an immense degree of human variation, so as a result, an approach that may be suitable for one demographic of people is not suitable for another. Evidence-based medicine and population-based statistics have created a modern form of “scientific” medicine that treats patients as parts of a population aggregate rather than a diverse pool of individual human beings. For some patients, this approach works, and if you look solely at the aggregate data the algorithmic protocols proposed are “optimal.“
However, on an individual basis, this approach often fails, which has created a massive patient demand for the minority of doctors who treat patients on an individual level rather than as part of a group. It is also my belief that many of the individuals who design these algorithmic protocols do not consider the experience of each human being who is forced to go through them, and to some extent they cannot because there is no threshold for sensitivity and specificity that can be set which is suitable to the every member of the population-it will always be too high for some and too low for others. This problem is also a major issue within the health insurance industry where many requirements doctors and patients must follow to receive care are the results of questionable thresholds being established that do not meet the needs of many patients and subject them to a great deal of difficulty.
Although I do not believe the Covid vaccine should have never been allowed to go to market, they all had a risk-reward ratio that was much better for individuals who had a higher risk of dying from Covid, which was why the elderly were the first to be vaccinated once the vaccines became available. However, children have a nonexistent risk of dying from Covid, so it is completely and utterly inappropriate to treat them in the same manner the elderly are being treated – yet as we all know this is what has happened because many individuals who push collectivist policies do not recognize actual diversity exists within the population and that people are not all the same.
Third, activists typically fail to recognize that an existing solution to a problem is often the result of a great deal of work between competing parties to create a somewhat acceptable balance between sensitivity and specificity on a challenging issue and replicating that process overnight is impossible. Because they cannot see the other half of the picture, they instead demand everything to be changed to meet the sensitivity or specificity they are ideologically attached to and are blind to the consequences of doing this.
This problem was recently embodied by the defund police movement, which after being aggressively pushed through by progressive activists (who had many legitimate concerns about the corruption and malfeasance within their police force) resulted in large spikes of violent crime which eventually led many of the liberal members of the community to abandon these activists and beg for the police to come back.
Although the push to defund the police is the most well-known recent example, this incorrect assessment of sensitivity and specificity is by no means exclusive to the left and has likewise frequently come from the right.
Sensitivity and Specificity in Morality
Practical morality is intended to provide a system of rules that protects each member of society. As a result, it likewise runs into the same issue of sensitivity and specificity that will be found in any other intervention. Unfortunately, all of the same issues highlighted before apply to prescribed moralities and in most cases, individuals advocating for their preferred morality do not account for the inevitable risks that will result from their position.
For example, consider the contention that sexual intercourse should be reserved for monogamous marriage. The intended purpose of this policy is to ensure social stability and functional families that can propagate the existing institution into the next generation.
The downside to this policy is that it often results in individuals who should never have been married (as they are not compatible) being stuck together and having unhappy marriages that often traumatize their children. This downside to advocating for traditional sexual relations understandably leads many to rebel against the approach and have a large number of sexual partners…which likewise often backfires and prevents them from being able to form healthy and loyal relationships that can be sustained for the time required to raise children.
As outlined above, the key question with each form of practical morality is thus where is the acceptable balance between sensitivity and specificity-for example do you follow the model used in many parts of the world where pre-marital sex is punishable by death or do you embrace complete sexual liberation?
Unfortunately, much in the same way that corruption causes detection thresholds to be weighted toward sensitivity (so that pharmaceuticals and other medical products can then be sold to more people), political fixations cause proponents of practical moralities to weight their calibration towards implementing their ideology (increased sensitivity) while simultaneously downplaying the existence of harms from their approach which should necessitate also adopting a higher specificity.
The abortion issue perfectly represents each of the issues that emerge when you have conflicting moral prescriptions and policy decisions that prioritize the well-being of the mother or that prioritize the well-being of the baby. As was detailed in the previous part of this series, because the activist left chose to change the existing threshold to prioritize sensitivity towards supporting the mother, the resulting decreased specificity for protecting the baby created a large backlash against these policies which culminated in the previously inconceivable abolition of Roe v. Wade.
Because this issue has become so politicized, the risks and rewards of each option have not been clearly presented, it has remained an emotionally polarizing issue for much of the country. I believe the fact that in many places we are at the same place we were with abortion 50 years ago means something needs to be done to help move to a societal resolution on this issue. If this issue as I suggest is instead to be viewed through the lens of competing approaches to sensitivity and specificity, clear information on the benefits and harms of each approach is also needed.
At this point, I have seen numerous examples of each permutation that can occur with attitudes towards abortion:
•I have met many mothers who had abortions and have regretted the decision for decades.
•I have met mothers who kept their baby but have had an immense amount of guilt over the fact they strongly considered aborting them.
•I have met many mothers who feel eternally grateful that abortion saved them from a terrible partner, poverty, and creating a disastrous childhood for a future child.
•I have met mothers who hate and despise their children and state they wish they had aborted them.
•I have met children who were pronounced medically unviable (ie. Down Syndrome) and whose mothers were repeatedly but unsuccessfully encouraged to abort them by numerous doctors, who once born had no health defects and blossomed into amazing individuals.
•I have met many grown adults who said their mother strongly considered aborting them, but some outside factor prevented her from doing so, and as a result, these adults cannot ever allow themselves to be pro-choice.
•I have also met a few adults who wish their mother had not had them when they did, and instead terminated the pregnancy so she could have done it when she was better able to raise them.
•Lastly, I have seen many of the examples listed above occurring also occurring with the father.
All of this in turn argues that no threshold for sensitivity and specificity can result in a decision all the involved parties feel comfortable with. When situations like this arise, they often illustrate that the specific approach being utilized is not the actual solution to the problem. Typically, this is because the actual solution is not something anybody wants to examine (and partly because as is also the case for many other issues, too many activists in America are invested in perpetuating the abortion issue because it sustains their own personal power).
I would argue the two major problems underpinning the above dilemma are a lack of support for preventing pregnancy in the first place and a lack of support for helping mothers be in a good place to raise future children from. One of the largest studies ever conducted on the root causes of poverty found following three simple rules allowed 90% of people to escape poverty, and one of these rules was to wait until the age of 21 to get married and have children.
It is difficult to even begin to describe the impact of preventing most people from entering poverty, and this ultimately matters more than nearly any other health decision we could make. Similarly, as we are discovering more day by day, the economic costs from the lockdowns were orders of magnitude worse than any possible benefit to them. This was a result of our leadership allowing academic “experts” with a bias toward enforcing these policies to craft them, who then predictably chose a threshold that heavily weighted the sensitivity of preventing deaths from Covid through lockdowns over the specificity of preventing the unintended consequences of these lockdowns.
The saddest thing about this was that the main modeler who forecast catastrophic death rates if we did not lock down, Neil Ferguson, had repeatedly erroneously catastrophized pandemics in the recent past and received significant funding from Bill Gates. He also used a very poor model that should not have stood up to scientific scrutiny, and was later caught violating the harsh lockdowns he proposed to engage in an affair. However, most policy makers did not know this backstory nor were they given time to seek independent advice from the outside scientific community, so Ferguson’s flawed model effectively became law.
For the sake of brevity (as it is a very long essay), I will not go into the specific societal changes that could be created so we can have a much more nurturing and supportive environment that allows mothers to become pregnant at the right time and to be well supported is raising that child so that these mothers do not have to make the difficult decision over having an abortion in the first place. Nonetheless, I view the debate over the appropriateness of abortion to be similar to the ethical debate that occurs when there is a need to conduct an expensive highly risky emergent surgery for someone who had a problem that was never addressed early in the disease process (where relatively benign options were available) and instead was put off until it eventually became a medical emergency.
What are the Harms of Abortion?
One of the major issues with abortion that many lack awareness over is that abortions can be a dangerous and traumatizing experience. I believe this lack of awareness arises from the activist Left’s need to win this issue so they deliberately omit mentioning the harms associated with abortion (excluding the endless coat hanger references which have no medical relevance in our current era of abortion technologies).
In high school, I was once requested to monitor a 28 year old who had just had a surgical abortion as there was a risk of fatal blood loss for them after the procedure and they had no support within their immediate circle. When I was with this woman, I was astonished at how hard the abortion was on her body, as before this time I had been led by my sexual education teachers and the media to believe abortion was a quick, easy, and benign procedure.
In medical school and residency, I never attended a surgical abortion nor sought one out, but I did observe women going through medically induced abortions. I found that the medically induced abortion experience widely varied in severity (it was very difficult for some women, other women said it was not that much different from the painful periods had each month).
Seeing all of this made me wonder what harm directly correlated with abortion.
After researching the topic I found out there was evidence suggesting:
•Abortions expose mothers to an increased risk of death (this study found: “The risk of death from abortion (101 deaths per 100,000 ended pregnancies) was almost four times greater than the risk of death from childbirth (27 deaths per 100,000 ended pregnancies).”
•Abortions increase the risk of subsequently developing breast cancer (this study found abortions increase the lifetime risk of breast cancer by 2.5 times and discusses the politics of publicizing research). This topic is further discussed here.
•Abortions increase the risk of infertility (this strongly pro-life website cites a variety of studies demonstrating a significantly increased risk of infertility following abortion but not miscarriages). This is attributed to weakening the cervix or causing the placenta to grow in the wrong location, but I also believe it results from progesterone dysregulation (supplemental progesterone is often needed to maintain pregnancies and the abortion pill is an antiprogestogen).
In most cases, these same harms do not occur from natural miscarriages. Since each of these is a highly contentious scientific topic, they have not been sufficiently studied or published the medical literature. This is analogous to the scientific censorship we have seen regarding generic medications being used to treat COVID-19 or the potential harms of the Covid vaccines.
Potential Spiritual Consequences of Abortion
In the previous section, I attempted to discuss some of the more easily recognized effects abortion can have on the body and mind. Less easy to recognize effects include long-term psychological trauma, complex patterns of pain within the body, and significant exacerbations of chronic neurological or immunological illness. I have personally observed each of these following abortion (however it must be noted that for many women, there was no detectable change in health following abortion).
The spiritual consequences of abortion are much trickier to establish and likewise cut to the heart of the abortion issue. Taking out all the concerns of practical morality, the broader question with abortion is one of universal morality, whether or not abortion is murder, and if it is, at what point in the pregnancy it becomes murder.
There are two fundamental concerns with the answer to this question.
•The first is that if it is murder, then by failing to outlaw it, the government fails in its core responsibility of protecting the weak and vulnerable who cannot advocate for themselves. While there are many disagreements on what the role of government should be, virtually everyone agrees on this specific obligation.
•The second is that if it is deemed acceptable to murder under these types of circumstances, then it may also be deemed acceptable to euthanize the undesirable members of society. Many individuals are willing to have an abortion if they know their child will be born with Down Syndrome (although as the case of my friend mentioned before shows, the predictions from these routine tests are not necessarily accurate) but at the end of the day, this is not that far from the eugenicists sterilizing mentally handicapped members of the population, or the Nazis going a step further and executing them.
This principle may seem like something that is none of your concern, but, population control (as summarized here) has always been a fixation for the ruling elite, and evidence is continuing to emerge that the Covid vaccination program is a more advanced application of decades of work to develop sterilizing vaccines. In addition to supporting abortion under any circumstances, the activist left also tends to believe in the necessity of reducing the human population by any means possible (although they have the naïve belief that they are somehow superior and will therefore be spared from whatever depopulation approach that occurs).
One of the curious things about SARS-CoV-2 is that it has some very inexplicable characteristics that cause it to primarily kill the members of society who are the greatest burden on it (such as the elderly, the obese, and those with diabetes). This has led some of my colleagues with the greatest knowledge of the virus and its precursors to suspect the virus was created to thin the herd because our current resource consumption and financial obligations to the weaker members of society are not sustainable, and the dire need to address this has made governments around the world willing to go along with this program (except in Third World countries not sharing these demographic needs, which in some cases results in the vaccine-hesitant leader subsequently being assassinated).
There are hence a lot more consequences than people initially appreciate if they support abortion and abortion is in fact murder.
Like many other issues that have become heavily politicized, zealots will always dismiss inconvenient truths to push along their perspective. This is a major reason why the left so aggressively gaslights individuals who are having severe injuries from the Covid vaccinations; acknowledging that is occurring would weaken their political cause, and once you take all the fancy rhetoric and egalitarian aspirations for helping their fellow human beings espoused by political zealots out of the picture, you often find all they actually care about is being right and individuals who get in the way of them being right are typically tossed in the trash.
A recent example is many individuals complaining about bad reactions to vaccines being treated almost identically to individuals who gender transition and then realized they made a mistake and try to undo their transition. At first, when these victims adopt the desired political position (i.e. by vaccinating), they are fawned upon and embraced by their peer group, but once they flip to the opposite perspective, that group’s wrath is unleashed upon them, and any claims about looking out for their well-being go out the window.
For that reason, it is important to have an honest conversation about the topic, which includes honestly disclosing both the harms and benefits of abortion, many of which you have likely never heard of because it is not to the benefit of activists on either side to share them. However, it also touches on a much deeper issue that cuts to the core of what it means for us to be human.
My belief is that because many individuals do not want to consider the possibility that they committed murder (or it is irrelevant to them in comparison to their emotional and political needs) they close their eyes to the topic (in many ways displaying the same tendencies I attributed to doctors who refused to acknowledge pharmaceutical injuries), and some go even further to directly dehumanized the fetus and label it as nothing more than a parasite that is stealing from the mother and has no right to continue its parasitism.
This tendency to close your mind down to an uncomfortable topic is one of the key things that always allows mass genocides to happen. Because most of my family was executed by the Nazis while most of the German population could not bring themselves to open their eyes to what was occurring, I have always made it a point in my life to directly confront things that are uncomfortable and difficult to think about (for example what we do to animals in research and factory farming).
This then leaves us with a challenging question. How do we know if abortion is murder, and what type of sensitivity and specificity do we need to the possibility it could be murder?
In many ways, it is no different from the sensitivity and specificity required to convict someone for the death penalty (which to be fair, “pro-life” states, on account of their holding an increased sensitivity for executing murders often fail to protect innocent individuals from being executed). So far, I have skirted around the actual issue of murder by showing that the concerns of practical morality in many regards provide a clear framework to guide how this problem can be approached.
Spiritual Morality
Note: the following sections are likely to be the most controversial part of this article, and I request that if you disagree with me to understand that this is simply my best attempt to answer an impossible question. I also fully understand the need for shorter articles, but I deliberately avoided doing so here so that this section would not be presented in isolation.
A central belief of my faith is that if something is true, it will inevitably be discovered again and again. Likewise, once you begin to study each religion, after you get past the specific technicalities they disagree upon and go to war over, you will find there is a huge amount of common ground between them. This suggests they are all working with the same universal truths.
One of the things which makes the subject of spirituality so difficult is that a large part of the spiritual experience and spiritual knowledge arises from a realm that can only be contacted by a personal mystical experience that is not available to all members of the religion. This is often the basis for the ethical laws codified within a religion’s sacred texts, which must then be correctly interpreted by adherents of the faith.
In most cases, the best tool we have available to discern the nature of a universal morality is to find common ground within the religious texts each of us is receptive to. This is challenging to begin with (as so many different interpretations emerge) and further complicated by the fact political forces will always alter these texts over time for their own benefit (the Quran being the only exception I know of, due to Mohammed being instructed to codify within the Quran that it could never be changed).
I have concluded that spirituality and morality are inseparable because once you allow yourself to become receptive to universal laws, you are also bound to not violate those laws in your everyday conduct. A large part of the spiritual development process is thus gradually becoming able to bear witness to these universal laws, and in my assessment, the moral frameworks or rituals of each faith were deliberately designed to serve as initial stepping stones in the correct direction until you develop the ability to innately grasp the universal laws themselves.
My faith encourages each inherent to attempt to look to the depth of each situation encounter and then discern what the correct moral conduct is for that situation because once one becomes able to understand the essence of morality and how to apply it in harmony with one’s body mind and spirit, it enables the process of spiritual self-actualization. This can often be an incredibly complex task, and likewise, take decades to figure out. One major reason I went into medicine was to have to deal with difficult issues daily that challenge and refine my ethical constructs; unless you work in medicine, it is difficult to appreciate how many difficult ethical situations arise.
Spiritual Blindness
My favorite passage from the Bible is
Jesus said, “Father, forgive them, for they do not know what they are doing.”
Although like many things there are differing interpretations of this passage, my interpretation of Jesus asking God to forgive the romans for crucifying him is remarkably consistent with the ideas found within many eastern faiths. A key component to spiritual morality is being able to recognize the wide range of consequences that result from each action, including very subtle ones within the spiritual realm and ones that will occur far into the future. The notion of “karma“ is meant to encapsulate the equal and opposing reactions that ensue from each thing we do. One’s perspective on karma in turn changes with spiritual development because it gradually shifts from being an abstract concept to a tangible reality and a self-evident fact.
The dilemma many spiritual adepts encounter is having to bear witness to humans continually conducting “wicked” actions that create negative karma and ultimately harm the perpetrator far more than any possible benefit they got from the initial selfish action. One of the best contemporary examples relates to the Tibetan people, whom the Chinese government has gradually been ethnically cleansing so that they can acquire the rare earth minerals within the Tibetan plateau (strategically this is very important for China). A lot of truly horrible things have happened to the Tibetan people, but whenever I speak with them, their primary response is to feel immense sadness and compassion for the karma they can see the Chinese are creating for themselves by violating the Tibetan people and the Tibetan plateau.
Hence, much like Jesus said at the time of his crucifixion, if humans could understand the consequences of their actions, most of their destructive behaviors would stop. Unfortunately, this lack of consciousness is pervasive throughout society, and as we move into the trans-humanist future where everyone is disconnected from their bodies and lives within the Internet, the inherent human capacity to innately know what they are doing is wrong only further diminishes. Mattias Desmet, through his “Mass Formation Psychosis” concept likewise makes the case that the totalitarian state we are entering can only manifest in a society where everyone is disconnected from their body mind and spirit (with any luck my next article will be the review of his book I am working on).
What is Life?
Like many other challenging questions in our society, the question of when life begins is fraught with many epistemological questions such as how life is defined. It has thus remained a continual debate because we do not have an established framework in place that could answer this question.
One of the fundamental shortfalls within science is that it has no way to define what “consciousness“ is, which I believe arises from the fact our system of science works within the realm of human consciousness and hence lacks the perspective to see beyond it. As such, science can only identify components of the neurological system that appear to be linked to consciousness and describe patterns that are found in association with “consciousness.”
Once you branch into the alternative sciences, it does become possible to directly bear witness to consciousness and the nature of life, but at least from my perspective conventional science has been extremely resistant to embracing these topics because doing so challenges its authority as the sole arbiter of truth in the universe and the trans-human future we are walking into is incompatible with the existence of a soul or a spiritual life force existing within the body.
For example, it has frequently been recognized that approximately 6% of individuals who receive heart transplants will adopt the personality and behaviors of the heart donor. Books have been written on the subject, and the frequency of this occurrence should raise major questions as to the actual nature of our consciousness and where it resides.
In my worldview, every cell has a “biological consciousness“ (which grows in complexity as cells come together into a more complex mass), and every living creature has the potential to serve as a vessel a soul can inhabit. While the central nervous system is a remarkable interface for the soul with the body in the surrounding environment, it is not the source of consciousness, and as a result, any model that attempts to model consciousness without the existence of a soul faces an impossible task (that said, there are some very intriguing models that apply quantum principles to microscopic components of the nervous system).
One of the most common times individuals experience profound spiritual experiences is at the boundary of life and death. For example, when a mother gives birth a profound spiritual presence enters the room, in many individuals I know who are sensitive to that presence choose to enter obstetrics or midwifery so that they can bear witness to it on a regular basis. Similarly, at the moment of death when the soul leaves the body, a very powerful spiritual change also occurs and this has given rise to the documented phenomenon known as “shared death experiences,“ where individuals in a room with someone who just died experience something similar to a near-death experience (I have experienced both).
Throughout my life, I have asked a lot of spiritual teachers when they and their tradition believe the soul enters the body and the fetus transitions from having a biological consciousness (which is a form of consciousness) to having human consciousness.
The most common answer I have received is that shortly after conception, the soul is drawn to the mother’s body, and it typically enters the fetus after the fourth month of pregnancy (as this is when the fetus has become a vessel the soul can inhabit). If this is true, abortions that occur after four months have the potential to result in the death of a conscious being, and almost certainly result in the death of a conscious being one to two months later.
In addition to the physical and emotional consequences I have listed in the previous section, I also believe there can be energetic and spiritual consequences to abortion. Within Chinese medicine, it is believed that many of the problems women experience after abortions and miscarriages result from the energy of the fetus being retained by the body and not being released. I believe this energy is a reflection of the biological consciousness of the fetus, and I have met many women who had chronic problems in their bodies until they were able to release it from their system. As that requires exploring a model of medicine that is radically outside of the conventional paradigm, most women who encounter this issue will never have a means of addressing it.
I have also seen cases where both the mother and the father were adversely affected by the soul of the aborted child. As it is beyond my capacity to recognize when this is occurring, I am hesitant to provide any claims over what occurs, and simply leave it at this is a real issue that can occasionally happen to some people and is especially problematic for women who are highly sensitive to this realm.
Finally, in the section, I wanted to share that there any many issues with existing birth control options; for example I never trusted oral contraceptives because I know two women who became pregnant while on the pill and then had abortions. One of the most unfortunate ethical issues I discovered in the past is that one commonly used form of birth control, the injectable Depo-Provera (which was the WHO’s method of choice for sterilizing the third world before the technology existed to do it with vaccinations), has a relatively unknown mechanism of action. In addition to preventing pregnancies by preventing ovulation and blocking sperm from being able to pass through the cervix, it also will cause spontaneous miscarriages to occur if fertilization nonetheless occurs.
For example, one friend of mine who did not wish to have a baby became pregnant while on Depo-Provera, then decided she wanted to keep the child, after which she had a traumatic miscarriage in the shower that took her a long time to get over.
The Covid vaccinations appear to be able to create a similar effect (as I have now come across many cases of late-term miscarriages you rarely see normally) that are coinciding with a historic drop in fertility around the world. Beyond the heartbreak of losing one’s child, I suspect that many of these women will also develop some of the unresolved issues that can follow a miscarriage or abortion later in pregnancy.
The Timing of Abortion
Because people will always try to argue and push the limit on any point, it is often necessary to draw a hard boundary no one can ever cross. For this reason, I understand why the religious right considers abortion at any stage of pregnancy to be murder and unacceptable under any circumstances; once you compromise on this area, before long you will have activists pushing for late-term abortions. Nonetheless, I do believe there is a huge difference in the trimester of abortion when considering the morality of the event and the harm it creates to the mother, so to equate them together by using the same label ("abortion") is extremely disingenuous.
For reference, the trimesters are as follows:
•First trimester: Weeks 1 to 12 of the pregnancy (months 1-3)
•Second trimester: Weeks 13 to 27 of the pregnancy (months 4-6)
•Third trimester: Week 28 to the end of the pregnancy (months 7-9)
In the previous section, I outlined a spiritual framework for why I believe the fourth month constitutes the threshold for where major ethical concerns can no longer be ignored with abortion.
Many pro-life activists believe this occurs at six weeks when the heartbeat starts and I am open to this viewpoint given the transfer of consciousness that can occur following a heart transplant, but at the same time, I feel it creates an unrealistic standard because many women will not realize they are pregnant at six weeks (and unrealistic standards cannot be implemented; the failure of the war on drugs is an excellent example).
In addition to religious beliefs on the subject, there is also a medical basis for determining what constitutes life. With our currently existing medical technology (it is entirely possible in the future they will attempt to grow babies in artificial wombs), it is impossible for a fetus to survive outside of the mother in the first trimester, and very challenging to survive in the second trimester:
The most premature baby to survive is Curtis Zy-Keith Means (U.S.A.) who was born to Michelle Butler on 5 July 2020 at the University of Alabama at Birmingham Hospital in Alabama, U.S.A. at a gestational age of 21 weeks 1 day or 148 days, making him 132 days premature.
When the subject has been studied, usually, the earliest a baby can survive is about 22 weeks gestation, while the age of viability is often defined at 24 weeks. At 22 weeks, there's a 0-10% chance of survival; at 24 weeks the survival rate is 40-70%.
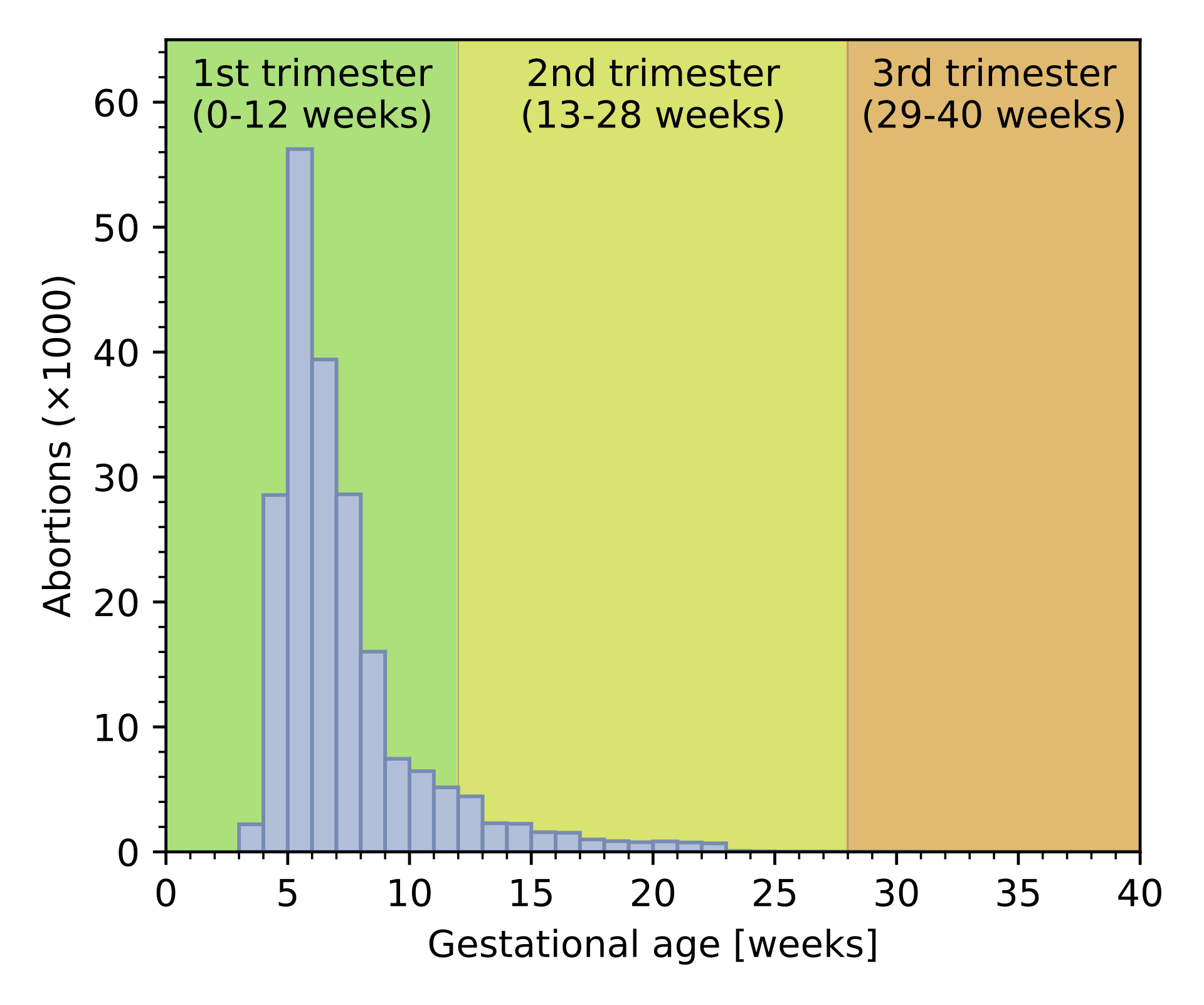
Let’s now look at when abortions are typically conducted within United States with this 2016 dataset (remember, the non-surgical pharmaceutical abortion method that will likely become more popular once abortion is banned in Republican states can only be done in the first ten weeks of pregnancy):
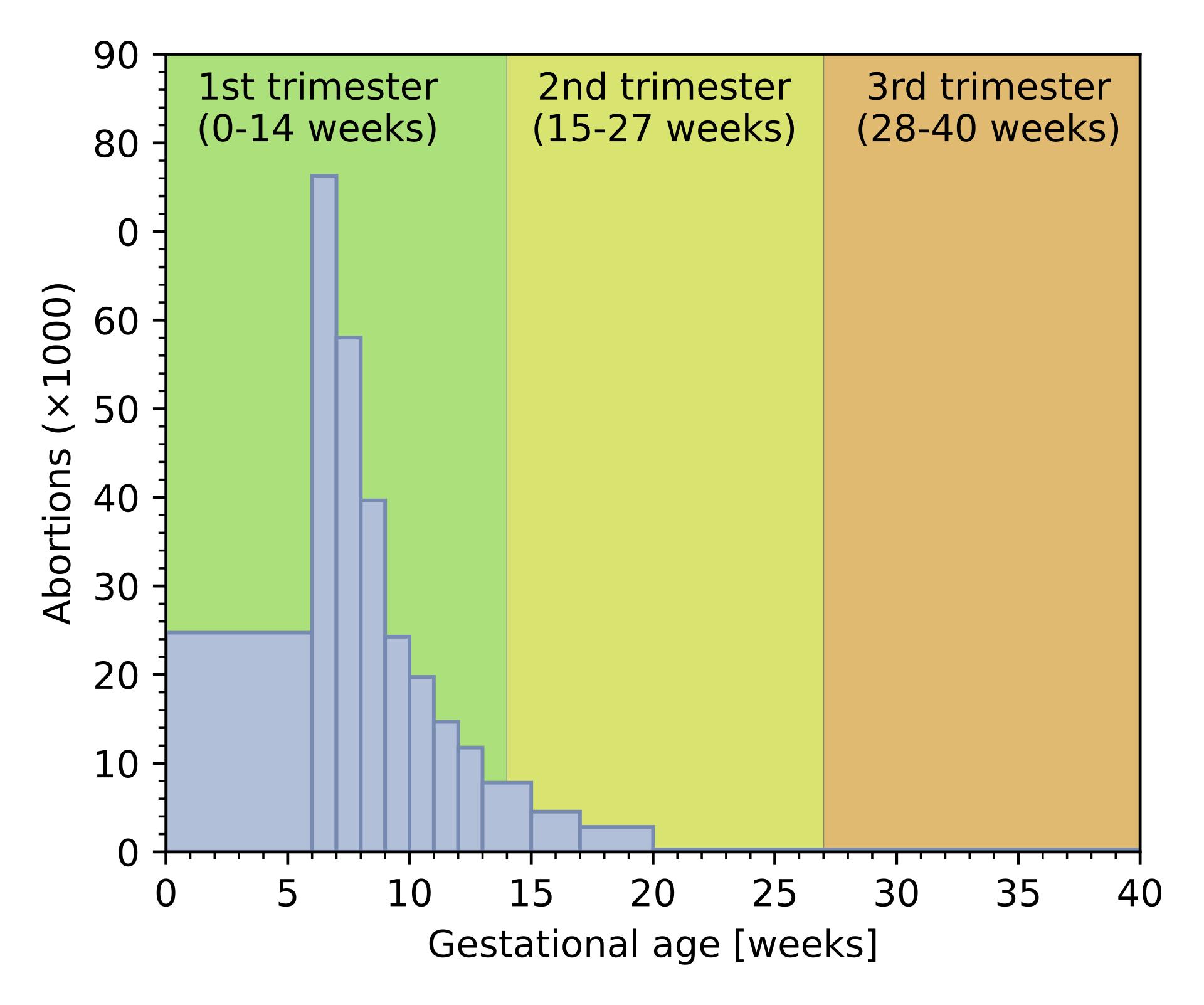
(Similar Results are were also found in 2019 England and Wales):
Approximately 1% of the abortions performed within the United States occur when an infant could survive outside of the mother, and one of the reasons why New York’s (highly partisan) 2019 Reproductive Health Act upset so many people was because it provided legal protections for this practice. I have also attended guest lectures provided at medical schools by gynecologists who provide late-term abortions, and these individuals are typically viewed as heroes standing up for women in desperate circumstances against the hateful religious right.
When I looked at some of those cases individually, the degree to which late-term abortions can be justified highly varies. For example, while there are lots of ways to rationalize it, I do not think it is acceptable to execute a living human being because having a child creates a significant lifelong burden for the mother and the mother was unable to get an abortion earlier in the pregnancy. On the other hand, some cases involve real medical risks to the mother if she continued the pregnancy and hence are a much more ethically challenging subject. This moderate stance unfortunately put me in serious conflict with the audiences of those lectures.
Liberty & Ethics
I have been very close to individuals who have lived both in America and the worst communist dictatorships in the world. One thing a few of them have told me is that “the price of living in a free country is needing to allow people to do stupid and self-destructive behaviors.” Regardless of how tempting it is to interfere in the lives of others and spare them from the suffering they are creating for themselves, once you open that door, the state will always abuse it to force you to do a variety of abhorrent things.
For this reason, I believe sensitivity and specificity must always be calibrated to take into account the potential consequences of a policy or intervention and generally support the following types of laws:
•Providing strict penalties for those who deliberately commit harm to others. This includes criminal convictions for murder.
•Laws that prevent a predatory party from preying on the vulnerable public. This can include outlawing the sale of a problematic product or requiring the placement of visible warning labels on it.
•Requiring that any mandated conduct or action that is believed to save lives does not expose the recipient to additional risk. Requiring seatbelts is one such example, banning drinking when driving is another, but mandating a potentially harmful vaccination is prohibited within this framework.
•Policies that incentivize good behavior without penalizing individuals who fail to abide by those policies. Tax breaks for having children are one such example.
•Requiring that laws that violate the rights of an individual for a greater good can only be permitted if the benefit of this violation significantly exceeds its potential harm and an individual court hearing is required to force this violation. Because it is not feasible to widely implement a policy of this nature (a judge could likely only process a few of these cases a day), this safeguard prevents the policy from being implemented except when it is absolutely necessary.
I also believe that individuals with an inherent conflict of interest in determining a policy should be prevented from dictating it, such as the many corrupt officials I have highlighted through this substack who pushed though their sponsors drugs on the public, or the parties who profit from selling aborted fetal tissue (there is a large demand for this material).
At the same time, this stipulation must also apply to everyone else. For example, I noticed most of the individuals who fervently supported the lockdowns had work-at-home jobs where it benefited them to be in isolation, whereas the individuals who could not transition to a remote position and became unemployed were typically the ones who oppose the policies.
I believe that if those workers (i.e. teachers) had not been able to transition to a remote job they likely would have protested against the lockdowns and chosen to mention the fact they were highly detrimental to the responsibilities of their profession (i.e. that the lockdowns have had had devastating effects on adolescent education that will ripple out for decades). For this reason, it was not appropriate for them to be able to advocate for the lockdowns.
Medical Ethics
I agree with the four principles of medical ethics described earlier in this series (respect patient autonomy, do no harm, maximize patient benefit, fairly distribute care to all your patients). Because each of these appears self-evident I am not sure of the value of restating the parameters associated with these principles.
I do however have a few perspectives that go beyond the conventional explanations attached to them. In general, I believe that it is important to treat each patient as an individual rather than adopting an algorithmic approach for everyone as this approach negates many of the benefits these four ethical principles can create.
More specifically, I prioritize informing the patients over what they are consenting to (which typically is not done properly in medicine), I make a large effort to ensure my care of one patient will not adversely influence my care of another patient (this is one reason why it is very important to set appropriate boundaries), and I try my best to make things affordable while maintaining boundaries so I am not overwhelmed by requests for free medical care that burn me out (I have to be careful on this one as I innately like helping people).
When I first began my medical education, one of my spiritual teachers told me the most common form of negative karma doctors accumulate results from them failing to treat a patient as a result of neglecting training that was provided in the past (which had they learned properly would have made them able to help the future patient). I feel this concept is encapsulated within the medical principle of beneficence but it rarely receives the attention it deserves.
Doctors regularly interface with the boundary of life and death and occupy the role traditionally held by priests in the society. Because of this, each doctor will engage with situations that have profound consequences for their patients, and, although many doctors do not realize it, for the soul of the doctor as well.
Because my morality system is framed around trying to discern the essence of each event I encounter, I often become aware of ethically questionable practices that are overlooked by my colleagues.
For example, watching infants and toddlers struggle with all their might in protest against vaccination (which the nurses laughingly dismissed as nothing more than a silly needle phobia) and then seeing the immediate trauma and damage that arose in the child’- body, mind, and spirit after vaccination made it very clear to me that something was very wrong with this practice. Furthermore, I can still clearly remember how conscious I was at their age, and I feel I had a sufficient degree of consciousness back then to be able to refuse consent. Similarly I have also met a few people who have memories of when they were inside their mother (and many more who did following hypnosis), although I have no possible way to quantify when in the pregnancy these memories occurred or their consciousness emerged.
Witnessing the various subtle harms created by a wide range of medical procedures has made me very cautious over which medical approaches I will utilize and has left me with the belief it is critical to fully respect a patient’s desire to decline a medical intervention. If, after being fully informed a patient says no, there should be no penalties for the patient doing so, and to do anything else opens the door to a dystopian situation like what can occur in a totalitarian communist regime.
On many levels, accepting that your medical education has only opened the door to being able to understand the entire human experience is a very scary prospect, especially since doctors are held to a standard where they are expected to be the definitive experts on the body mind and spirit. I believe this fear is one of the underlying reasons why medical science always seeks to create simplistic models that removes complexity from nature.
However, being able to recognize that life is a tapestry of complexity you will likely never fully understand is what ultimately makes life much more enjoyable and fulfilling because each day is a new discovery that broadens your horizons of what can exist within the body, mind, spirit, and universe.
At least in my case, this has process been one what prevented me from burning out and makes me excited to go to work each day. There is an immense amount that lies in front of each of us especially when we can fully interact with a fellow human being, and becoming perceptive to this realm is the only means I have found to address many of the complex ethical questions we encounter in medicine and the complex challenges our patients bring to us.
Conclusion
Sensitivity and specificity is a fundamental aspect of human society we will never be able to avoid having to deal with. In some cases, the whole topic is very straightforward – for example shooting someone in the head with a bullet has a relatively high likelihood of accomplishing the intended effect and nothing else (although there are individuals who are able to survive gunshot wounds to the head).
However, in many other cases it is not clear-cut, and in those cases determining the correct threshold to establish for sensitivity versus specificity requires both accurate knowledge of the sensitivity and specificity of your approach and the wisdom to understand how to appropriately calibrate between the two. This is somewhat analogous to evidence based medicine being supposed to just utilize “evidence,” but also use clinical wisdom and patient values to determine the appropriate ways to implement that evidence. Since these critical steps are often skipped, evidence based medicine has often failed to produce the benefit to society it was expected to.
I believe accurately setting these thresholds requires one to be honest with themselves about their existing biases and to fully appreciate the consequences of having too low of a sensitivity and too low of a specificity. An extreme version of this argument is "you may have no way to know if heaven or hell exist, but eternal damnation is such a terrible fate you cannot afford to take the risk, no matter how small it might be, that being an atheist entails if they do in fact exist.”
I agree that this is an unreasonable standard and were it to be followed, our lives vou/d become nothing more then enslavement to each new fear that was brought our way (which sadly has happened to the large part of our population who locked themselves away from society and still allow themselves to be enslaved by the Covid propaganda campaigns). However, when we touch on issues relating to life itself, there needs to be humility that considers the possibility what we are doing could be murder and that life is something sacred we have a responsibility to honor.
Beyond policies we enact in the real world, this also holds true within our own minds. Earlier in the article, I cited the example of a paranoid individual who is not that different from an overly sensitive PCR test in his ability to erroneously detect grave dangers in his environment.
One of the challenging facts I have how to come to terms with is that many individuals who fanatically advocate for the lives of others do not actually care about those individuals. Rather they care about the political capital those deaths create (the screenshot above is one such example). This is why you will see political activists get hysterical when certain types of deaths occur, but ignore or gaslight me occurrences of other types of death. I think this is very sad both for the consequences it creates in the real world and for the fact that it makes each adherent of that ideology dead inside.
As much as I would like to pick on one end of the political spectrum, I believe this tendency is just another fundamental aspect of human nature. For this reason, introspection is always needed to determine the sensitivity and specificity of your own internal value system and if it has been appropriately calibrated to prevent the potential consequences that could result from an inappropriate internal threshold.
My hope in writing this article has been to make the case that it is to the benefit of all of us to err on the side of protecting life in each choice we make. In certain cases, that will certainly be extremely difficult to do when, such as when a challenging pregnancy situation emerges. However, it many other situations it will not be, provided you have already created an internal inertia that drifts towards choosing life. On many levels, that inertia is one of my deepest values and is something that I believe is necessary in order to become truly alive and fully embody the precious human experience you were gifted with by being born here.
Let me know what you thought of this, as it goes into some highly controversial territory. I spent a lot of time working on it so hopefully it can somewhat convey what I’m trying to show. Thank you for your feedback!
It is highly regrettable that abortion, which is a complicated and sometimes dangerous medical procedure, a family planning tool, a population control tool (preventing some births with known fetal abnormalities), sometimes a medical tool (if the mother has certain health problems) is discussed with such fervor, toxicity and hate on both sides.
My dream is being able to discuss it with some compassion, understanding of many circumstances, and yet ALSO respect for the young life being carried, and for the complexity of intersecting interests.
Do the mother's interests matter? Yes
Is the unborn child a child? Yes
How to balance it? That's a hard question. But do NOT shy away from it.
A world with no abortions, or a world with no regard for life of the child, would be a mean world.
Unfortunately, abortion is a wedge issue, useful to exploit politically for both parties and their sponsors, so it will remain a toxic topic.
Excellent paper from a spiritual, emotional and physical level. As an obstetrician, these discussions are encountered on a daily basis. I have never in my career nor as a resident done an abortion. There are so many stories from an infection from a metal clothes hanger to a woman who delivered, and 4 weeks later decided to put enough dirt down her baby’s mouth and soffocate him. To a young gal who knew she couldn’t raise the baby and I coordinated the adoption. Another incident where, during the csection the girl crying finally said her father did this to her. You try, as a physician to navigate these social issues the best you can and take them home with me , hoping and praying that God has given me (or any physician) , the wisdom to help your patients and honor the oath you took. These times we live in are so politicized that nativigating through them have been terrifying for me . I loved my job but no longer happy I picked this specialty. I pray that someday, when I am judged I always advised my patients appropriately. Thanks amidwesterndoctordoctor and Tritorch for your enlightened and heartfelt discussions.