Hundreds of Studies Show DMSO Transforms The Treatment of Cancer
A remarkable cancer treatment has been hiding in plain sight for decades

Story at a Glance:
Dimethyl sulfoxide (DMSO) effectively treats a broad spectrum of conditions, including strokes, pain, tissue injuries, autoimmune inflammation, and cancer.
DMSO inhibits cancer growth and consistently reverts cancer cells to their normal state.
DMSO enhances cancer visibility to immune cells, enabling the body to eliminate tumors previously undetected by the immune system.
DMSO effectively mitigates major challenges in conventional cancer care, such as radiation damage, chemotherapy toxicity, and pain from "incurable" metastatic cancer.
DMSO markedly boosts the efficacy of many chemotherapy drugs, allowing safer, lower doses to achieve the same results.
When paired with certain natural therapies, DMSO often produces highly effective cancer treatments, revolutionizing cancer care.
Note: this is part one of a two part series. In the second part of this series (which can be read here), I explore how DMSO in combination a natural dye creates a remarkable cancer treatment which safely treats a variety of otherwise challenging cancers.
Cancer is one of the most challenging conditions to deal with in medicine, as two seemingly identical cancers can have very different causes. As a result, any standardized (holistic or conventional) protocol will inevitably fail some of the patients it is meant to treat.
Furthermore, since there is so much fear surrounding cancer (e.g., from what the primal fear brings up inside you, from how your social circle reacts to it and from how the medical system uses all of that to push cancer therapies) it is often very difficult to have a clear head about the ordeal or find the right source of advice.
Likewise, since so much money is involved (e.g. 65% of oncologist’s revenues comes from chemotherapy drugs and cancer drugs are by far the most profitable drug market), there is significant pushback (e.g. from medical boards or unhappy relatives) against anyone who attempts alternative cancer therapies making it very difficult to practice unconventional cancer care—particularly since no alternative treatment works all the time.
Note: in a recent article, I highlighted how urologists initially would not touch Lupron (which is now also used as a the puberty blocker) because of how unsafe and ineffective it was, but once they started being paid a lot of money to prescribe it for prostate cancer, it rapidly became their number one drug.
In contrast, while the conventional cancer therapies often have serious issues that make them far worse than any benefit they offer, some conventional cancer therapies are frequently the only available option which can save someone’s life (which has led to me at different times having fights with close friends or relatives either not to do chemotherapy or to get them to start it in cases where I felt it was absolutely necessary).
Given all of this, I presently believe that no “ideal” cancer treatment exists, but if it can be done (e.g., it’s effective for the cancer and feasible to implement), the most ideal to least ideal treatments are as follows:
•Identifying the root cause of a cancer, removing it, and having it quickly and permanently go away on its own (which is sometimes possible).
•Have enough time to rebalance the body so that its terrain no longer supports the cancer and the cancer can fade away on its own (which is often doable but a fairly involved process many have difficulty carrying out).
•Significantly enhance the function of the immune system so that it will eliminate the cancer.
•Find a treatment that is toxic to the cancer but relatively benign to the rest of the body.
•Find a treatment with an acceptable toxicity level and find ways to mitigate its side effects.
•Accept a moderately toxic treatment with significant side effects.
•Focus on living with the cancer rather than curing it and then finding ways to mitigate the symptoms you experience both from it and any existing treatment protocols.
•Use a costly conventional therapy that is unlikely to work and live with all the side effects until your life ends (which in more extreme treatment regimens can be quite severe).
If we take a step back, what’s truly remarkable about DMSO, depending on how it is used, is that it can effectively provide most of the benefits listed above with the least amount of collateral damage (e.g., side-effects, toxicity, etc.).
Dimethyl Sulfoxide (DMSO)
Exactly six months ago, I used this newsletter to bring the public’s attention to DMSO, a simple naturally occurring compound that has a number of immense therapeutic benefits and virtually no toxicity (detailed here). In turn, when it was discovered in the 1960s, it quickly became America’s most desired drug (as it cured many incurable ailments). A lot of the scientific community promptly got behind it and before long, thousands of papers had been published on every conceivable medical application for it. Consider for example this 1980 program 60 Minutes aired on DMSO:
As such, throughout this series, I’ve presented the wealth of evidence that DMSO effectively treats:
Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
A wide range of tissue injuries, such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
Many challenging infectious conditions, including chronic bacterial infections, herpes, and shingles (discussed here).
In turn, when I published this series (because of both how effective and easily accessible DMSO is) it caught on like wildfire, this publication went from being the ninth to top ranked newsletter in the genre, there was a nationwide DMSO shortage, and I’ve received almost two thousand testimonials from people who benefitted from DMSO (and often had remarkable results—particularly for chronic pain).
That response was quite surprising and in my eyes, a testament not only to how well DMSO works, but more importantly, how effectively DMSO’s story was erased from history (e.g., many long-time enthusiasts of natural health shared that they were blown away they’d never heard of it). This sadly illustrates how effectively the medical industry can bury anything threatening its bottom line (e.g., the FDA—for rather petty reasons—used everything at their disposal to make sure DMSO was forgotten).
In turn, within the DMSO story, I believe one of the least appreciated (or even known) facets of it are the remarkable contributions DMSO makes to the treatment of cancer—which is even more remarkable given that far more research has been done with DMSO and cancer than all the other topics I just listed. Consequently, for months I’ve wanted to publish an article on this (particularly since one incredible natural cancer therapy utilizes DMSO), but simultaneously, it just wasn’t feasible to as there was so much literature to go through.
That’s been weighing on me considerably (e.g. many readers have asked me to prioritize this article over everything else), so over the last three months (and particularly the last three weeks), I shifted my responsibilities to focus on the topic thoroughly. While it took a bit of a toll on me, the article is now done. As such, I greatly hope some of what’s in here can benefit you and I likewise thank each of you who has supported this newsletter and made it possible for me to spend so much time delving into these critical forgotten sides of medicine.
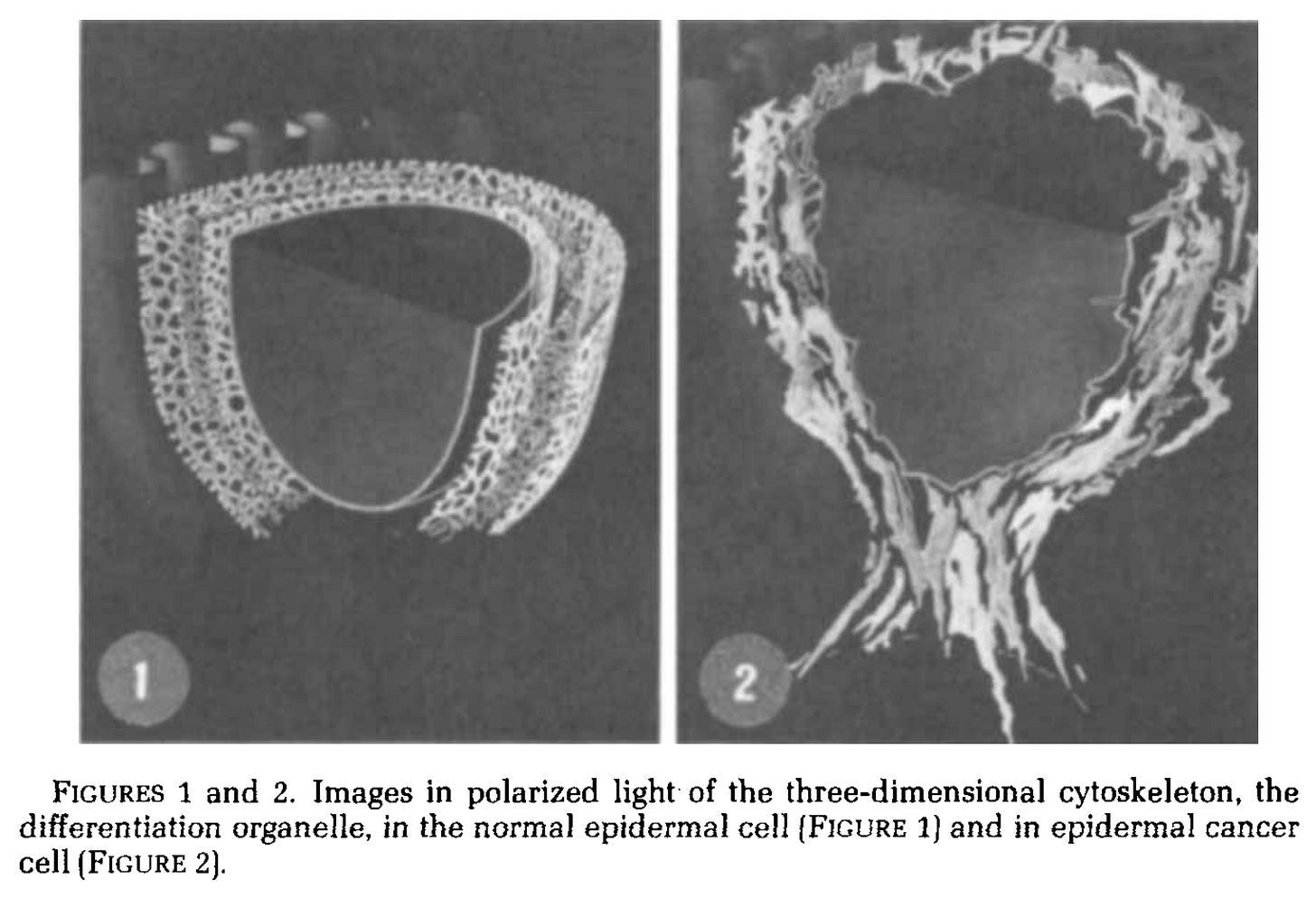
Cancer Differentiation
When life begins, the first cell has the potential to turn into anything. Then as it divides, its range of possibilities becomes more finite until each needed type of cell populates its assigned region of the body. This process is known as differentiation, and is a frequent interest in medicine as undifferentiated cells (e.g., stem cells) can replace lost cells by differentiating into them. Cancer is a disease of dedifferentiation where normal cells adopt an ancient survival program, lose their structure, order, and connection to the whole body, and instead voraciously divide through the body and consume it.
As such, an agent that could induce differentiation of cancer cells so they become normal could be immensely helpful in treating cancer. Unfortunately, only one “effective” agent has entered general medical practice, all-trans retinoic acid (a metabolite of vitamin A) for the treatment of promyelocytic leukemia (a relatively rare cancer).
There are now twelve tumor-cell types in the test tube in which DMSO tends to stimulate the tumor cell toward changing into a more normal cell, Dr. Jacob told me. — Morton Walker 1983
Sadly, to quote a 2023 review paper that compiled many studies where DMSO differentiated cancers:
Recently, DMSO has been included in biological cancer treatment and several FDA approved cancer immune therapeutic modalities such as CarT cell therapy and melanoma drug Mekinist (trametinib DMSO). However, besides its recognized biological role as a pharmaceutical solvent and cryoprotectant, there was no mention of DMSO’s possible ability to potentiate therapeutic activity as a component of these cancer treatments.
Note: while there is a general bias in medicine to avoid researching natural cancer therapies, DMSO has been extensively used in cancer research because it effectively facilitates many aspects of it (which had led to the truly curious scenario described above).
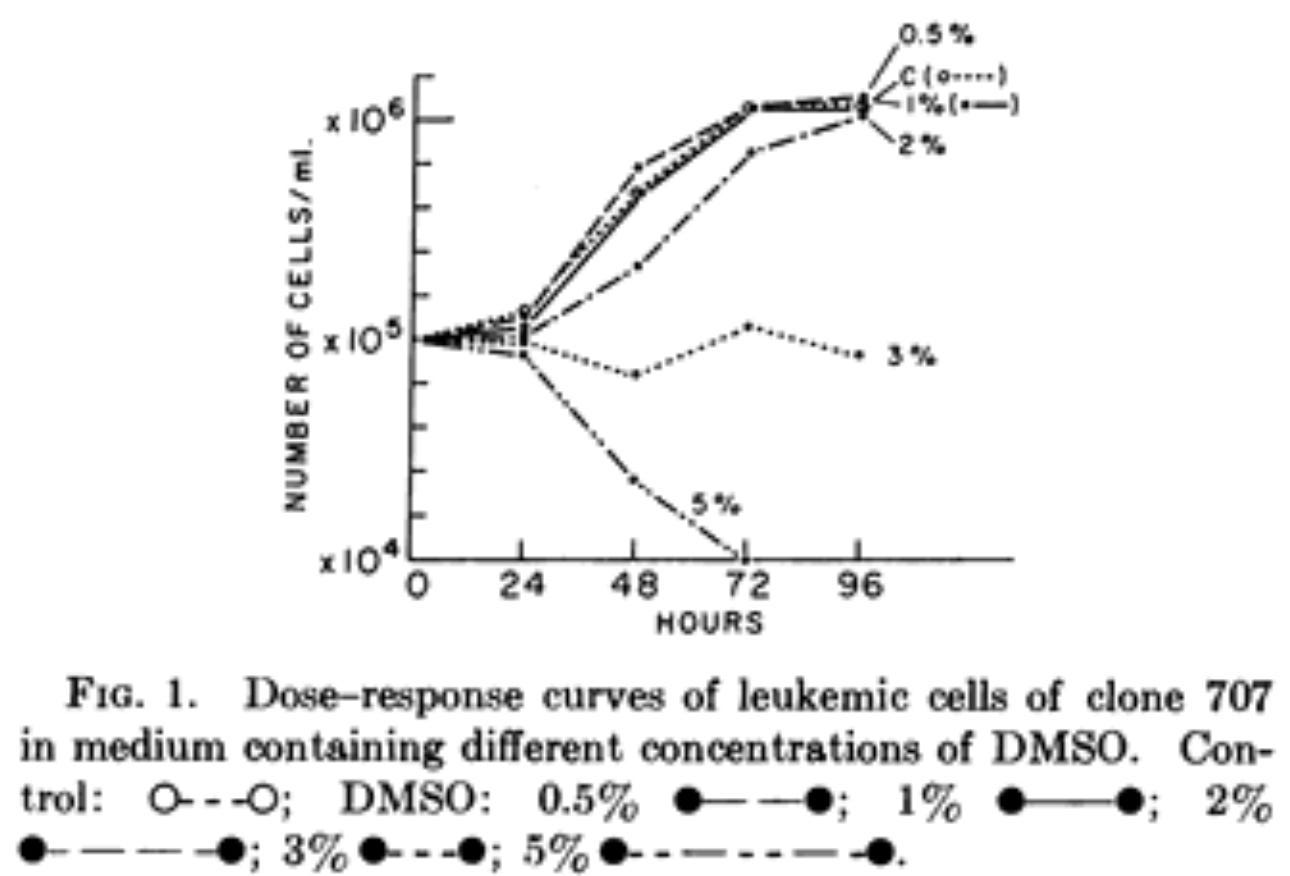
This saga began in 1971 when one of the nations top virologists accidentally discovered that if DMSO was given to leukemic cells (specifically erythroblasts—which cause a relatively rare type of cancer), at a 2% concentration, it caused most of them to differentiate back to normal cells (which took up to 5 days), at 3% it stopped their growth, and at 5% it killed them.
Additionally:
•Mice injected with the DMSO-treated cancer cells lived roughly twice as long as those injected with untreated cancer cells (suggesting DMSO made the cancer less aggressive).
•The cancer cells did not evolve resistance to DMSO (although subsequent research sometimes showed a small portion of cancer cells in a tumor were resistant to DMSO1,2). Additionally, for erythroleukemic cells that were resistant to DMSO inducing differentiation, butyrate did induce it (while butyrate and DMSO each antagonize the inducing action of the other).
Eight months later, she published another study that found that within five days, 2% DMSO caused 95% of erythroleukemic cells to differentiate. This was followed by studies that:
•Explored the mechanisms of differentiation, provided detailed descriptions of it, and showed it occurred in a consistent manner.
•Explored how certain steroids blocked (or supported) DMSO’s ability to induce erythroleukemic differentiation.
•Found increasing concentrations of DMSO caused increasing alterations of cancer DNA (which was an initial step in the differentiation process).
• Found the differentiation continued long after DMSO was no longer present and could be irreversible.
•Found the differentiation did not appear to be synchronized with the cell cycle.1,2
Following this, it became generally accepted that DMSO differentiates erythroleukemic cells, and decades of studies corroborated that.1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62
Note: DMSO’s ability to differentiate erythroleukemic cells was so well recognized that in 1992, it was selected for a microgravity experiment on the international space station.
Since erythroleukemia is closely related to the more common acute lymphoblastic leukemia (AML), decades of studies also showed DMSO differentiated AML.1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95
Additionally, DMSO was also shown to differentiate many other cancers.
Blood Cancers: acute promyelocytic leukemia,1,2 chronic myeloid leukemia,1,2,3 cutaneous erythromyeloleukemia,1 hairy cell leukemia,1 histiocytic lymphoma,1,2,3 non-Hodgkin lymphoma,1 T-cell leukemia,1 T-cell lymphoma1
Organ Cancers: bladder1, brain,1,2,3,4,5,6 breast,1 colon,1 esophageal,1,2 intestinal1,2 kidney,1,2 liver,1,2,3,4,5,6,7,8 lung,1,2,3,4 prostate,1,2 rectal,1 ovarian,1,2 stomach1, thyroid1
Other Cancers: embryonic carcinoma (into heart cells),1,2,3,4,5,6,7,8,9 fibrosarcoma,1,2 melanoma,1,2,3,4,5,6,7,8,9,10,11, nasopharyngeal,1 rhabdomyosarcomas1,2 tumors (in potatoes)1
Collectively, these studies showed:
•DMSO normally differentiated the cancer (it was rare for me to find studies where it did not) and did so in a dose-dependent fashion (e.g., 0.5-2% was often used). At higher concentrations (e.g. 1.5%), those changes were often permanent. However, in some cases, a minority of DMSO resistant cells did form, which then required another differentiating agent.
•Cancer growth, proliferation, and survival in tandem frequently decreased. In parallel, tumor suppressing genes (e.g., P21, PTEN, RB) increased, tumor promoting proteins were suppressed, and the cancer cells were weakened (e.g., with transient DNA strand breaks1,2) or induced into programmed cell death. Conversely, cancer triggers (e.g., C-myc1,2,3, C-myb, nucleolar antigen p145) were suppressed.
•Many metabolic pathways (e.g., JAK–STAT, ERK, NF-kB), histone H2A phosphorylation, and key cellular enzymes were increased during differentiation (e.g., Protein Kinase C,1,2,3 PI 3-kinase, TXA2, and TXB2 synthase, COX-21,2, 5-Lipoxygenase, phospholipase, CYP3A4, cytochrome b5 reductase and drug metabolism, acetylcholinesterase, carbonic anhydrase,1,2 disphosphase, and diaphorase).
•Other proteins and receptors were also increased (e.g., GPI-80, angiotensin II, Desmoplakins and Fibronectin) as were a variety of metabolites and signaling molecules (TNF-α, melanin, diacylglycerol inositol). Intercellular calcium was also increased1,2,3 as was the ion flux in and out of cells (except for potassium), the cellular transport of nucleosides. Finally, there were changes in G-protein signaling, and some cells were sensitive to staphylococcal leukocidin.
•Certain aspects of metabolism decreased (e.g., glucose transport, insulin receptor availability, general protein and transferrin synthesis, diacylglycerol synthesis, glycosaminoglycan synthesis and sulfate incorporation, heme oxygenase-1 activity,1,2) along with a decrease in histone expression and the association of Phosphatidylinositol-Transfer protein with the nucleus.
•Some things increased DMSO’s differentiation (e.g., TNF-α1,2,3, sphinganine, alpha-lipoic-acid, PP2, or suppressing PTEN) while others suppressed it (e.g., asbestos1,2, dexamethasone,1,2 hydrocortisone, hyperthermia, diacylglycerols and phospholipase C, blocking protein kinase C, lithium chloride, Mu IFN-Alpha1). Additionally, low frequency EMFs did not affect it.
Note: other agents also exist that can sometimes induce cell differentiation, but in many cases, DMSO works much better (e.g., oxytocin can turn certain cells into heart cells, but does not fully differentiate them if they are initially only one layer, whereas DMSO does).
•Vitamin D has been repeatedly found to synergistically enhance DMSO’s ability to differentiate AML1,2,3,4 (except in this study) and to commit AML to differentiate into macrophages1,2 while it counteracted DMSO differentiating erythroleukemia.1,2
•Retinoic acid (a vitamin A metabolite) has also shown promise for inducing cancer differentiation, works synergistically with DMSO1,2 and uses a different differentiating pathway than DMSO.1,2
In addition to these biochemical changes, some other effects of DMSO have been proposed to explain its differentiating activity (e.g., one study proposed that DMSO’s interactions with free radicals allowed it to induce differentiation).
Note: I have strong ethical objections to animal research and it is my sincere hope that since so much of it has already been done that it will not need to be redone to “prove” DMSO works.
Structural Changes
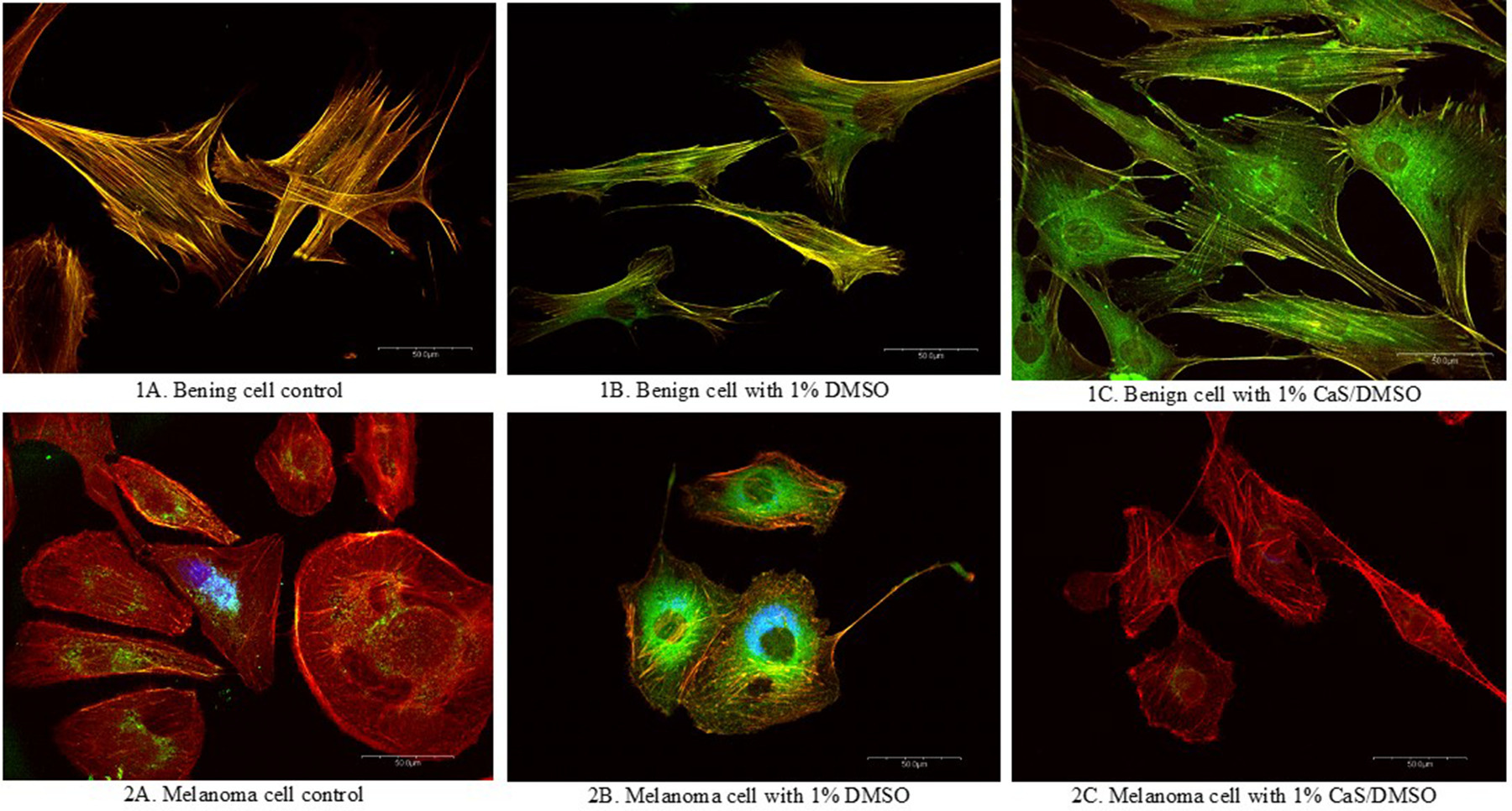
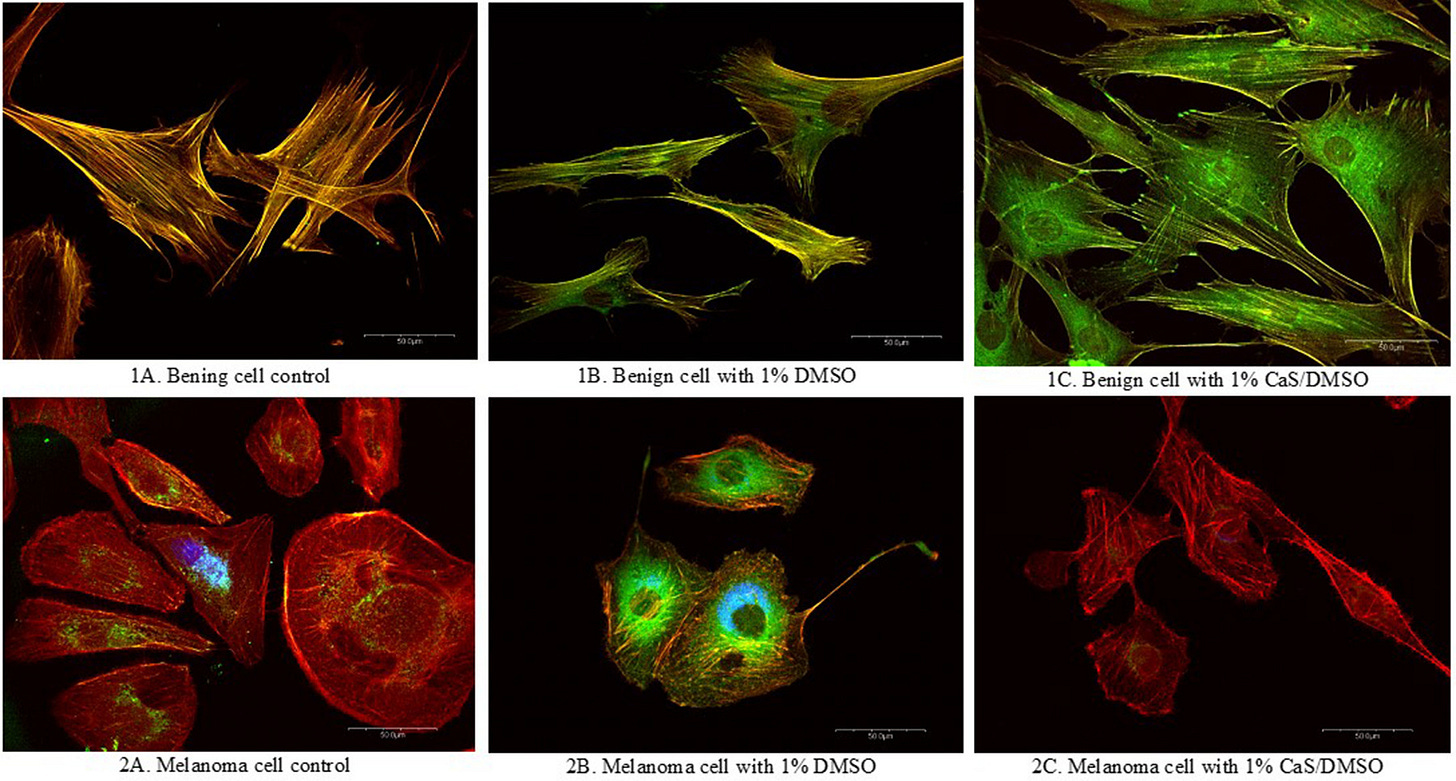
A recent study (which will be discussed later in the article) found that 1% DMSO significantly altered the cytoskeleton of melanoma cells but not normal cells:
DMSO in turn, has been hypothesized to induce differentiation through changing the abnormal cytoskeleton of cancer cells. Other data has also linked DMSO’s differentiating properties to cytoskeletal changes such as:
•An early study found that over four days, DMSO caused a progressive reorganization to melanoma cytoskeletons, which differentiated them and stopped their growth.
•Cytochalasin B disrupts the cytoskeleton and prevents DMSO from differentiating erythroleukemic cells.
•Tumor cells in culture typically grow chaotically, unlike orderly normal cells. Adding 1%–2% DMSO to the culture was found to dramatically reduce this disarray within 3 days, forming organized monolayers resembling noncancerous fibroblasts—a change which may be due to a normalized cytoskeleton.
Note: this study used raman spectroscopy to analyze DMSO induced AML differentiation
DMSO also changes other structural aspects of cancerous cells:
•DMSO was found to shift the cell membrane transition temperature from 33.0° to 36.8° (making it more likely to be in a gel-like state), and this shift appeared to correlate with the differentiation of leukemic cells. A follow-up study found other AML differentiating agents also shared this property.
•A 1969 study found (via electronmicroscopy) that DMSO transformed the thick (gel) quality throughout its cytoplasm and its structures to a homogenous fluid (sol) state. Likewise, in an early study, he noted that DMSO could melt away this fibrous barrier and that many cancer drugs mixed in DMSO (e.g., vinblastine) then cause the structures of cancerous cells to switch to becoming normal (albeit benignly overgrown).
•When erythroleukemia was exposed to DMSO, its cytoplasm became more 0.18 acidic, and its water volume rapidly shrank (12% after 15 minutes and 23% after nine hours).
•DMSO differentiating AML cells significantly decreased their viscosity1,2 and erythroleukemic cells’ negative surface charge and electrophoreic mobility1,2 (attributed to a loss of saliac acid residues).
•To assess if the differentiating effect of DMSO was mediated through changes in the cell membrane, the lipid content of the membranes of two different cancer cell lines was analyzed before and after DMSO exposure. From this, it was determined that DMSO increased the negatively charged phospholipid content and reduced the neutral lipid content (which increases membrane fluidity). Since more external negative charges improve a cell’s zeta potential, and increased membrane fluidity allows more phospholipids to be exposed to the water surrounding a cell, all of this suggests DMSO may enhance the zeta potential of cancer cells (an effect DMSO also has on regular cells).
Note: this study also analyzed the membrane lipid changes resulting from DMSO differentiation.
Collectively, many of these studies touch upon a longstanding observation that the transition to cancer is in part due to the electrical charges and the state of the water within the cells (e.g., it should be in an energy generating liquid crystalline state—something raising the membrane transition temperature promotes), which is a topic I have written more about here.
Note: these changes and cancer formation are also often associated with a loss of cellular energy (due to mitochondrial dysfunction). A few studies have shown that DMSO increases mitochondrial energy production and allows the mitochondria to continue producing energy after their function has been compromised.1,2,3
Polar Solvents
There is also some evidence that DMSO’s anticancer properties are a result of it being a polar solvent as:
•Several research teams have found that polar solvents inhibit the growth of human tumors being grafted onto mice, and some polar compounds can trigger cancer differentiation.
•Polar solvents such as DMSO caused disordered and tightly packed cancer cells to rearrange them themselves into an ordered parallel orientation like that seen in non-cancerous tissues (which was corroborated by a US government report from Sloan-Kettering that also found DMSO changed the surface proteins of cancer cells and caused them to be less tightly packed together and to have a slower growth rate).
•Other polar solvents have been found to induce differentiation (e.g., see this study and this study)
•DMSO’s ability to increase immune recognition of certain cancers may be due to its changing the exposed antigens or receptors on the cell membrane surface.
•Polar solvents allow chemotherapy drugs to penetrate cells they otherwise cannot enter (and likewise to pass through the blood-brain barrier so that otherwise unreachable brain cancers can be exposed to chemotherapy). This is important because often dangerously high doses of the chemotherapy have to be used in these circumstances to ensure some of it can reach the brain.
Pleomorphism
One of the forgotten schools of medicine is that microorganisms can assume different shapes (morphologies) and that particular morphologies can be highly detrimental to health. For example, previous pioneers of forgotten alternative cancer therapies (e.g., Rife and Naessens) believed these hard to detect organisms caused types of cancers, and as I showed in this article, they are linked to many autoimmune conditions.
A 1967 Russian study tested cancer patients for pleomorphic bacteria. While difficult to culture, pleomorphic bacteria were eventually isolated from the blood of some of them, along with being in the blood of some of those who had been around those who had recently died from a prolonged cancer:
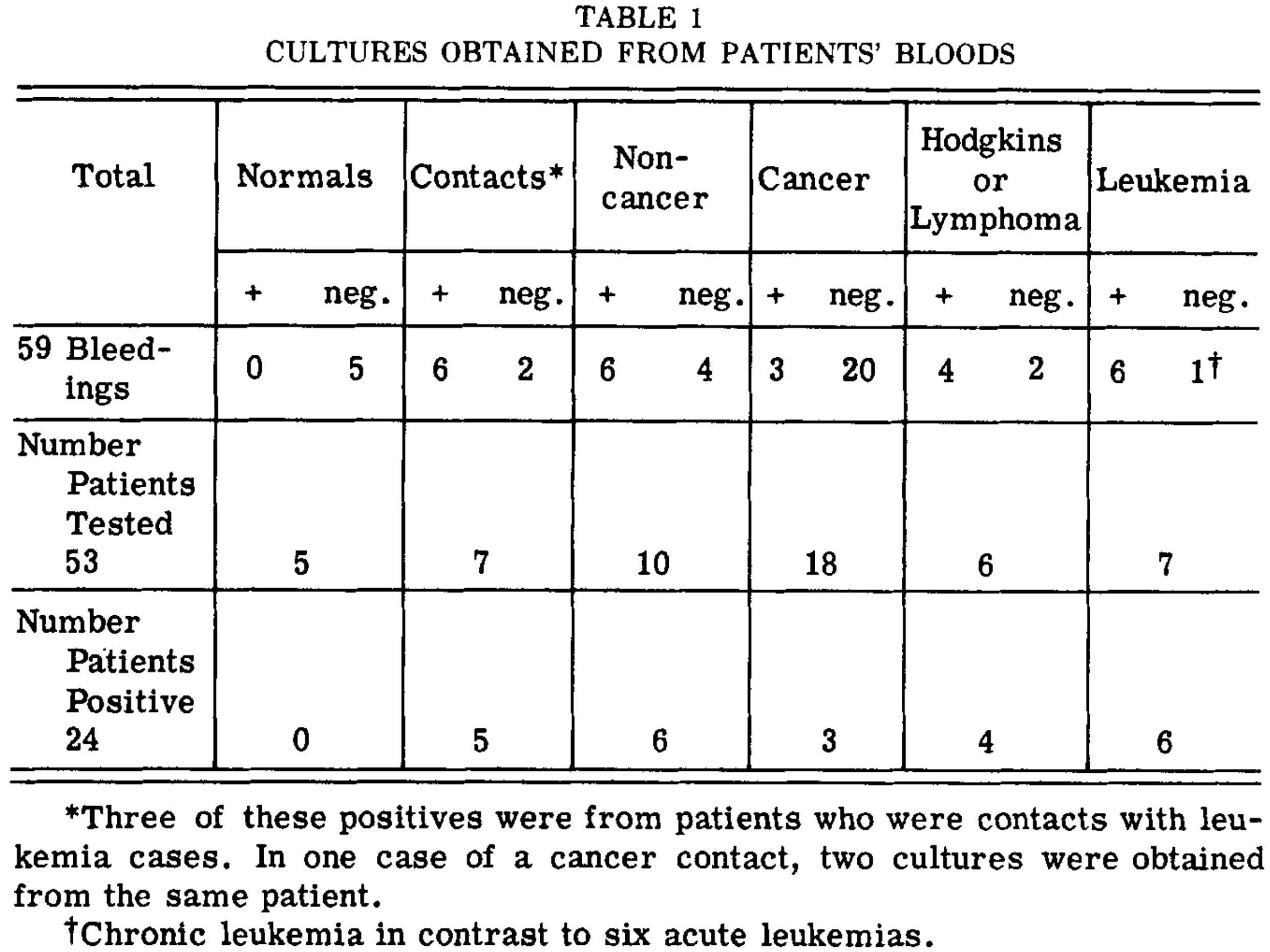
Likewise, 17 tumors were directly sampled, of which 16 yielded cultural specimens, with the negative coming from a granulomatous nodule. Additionally, one tumor had to be sampled twice as the initial specimen did not produce the bacteria. Finally, in some cases, the organisms were found directly within sampled cells.
Note: the morphology of the bacteria is extensively described in the paper, but essentially matches what many other pleomorphic researchers have found over the years.
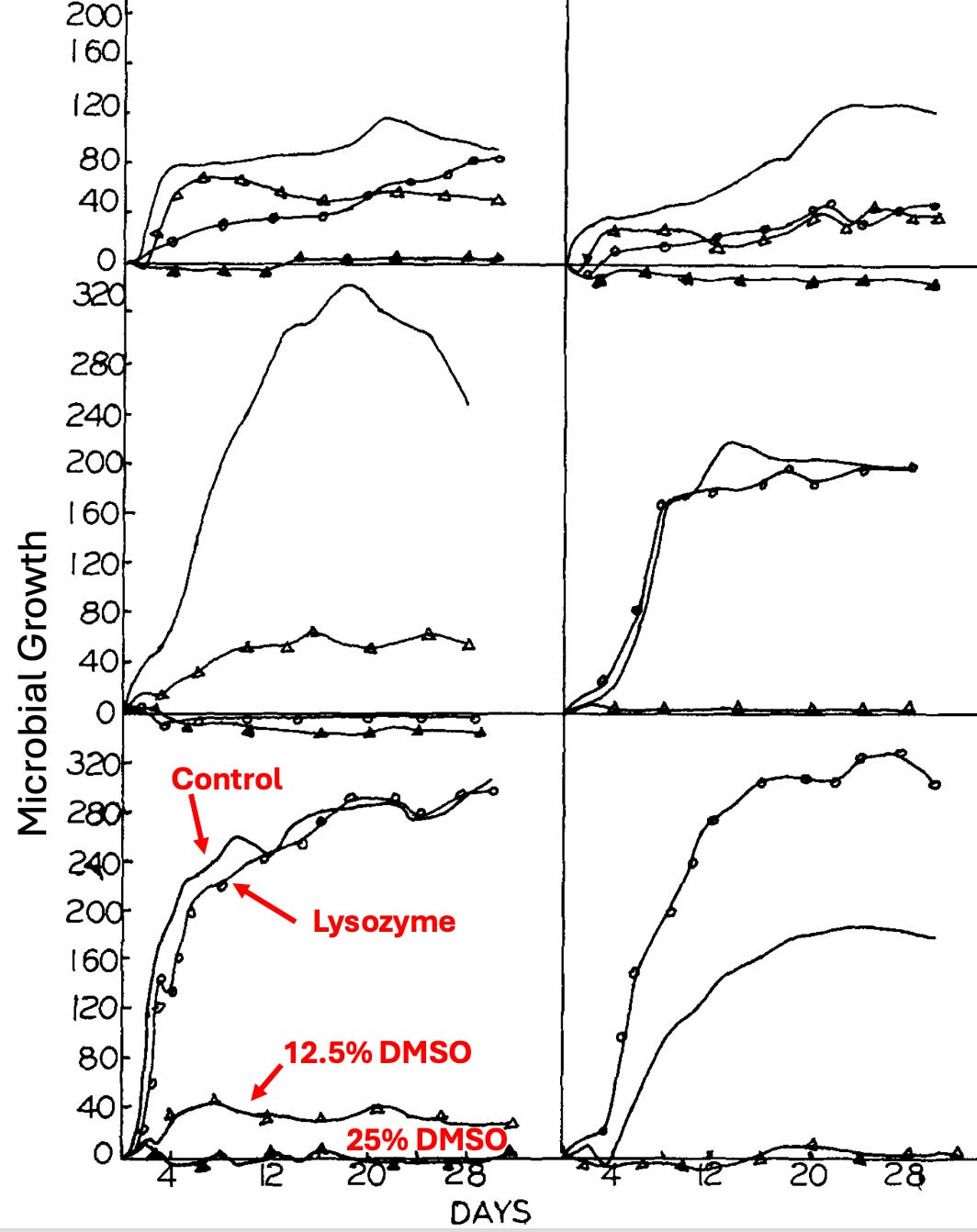
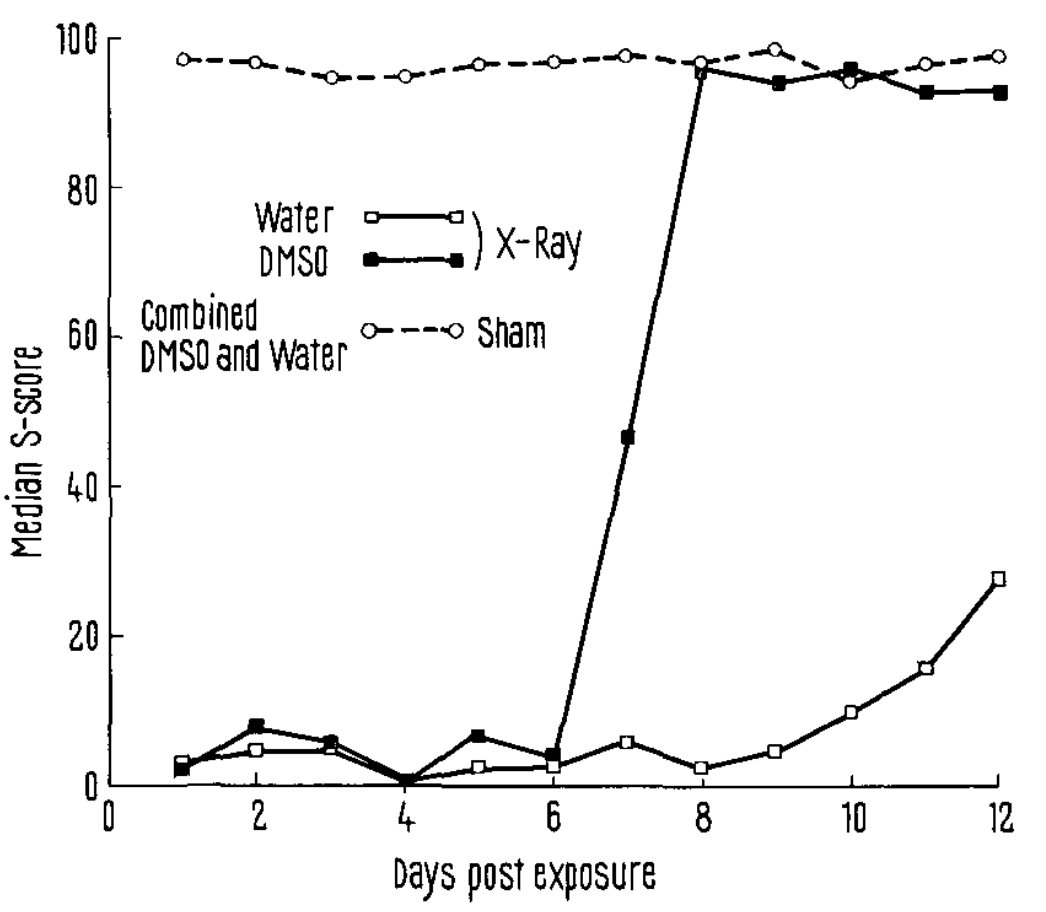
They tested three different agents on the bacteria: ethambutol (an antibiotic), lysozyme (an enzyme in many mucosal secretions protecting the body from invading organisms), and DMSO. They found that lysozyme did a bit, but DMSO did much more.
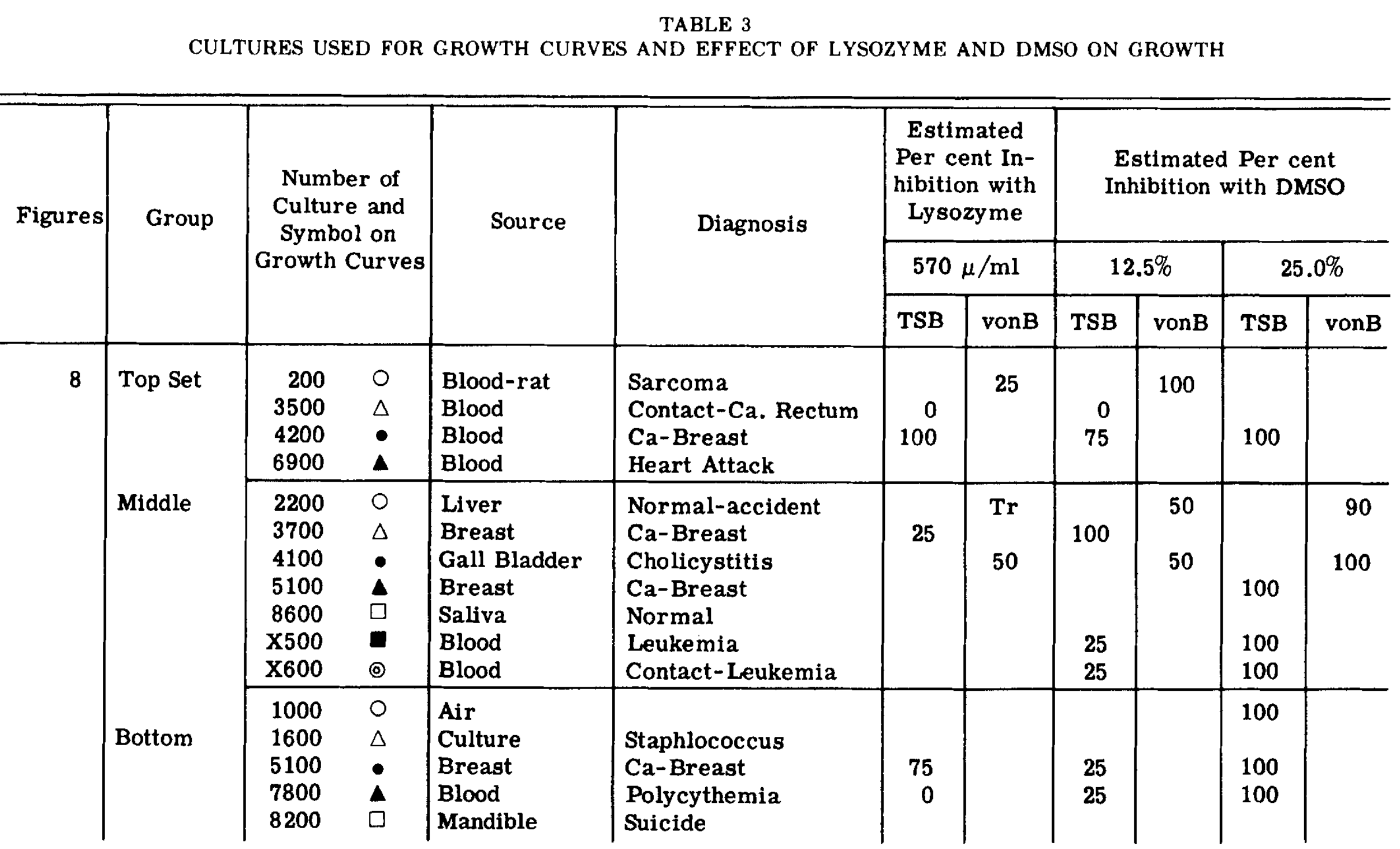
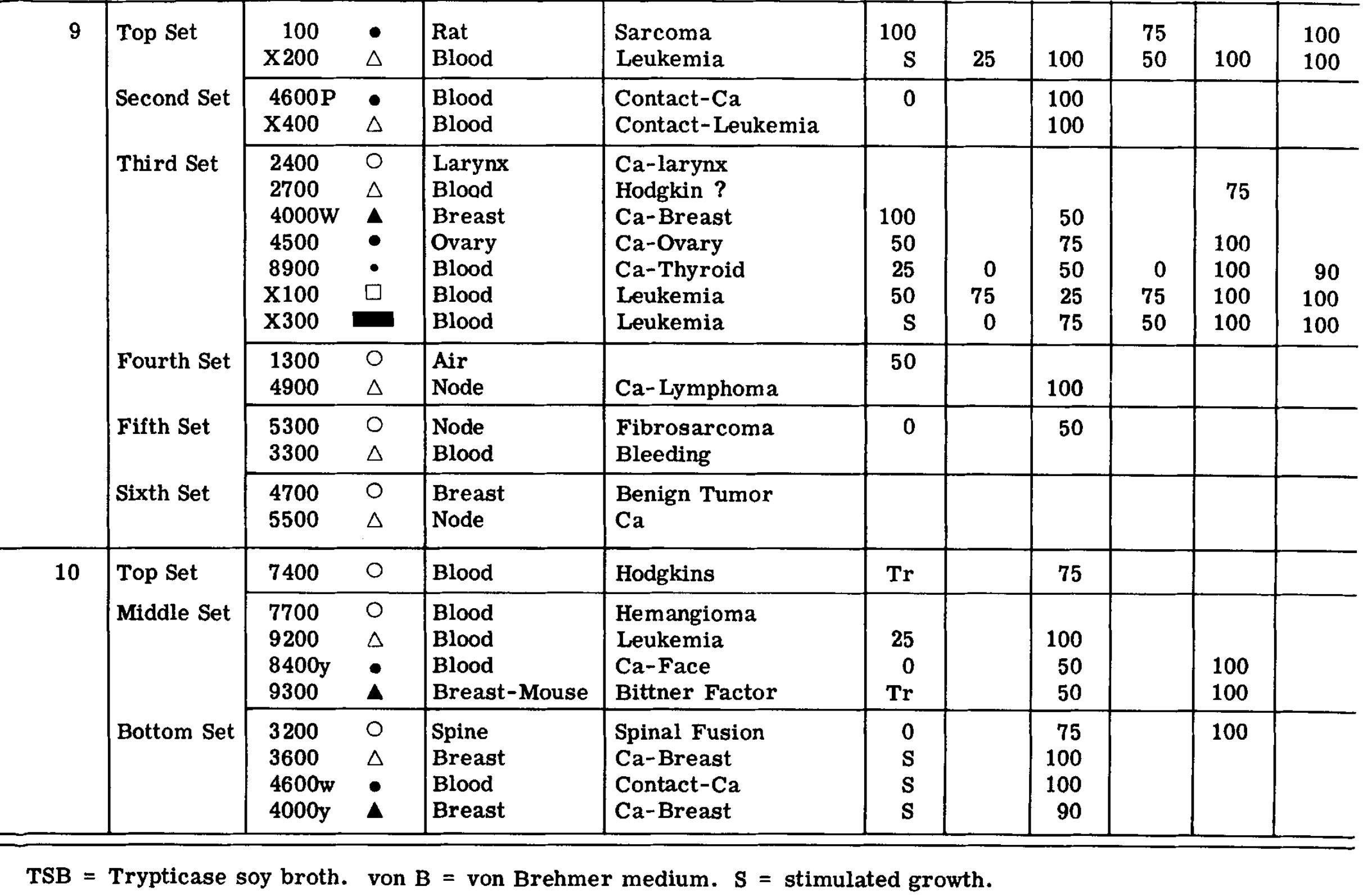
They also provided a series of growth curves that were illustrative of the effects of DMSO (one of which I annotated so you can identify what each symbol represents).
Note: when DMSO was added to fresh leukemic blood samples, it completely inhibited the dancing motion of particles free in the blood or attached to the periphery of the crenated red blood cells (another common pleomorphic observation), but did not damage the red blood cells at all.
Given that these microorganisms may induce cancerous changes, DMSO’s ability to eliminate them (as small bacteria without cell walls are the most sensitive to DMSO) could also potentially explain its differentiating properties. Likewise, its ability to eliminate them may explain why DMSO effectively treats so many autoimmune disorders.
Cancer Growth Inhibition
When DMSO differentiated cancer cells, it also frequently observed to slow their growth in cultures or implanted animals (e.g., by 62.6% in ovarian cancer cells after 5 days). In turn, this phenomenon has been observed in various cancers, including AML,1,2,3, breast cancer1 (doing so more effectively than thalidomide), Burkitt’s lymphoma1,2 CML1 colon cancer,1,2 erythroleukemia,1 intestinal cancer,1,2 liver,1,2,3 lung cancer,1,2,3 melanoma,1,2,3,4,5,6 nasopharyngeal,1 potato tumors,1 rectal cancer,1 ovarian cancer,1,2,3 prostate cancer,1,2,3,4 (and to eliminate its resistance to hormone suppression), sarcomas1.
In addition to the changes identified in the previous section, a few others have also been linked to DMSO’s ability to reduce cancer proliferation such as DMSO:
•Reducing c-myc, and ras1,2 by up to 80-90% (genes which are commonly linked to uncontrolled cancer growth), telomerase activity (which cancers need to divide indefinitely), AP-1 (a protein linked to the spread of cancer and a target of anticancer research.
•Upregulating HLJ1 (a tumor suppressing protein1,2,3), transforming mutated p53 (another important tumor suppressor protein) to one which regains functionality, and causing an immortal cell line to stop and synchronize its uncontrolled growth by making it regain contact inhibition and no longer grow when pressed against another cell)
Note: rapamycin enhanced DMSO’s ability to arrest AML’s growth, while dexamethasone inhibited erythroleukemia.
Additionally, when DMSO differentiates cancer cells, it often induces programmed cell death (apoptosis) in them. In turn, DMSO has also been repeatedly shown to augment apoptosis in:
•In differentiated AML cancer cells.1
•EL-4 lymphoma cells (via caspase-9).1
•Histiocytic lymphoma1,2,3,4 (despite their expression of the anti-apoptotic Bcl-2 protein), which was partially attributed to its enhancing mitochondrial membrane depolarization and the activation of a yet unidentified tyrosine kinase.
•Thymic lymphoma by decreasing c-myc expression which then decreased ornithine decarboxylase (ODC) activity.
Note: another drug (an FDA-approved cancer therapy) also decreases ODC activity, inhibiting growth but not triggering apoptosis.
•Cancer like macrophages1 (by reducing their CSF-1R receptor levels).
•Human skin cells (keratinocytes) transformed by the cancer causing virus SV-40 (with 2.5% DMSO) but did not do so for normal keratinocytes.1
Note: one study found Caspase 9, (associated with the intrinsic pathway) showed no significant activation following DMSO, indicating that DMSO induces apoptosis via the extrinsic pathway.
Dose-Dependency
Many studies also show DMSO’s cancer inhibiting properties happen in a dose-dependent fashion. For example:
•DMSO differentiated melanoma cells and inhibited their growth in a dose-dependent manner (e.g., 0.5% DMSO reduced it by 31.4%, while 2.0% reduced it by 88.94%) and if at least 1.5% DMSO was used, it permanently differentiated melanoma and slowed its growth
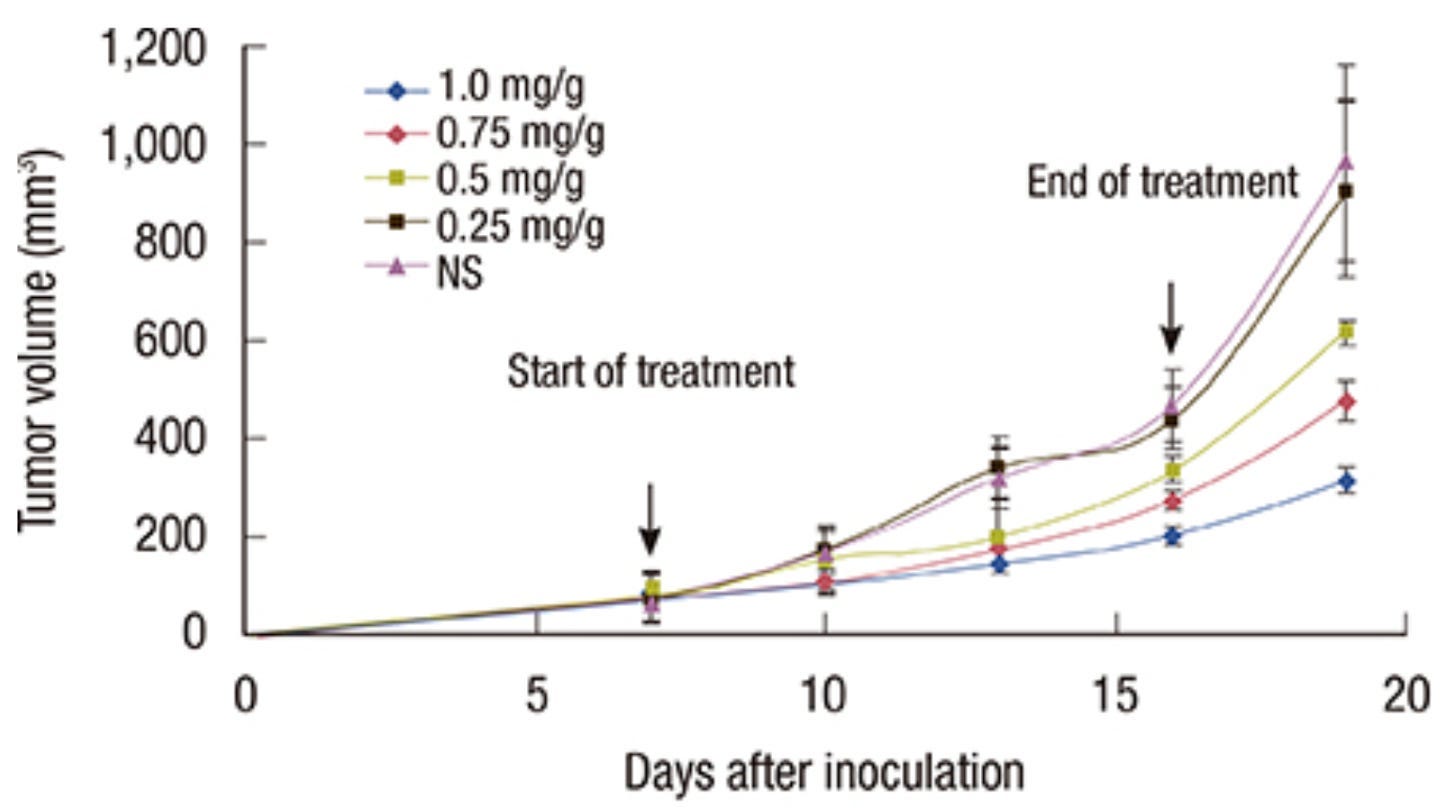
•In a 2014 study, breast cancer cells were implanted into mice, and then once tumors had grown in the mice, DMSO or saline (NS) were injected into the mice, where DMSO alone was shown to inhibit cancer growth in a dose-dependent manner.
•A 2019 study showed that DMSO decreased the viability of breast and lung cancer cells in a dose-dependent fashion.
•In a 2020 study, researchers found DMSO suppressed the proliferation (up to 69%) of erythroleukemia, AML, liver, and breast cancer (e.g., 5% DMSO downregulated CDK2 and cyclin A). This inhibitory effect was first observed at a 2% DMSO concentration and intensified with increasing doses, reaching a maximum at 10%."
•A 2020 study found 2% (but not 1%) DMSO inhibited the growth of human cancer cells, that this effect increased as the dose was raised to 5-6% and that it also damaged the cancer cells and down regulated CDK2 and cyclin A (both of which are needed for cancer growth).
Note: while DMSO typically causes apoptosis in Burkitt’s lymphoma cells, at a narrow range (1-2%), it suppressed it—something I did not see for any other cancer. Likewise, while a few studies indicated that DMSO increased cancer cells' viability or metastatic potential, almost all of the studies I found showed it had an inhibitory effect.
•A 1967 study repeatedly found that 2% DMSO effectively killed most leukemic white blood cells and that normal (healthy) white blood cells had a much greater tolerance to DMSO, particularly when only exposed to DMSO for a day or less.
•A 2020 study found that DMSO significantly inhibited the proliferation of 4 cancer cell lines and was much more potent than alcohol or methanol.
•Most importantly, a 2021 study found that very low concentrations of DMSO (including the lowest tested, 0.0008%) had significant effects on the biochemical activity of cancer cells, potentially explaining why small doses of DMSO (which spread throughout the body) can affect cancers.
Animal Studies
Many other animal studies also show that DMSO treats cancer in animals:
•A 1989 study of rats with aggressive (implanted) prostate cancers found that 2.5% oral DMSO significantly slowed the cancer’s growth.
•A 1967 study induced breast cancers in mice and found that drinking DMSO caused a small reduction in their rate of occurrence and prevented some of weight loss caused by the cancers.
•A 2008 MRI study evaluated the microvasculature of mice with implanted tumors before and after a week course of DMSO. It found DMSO greatly reduced cancer vascular permeability, which is potentially significant for cancer management as leaky blood vessels can support rapid irregular growth or metastasis and can compress surrounding tissues or cause inflammation and sometimes interfere with the delivery of chemotherapy to those cells.
Note: many holistic schools of medicine have concluded cancers arise from poor blood flow to a tissue or poor lymphatic drainage from it. Given DMSO’s remarkable ability to improve circulation, it is highly possible that this contributes to its ability to prevent cancer.
•A 2011 study found that in mice with experimentally induced Dalton’s lymphoma, injected DMSO was shown to regress their tumors and upregulate TNFα and p53 in lymphoma cells, which impaired their metabolic pathways and triggered an apoptotic pathway (whereas normal white blood cells were unaffected).
Additionally, in hamsters, DMSO has been shown to prevent 9,10-dimethyl-1,2-benzanthracene and 3-methylcholanthrene from creating cancers, and two other studies1,2 found that DMSO partially prevented methylcholanthrene from causing skin cancer in mice (particularly malignant cancers).
Note: a 1967 rabbit study found that DMSO does not increase the spread or growth rate of tumor cells implanted into the peritoneal cavity (thereby indicating that topical applications of that manner are safe).
Human Studies
Finally, a few studies have also shown that DMSO alone can significantly improve cancer outcomes:
•A 1992 study conducted by an Iraqi researcher (who’d found DMSO cured a variety of challenging gastrointestinal conditions) conducted a controlled trial of 198 patients who’d had surgery for colon cancer (in the sigmoid) that had spread into the local lymph nodes, and found that the long term administration of oral DMSO after the electrosurgery significantly improved their 5 year survival.
•That researcher also conducted a 1992 controlled trial of 228 patients who’d just had an uneventful surgery to remove two-thirds of their stomachs (due to stomach cancer). Daily oral DMSO significantly increased their survival rates in the 160 patients who could be evaluated at 5 years.
•A 1999 trial of 25 patients found intravesical DMSO treated bladder cancer and that if a one biomarker was then negative following therapy, they were much less likely to have a recurrence.
Immune Activation
Since the body relies upon the immune system to eliminate cancers, many natural and conventional approaches to cancer have tried to support that. Fortunately, while DMSO is highly effective at reducing autoimmunity and inflammation within the body, it does not impair the immune system's response to cancer, and if anything enhances it.
A key reason for this is that DMSO achieves what many conventional cancer immunotherapies aim to do—prevent cancer from evading the immune system, thereby allowing it to be targeted and eliminated.
The earliest application of this was from George Moore, a renowned cancer researcher who had investigated treatments for large oral, genital and rectal HPV-related warts, such as condylomata acuminata (which often required repeated, painful interventions like surgical excision, cautery, or cryotherapy to reduce their size) involving topical dinitrochlorobenzene to solicit a local immune response to the warts. In his 1978 JAMA paper “Condyloma A New Epidemic,” he reported he had successfully treated 22 of 23 patients who had podophyllum resistant warts, while in 1975 he reported to the Lancet::
We have been using dinitrochlorobenzene (D.N.C.B.) for the treatment of cutaneous metastases from various malignancies such as breast melanoma. In such instances penetration of the skin by the antigen is important. The addition of dimethylsulphoxide to D.N.C.B., in a water-soluble base, and the use of an occlusive dressing have been helpful. Caution must be used since some local reactions may be severe especially in the axilla or in skin folds. Solid tumour metastasis can be completely destroyed. The search for and evaluation of antigenic agents for topical immunotherapy must be expanded.
Additionally, an author who corresponded with Moore shared that Moore began treating these warts because he disagreed with the "barbaric treatments" used for them, and that his DMSO D.N.C.B. treatment (which he characterized as a cancer vaccine) was so effective he was rapidly deluged with male patients seeking him out (which he described in language that emphasized the point but is no longer appropriate to put into writing).
Note: as I showed here, topical DMSO can be effective for a variety of skin lesions including warts and cancer.
Much later, a pivotal 2016 study proved it was possible to use DMSO to make a “vaccine against cancer.” It exposed liver cancer cells to 2% DMSO, which temporarily slowed their growth and permanently changed their gene expression. These treated cells were then injected into mice and, unlike untreated cancer cells, did not form tumors. Crucially, the DMSO-treated cells induced an anti-tumor immunity that allowed the mice to completely eliminate untreated liver cancer cells. This treatment also conferred a partial immunity to the mice against certain other cancers, specifically B16-F10 melanoma cells. The study found that DMSO treatment increased the activation of cancer-eliminating immune cells (CD4+, CD8+ T cells, and NK cells). Mice lacking a functional immune system did not respond to this therapy, confirming the importance of the immune response.
Note: given the myriad of issues with the vaccines (e.g., many toxic and autoimmune or microstroke provoking substances typically being added in), I hesitate to use the term vaccine here. However, that does characterize what is happening here (and does not require the toxic substances typically found in vaccines).
In turn, numerous studies have shown that DMSO stops cancer cells from being able to evade the immune system as:
•DMSO increased the differentiation of lung cancer cells and increased the surface expression of H-2K and H-2D antigens at least 100-fold (which aids the immune system in being able to target the cancer). In a follow-up study, the authors showed this H-2 change greatly increased their susceptibility to being eliminated by the immune system (via H-2-restricted immune lysis). Another study found that DMSO increased the expression of H-2 antigens in T-cell lymphoma and increased their sensitivity to immune cells.
•DMSO significantly decreased the metastatic potential of mouse lung cancer cells, which the authors attributed to its increasing the expression of class I antigens (which the immune system uses to target cancerous cells). However, the two other agents that increased class I antigen expression did not reduce mice metastasis
•DMSO increased the ability of the spleen (likely its macrophages) to identify and eliminate cancerous cells.
•DMSO induced surface antigen expression in melanoma cells.
Likewise, DMSO was also shown to increase anticancer immune cells. For example, in a 2014 study, DMSO increased the presence of anti-tumor macrophages and decreased pro-tumor macrophages. In a 1975 study, DMSO potentiated the immune response to specific cellular antigens by increasing T-cell MIF production and possibly also by exposing antigens to T-cells.
Finally, when DMSO differentiated AML cancers into immune cells, those cells were able to mount an effective immune response (which could potentially be helpful in leukemia). Specifically, those cells (which often become neutrophils or macrophages):
•Could effectively mount an immune response (whereas other differentiating agents produced immune cells that did not).
•Were better able to bind carbohydrate antigens (which macrophages need to consume foreign invaders).
•Had a high responsiveness to immune receptors (e.g., TLR2 and TLR4) that trigger an immune response to invading pathogens.
Amyloidosis and Multiple Myeloma
Multiple myeloma (MM) is a type of blood cancer characterized by the uncontrolled growth of malignant plasma cells in the bone marrow, which produce abnormal proteins that can overwhelm the body (which sometimes creates enough issues to need to be removed with plasmapheresis blood filtration).
As I showed in this article, there are over 40 studies demonstrating that DMSO prevents amyloid proteins from clumping together and instead eliminates their deposits from the body (e.g., one study found this after testing 125 Bence Jones proteins)—which represents a massive paradigm shift for this (currently incurable) disease. Since amyloids are seen in 10-15% of cases of MM, case reports have gradually emerged of it helping those MM patients:
•A 1981 case report found (with imaging) that DMSO was an effective treatment for soft tissue MM amyloidosis.
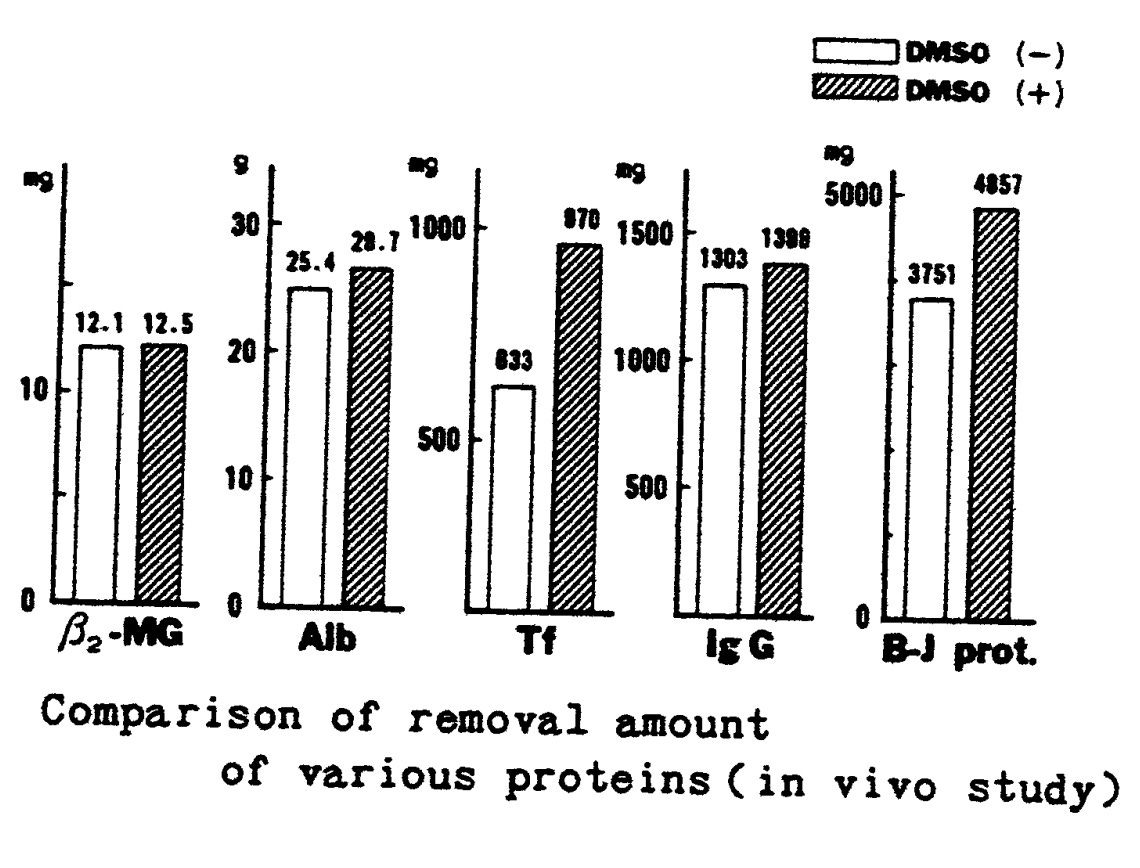
•In a 1987 case report, Japanese researchers used plasma exchange to remove harmful proteins from a patient with Bence-Jones type of MM and one with fulminant hepatitis. It found that DMSO significantly increased the filtration of the unwanted proteins, did not damage the filtration membrane, and caused no side effects (e.g., hemolysis, shock, fever, or liver damage)
•In 1984, a patient with Bence-Jones MM treated their carpal tunnel syndrome (caused by amyloidosis) with a topical DMSO ointment.
•In 2009, an MM patient with pulmonary amyloidosis was successfully treated with DMSO.
Finally, a 2000 case report discussed using DMSO to cure, rather than just mitigate the symptoms of MM amyloidosis. In a patient with previously undiagnosed MM (which had caused significant issues in the rectal submucosal and lips, along with creating a mass in the submandibular region). He was put on long-term combination chemotherapy (vincristine, doxorubicin, and dexamethasone), IFN-alpha and oral DMSO which resulted in a marked improvement of his amyloidosis symptoms as well as a significant improvement of his MM (e.g., a decrease in the levels of plasma cells in bone marrow and of M-protein and immunoglobulin G in serum).
Cancer Pain
In addition to being potentially lethal, cancer (and cancer treatments) are accompanied by many other debilitating symptoms, one of which is pain—something so severe the general restrictions on opioids are typically lifted for it (e.g., fentanyl is often used to treat advanced cancer pain—but in 10-20% of patients their pain is severe enough that even potent opioids can’t address it).
Fortunately, since DMSO has a rather unique mechanism of treating pain, it is often able to treat a wide range of challenging pain conditions nothing else works on (e.g., I’ve now had hundreds of readers share life-changing pain improvements with me from topical DMSO nothing else they’d tried had ever worked on). As such, many over the years have found it provided incredible relief for metastatic cancer pain.
One of the most well known examples was Otis Bowen MD (a popular second term Indiana governor) who “illegally” used topical DMSO to treat his wife’s pain from terminal multiple myeloma and then publicly denounced the FDA’s absurd embargo on it at the AMA’s 1981 national meeting. Remarkably, a few years later, Bowen became Reagan’s Secretary of Health and Human Services. Still, even then, with this highly ethical doctor at the helm of the HSS, DMSO was unable to overcome the FDA’s prohibition of it—which helps to highlight the incredible challenge RFK Jr. is now facing (but gradually surmounting).
Likewise, a few studies have shown that DMSO can treat this pain:
•A 1967 study gave two older patients with cancer pain DMSO, one of whom had an excellent response to treatment and one who had a good response.
•A 1967 study found that of 7 patients with metastatic cancer pain, DMSO gave 2 a full remission and 2 a partial remission.
•A 2011 trial gave DMSO and NaHCO₃ to 26 patients with advanced cancers who were experiencing significant pain (even with all the available treatment options). This significantly reduced their pain (to the point that all were able to stop using morphine) and greatly improved their quality of life (e.g., chemotherapy symptoms).
Note: this paper further discusses DMSO’s ability to treat intractable cancer pain. It highlights that this may be due to DMSO’s ability to address membrane hyper-excitability (e.g., through suppressing NMDA and AMPA induced ion fluxes—which are linked to central pain sensitization and may explain why DMSO effectively treats complex regional pain syndrome).
Protecting Against Cancer Therapies
One of the primary values of DMSO is its ability to protect cells and tissue from a variety of lethal exposures (e.g., burns, freezing, blood loss, asphyxiation, UV light, and soundwaves) and to greatly accelerate healing from injuries (e.g., sprains or burns).
Since many of the complications from cancer arise from the treatments for it, DMSO hence has value as an adjunctive cancer therapy—particularly since DMSO does not protect cancerous cells from cancer treatments (and rather often makes them more potent). For example:
•One study found that DMSO protected human hematopoietic stem cells from radiation, but did not provide any protection to AML cells.
•Rather than protect them, DMSO triggered cell death in erythroleukemic cells that had been exposed to radiation.
•DMSO caused the AML cells it differentiated to become sensitive to radiation.
Conversely, DMSO has also been shown to protect non-cancerous cells deliberately sensitized to radiation.
Note: as I showed here, DMSO is also very effective for healing from surgery, and as such can often help the recovery from cancer. For example, in dogs that required a unilateral mastectomy, giving IV DMSO 15 minutes prior to the surgery’s conclusion reduced the post surgical inflammation.
Radiation Therapy
In addition to protecting cells from other sources of injury, as early as 1961, DMSO was also recognized to protect cells and tissues from radiation exposure.
Note: by 1967, it was well recognized that DMSO (even just applied topically to the skin) strongly protected against lethal x-rays and did so in a manner that was much more effective than many other available radioprotective agents.
Since cancer treatment frequently requires radiation therapy (which frequently causes a variety of complications that lack established treatments) and the evidence is quite strong for DMSO’s ability to address those complications (especially if given prior to radiation but also after radiation), I believe this is one of the areas where DMSO provides greatest benefit in the treatment of cancer.
Note: I have mixed feelings on radiation therapy as while sometimes necessary (particularly if robust alternative treatments are not available), it frequently creates significant side effects (ie. fibrosis of the tissues) that can cause issues for years. I also believe our focus on radiation therapy ultimately resulted from mining magnate James Douglas devising a way to produce cheap radium and then giving a large donation (along with subsequent donations) to America’s premier cancer institute to create a program for developing radiation therapy that spread across the world.
How DMSO Treats Radiation Injuries
Radiation has a variety of mechanisms through which it damages tissue such as:
•Directly breaking chemical bonds (which damages DNA, RNA and proteins) and damaging mitochondrial membranes (which are particularly sensitive to radiation),
•Indirectly creating reactive oxygen species and free radicals (which damage a variety of cellular components).
•Triggering an immune response (e.g., by releasing IL-1, IL-6, TNF-α, and TGF-β), which often leads to chronic inflammation, fibrosis and adhesions.
•Putting cells into senescence (a state of permanent growth arrest).
•Causing normal cells in the vicinity of the affected ones to die as well (e.g., when only 1% of cells are exposed to radiation, approximately 30% of cells will exhibit similar toxic effects from the radiation), a fascinating phenomenon known as the bystander effect which I believe is mediated through mitogenic radiation emissions.
DMSO in turn, counteracts each of these effects. For example, in previous articles, I highlighted the body of evidence that DMSO:
•Treats (and prevents) fibrosis in many different organs.
•Eliminates adhesions.
•Reduces the key inflammatory cytokines (also discussed here).
•Rescues senescent cells trapped in the cell danger response (also discussed here).
•Neutralize free radicals (e.g., through scavenging charged ions and forming protective DMSO radicals), prevent radiation from creating harmful free radicals (also shown in this study) and prevent free radicals (or reactive oxygen species) from damaging DNA. (also shown in this, this, this, and this study).
Note: one study found this protection only occurred for cells in the liquid state (but not frozen ones), while another found DMSO could also protect cells if it was given up to 10 days post irradiation.
•To prevent the bystander effect from damaging non-irradiated cells (possibly through preventing the formation of free long lasting free radicals).
•Regrow lost hair (a common complication of radiation therapy).
•Reduces chromosome damage from radiation.
•Accelerates the healing of tissues after injuries (e.g. from radiation).
This highlights that DMSO’s protective effect is selective, primarily benefiting healthy tissues while maintaining a reduced impact on cancerous growth.
AML cells differentiated by DMSO were initially more sensitive to radiation, but after 3-5 days (once they had become more differentiated), they became less sensitive to it.
Further studies are warranted to explore this dynamic in greater detail, particularly to determine how DMSO can be strategically applied to balance the protection of healthy tissues and the effective targeting of cancer cells.
Cell Studies
Studies have repeatedly shown that DMSO protects cells (particularly when given prophylactically) from being damaged by (often otherwise fatal) radiation (e.g., DMSO was shown to protect skin cells from dying after exposure to gamma radiation and make hamster cells four times as resistant to radiation).
Note: in one detailed study, when 3% DMSO was given prior to irradiation, the protective effect increased (up to when 15% DMSO was used).
DMSO also:
•Protected the enzymes catalase and lactic acid dehydrogenase from being inactivated by x-rays (with DMSO concentrations as low as 0.28%).
Note: the protective effect of DMSO on enzymatic activity has also been observed in some of the earliest studies on radiation therapy (e.g., one where it protected catalyze), making it one of the earliest breakthroughs in understanding how DMSO works on a biochemical level.
•Protects lymphocytes and macrophages from DNA damage and death (along with protecting chromatin from gamma rays).
•Protects human kidney cells from freezing and radiation damage, and makes warmer cells (e.g., those at body temperature) as resistant to radiation damage as frozen ones.
•Protects certain bacteria from x-ray exposure (also shown in this and this study) while making another species spores’ more sensitive.
Most recently, a 2024 study found skin cells (modified to become pluripotent stem cells) found giving DMSO prior to irradiation protected the cells from the genetic damage radiation would otherwise cause.
Lastly, this study (which used deuterated DMSO) discussed the chemical changes DMSO and water undergo when they absorb radiation.
Plant Studies
Pre-treatment (but not post-treatment) DMSO prevented 52% of the radiation induced chromosome breaks. A subsequent study found similar results for barley, wheat, and triticale seeds, along with DMSO also reducing seedling injury and death. Additionally, another plant study found that ultraviolet radiation and DMSO together increased the productivity of an antimalarial compound.
Animal Studies
These animal studies provide clear evidence of the versatility of DMSO in protecting organisms from radiation damage.
A 1967 study found that while only 9% of mice survived after a lethal radiation exposure, when they were given intraperitoneal DMSO, most survived (54% of those receiving 50% DMSO, 67% of those receiving 75% DMSO, and 63% of those receiving 90% DMSO).
When DMSO was given to rats within an hour of an otherwise lethal radiation dose, 70% instead survived. Applying DMSO to newborn rat skin protected them from damage from x-ray exposure.
DMSO was found to protect newts from lethal x-ray and gamma ray exposures (along with preventing organ and skin damage).
In fruit flies, DMSO significantly reduced x-ray mortality and mutations of their sperm.
DMSO protected Golden hamster embryos from gamma rays and (by accelerating DNA repair) prevented X-ray damage to hamster ovary cells.
Dipping mice tails in DMSO prior to irradiation (but not after) significantly reduced their mortality.
Mice tail bones treated with DMSO continued growing even after exposure to substantial doses of radiation.
DMSO given 8 minutes before a 1000 R exposure to the head prevented cataract formation in mouse eyes.
In mice, to prevent radiation-induced oral mucositis (e.g. ulcers) through facilitating DNA repair of the stem cells there.
In mice, it protects intestinal crypt cells from radiation (which rapidly divide and hence are significantly more sensitive to radiation). Likewise, this study also used DMSO to protect intestinal cells from radiation.
In rats, it prevents radiation induced damage (from oxidative stress) to the kidneys.
A rabbit study found that DMSO protected them from Cobalt-60 radiation (and the inflammatory response to it) without causing any negative changes to the structure of the lungs or the capillaries.
Note: another study showed DMSO also protects cells from other radioactive isotopes.A 2022 mouse study found DMSO giving DMSO prior to irradiation protected mice testicles (e.g., testicular weight and hormonal function was preserved) and fertility (e.g., spermatozoa remained alive and did not accumulate DNA damage as DMSO facilitated DNA repair).
A 2020 mice study found that DMSO to some extent prevented radiation fibrosis.
A study found that even greater protection from radiation occurred when DMSO was combined with levorin (or methylated levorin or isolevorin).
Note: the authors of that study also published a review that further discusses DMSO’s radioprotective and anticancer effects when given with those compounds.Inhaling DMSO vapor was also shown to protect mice from radiation exposure (which was also shown in this study).
In a mice study, 100% DMSO (but not 80% or any concentration lower than that) was found to increase the sensitivity of mice skin to radiation injuries, which led the authors to suspect the increased blood flow created by 100% DMSO was bringing oxygen to the tissues which could then be turned into harmful free radicals.
Topical application of 30% DMSO to the skin of 16-day-old nestling rats 20 minutes before x-ray exposure protected them against x-ray-induced damage.
A rat study found that giving them DMSO post-irradiation increased their ATP, ADP, and AMP levels (whereas no change was seen in non-irradiated rats that received DMSO), suggesting DMSO had augmented a post-radiation regenerative process.
When unpleasant radiation exposures were used to create a conditioned taste aversion to saccharin (a sweetener) in rats, giving DMSO was found to prevent that negative conditioning from occurring.
Note: this avoidance can also be transferred by injecting brain tissue of the irradiated mice into a non-irradiated one. However, if DMSO is given before irradiation, it prevents any transferability.
Human Data
Earlier in this series, I showed that DMSO has a remarkable ability to protect and heal the skin from injury, and in turn, since 1966, numerous Russian German and Japanese studies (including clinical trials) have demonstrated DMSO’s remarkable ability to protect human skin (along with its collagen and mucopolysaccharides1) from radiation.1,2,3,4,5,6,7,8,9,10,11,12,13
These include studies where:
•The irradiation was done by radioactive cobalt.
•In patients with radiation-induced skin fibrosis following telecobalt radiation therapy, DMSO significantly reduced fibrosis by decreasing collagen levels in the affected skin, leading to improved or complete resolution of clinical fibrotic signs.
•Trasylol and epsilon-aminocaproic acid were given in conjunction with DMSO to prevent a subsequent radiation injury or DMSO was used with CoQ10 to modify radiation injuries.
•It treated radiation fibrosis,1,2 radiation dermatitis, radiation injuries or other local radiation complications.
Note: while DMSO can treat radiation injuries after the fact, it works much better when given prior to radiation therapy.
DMSO has also been shown to protect other tissues. For example:
•A 1977 study where 80 patients who had developed late local radiation complications (induration, ulcers) from the treatment of breast or genital cancer (or a non-cancerous disease) received DMSO, resulting in both a high efficacy of treatment and no side effects.
A 1985 Russian study gave 22 patients with cervical cancer topical DMSO prior to internal radiation therapy done with an older device that delivered gamma rays. It found that compared to 59 controls (who only received radiation therapy), DMSO prevented the normally expected radiation burns and other toxic reactions to the treatment (e.g., in the bladder and rectum). Additionally, while it protected normal tissue, DMSO did not protect the cancerous tissue.
A 2006 study of 807 patients with cervical uterine cancer gave 10% DMSO into the bladders of 113 patients an hour before receiving weekly intracavitary irradiation therapy and to 473 patients who also received metronidazole dissolved in 100% DMSO. In those who received neither, the radiation damage to the rectum and bladder was 19.0% and 8.8%, in those who received only DMSO it was 9.5% and 7.1%, and in those who received DMSO and metronidazole it was 1.7% and 1.7%. Additionally, the study found that larger DMSO doses offered more protection.
A 1978 American study that used DMSO to treat a variety of inflammatory conditions of the urinary tract included 12 patients with longstanding radiation cystitis (e.g., from prostate cancer therapy), of whom 50% had a positive response to DMSO (3 “excellent,” 2 “good” and 1 “fair”).
Note: a 1979 Russian study also used DMSO to treat radiation cystitis while anecdotes of DMSO producing dramatic results for radiation cystitis can be read here.
•A Japanese study (by this researcher and summarized here) evaluated 22 breast and cervical cancer patients and found that DMSO protected them against radiation dermatitis (e.g., erosion, blistering, itching, and pain) while also enhancing cancer sensitivity to radiation (as the DMSO treated areas showed skin reddening and exfoliation earlier) and accelerating the regrowth of normal tissues. Additionally, they found that when DMSO was only applied to one side, the non-applied side did worse, that the hyperpigmentation which follows radiation therapy was greater in DMSO treated patients, and that only one of the 22 patients had to stop DMSO (due to having a skin eruption which may have been linked to DMSO).
•This author detailed a case of a patient with lung cancer that was treated with three months of radiation therapy but severely damaged her lungs (making her require oxygen and leaving her unsure if she’d survive—but after topical and oral DMSO, she had a rapid recovery. Likewise, he also shared a case of another woman with lung cancer who was expected to have significant lung complications from the treatment (as she required a borderline lethal dose), but took topical DMSO prior to each treatment and instead had no complications and was fully healthy three years later.
It is thus quite remarkable that all of this remains unknown. To quote the author of one of the above (2022) study:
Currently, there is no approved agent for the prevention or treatment of radiation-induced testicular injury…In summary, our findings demonstrate the radioprotective efficacy of DMSO on the male reproductive system, which warrants further studies for future application in the preservation of male fertility during conventional radiotherapy and nuclear accidents.
Note: in addition to the higher doses experienced from radiation therapy, diagnostic radiation, specifically CT scans (which expose the body to much higher radiation doses than X-rays) also pose a cancer risk—particularly since the dose of radiation with CT scans can have over a 10-fold variation. In turn, a CT scan was found to make you 17-24% more likely to develop cancer, with the risk increasing the younger you were at the time of the scan and being much higher for certain types of cancers1,2,3,4,5. with a 2009 study estimating 29,000 cancers were caused by the CT scans performed in America in 2007. As such, I try to avoid CT scans I do not feel are essential (particularly since a detailed physical exam frequently provides more actionable information) and it is my sincere hope at some point in the future, DMSO will be given in conjunction with CT scans (but unfortunately their use keeps going up and they are viewed as a highly lucrative growth market).
Chemotherapy Injuries
After shock, cells often enter a defensive state where their functions become impaired or cease, and if not addressed, the cells eventually die. In turn, many (frequently miraculous) regenerative therapies (e.g., Ultraviolet Blood Irradiation) effectively work by restoring the function of these shocked cells. DMSO excels in this regard, and throughout this series, I’ve shown how it produces almost unbelievable results by doing the same for nervous tissue (e.g., after a stroke, brain bleed or paralyzing spinal cord injury) and many of the internal organs.
Since chemotherapy and radiation shock the body, DMSO can also prevent cell death, which follows their application—but like UVBI, it does so in a manner that doesn’t protect the cancer cells (rather, it increases cancer cell elimination). As such, whenever we have patients on conventional cancer regimens, we try to put them on therapies like DMSO as we find it significantly reduces the side effects from chemotherapy (e.g., in a previous article I discussed how effective UVBI is for this).
In turn, one of the areas of the body where this loss of cellular function can most easily be observed is with the sudden onset of hair loss. Since chemotherapy is the most toxic to rapidly dividing cells (which hair has to be so it grows), rapidly hair loss is one of the most common side effects of chemotherapy and in a previous article, I provided the wealth of evidence appropriately applied DMSO is often extremely helpful for hair loss (as are more costly regenerative therapies which rescue frozen hair cells). Because of this, many doctors over the years have reported DMSO has an extraordinary ability to rapidly regrow the hair that is lost after chemotherapy.
Extravasation Injuries
Since the medical field has been extremely reluctant to consider any alternative cancer treatment that could threaten its bottom line (regardless of how much data is behind it), DMSO has essentially not been utilized in the treatment of cancer. However, there is one exception to this rule, as DMSO is able to address a challenging issue encountered with chemotherapy without threatening the existing market.
Since many chemotherapy drugs are quite toxic, they have to be administered in a tightly controlled manner. Unfortunately, in many cases however, the drug gets through the injected vein and leaks into the surrounding tissue.
Note: since extravasations are often not reported, estimates widely vary on how common they are (e.g., 0.1-6% of adults who receive chemotherapy), but one study made a compelling case that it occurs in 39% of patients.
Due to how toxic some of the chemotherapy drugs are (particularly the anthracyclines), when that leakage occurs and the drugs concentrate in one area it can often cause significant damage to the surrounding tissues, and lead to ulceration or necrosis (tissue death). Since the existing treatments don’t always give satisfactory results and DMSO is extremely effective at healing a wide range of tissue injuries, it eventually got used as a treatment for these injuries and quickly caught on.
Note: currently there is only one drug (dexrazoxane, which is a chelating agent derived from EDTA) that is approved for the treatment of anthracycline extravasation. Despite this, a 2014 review on dexrazoxane noted, “the non-invasive combination of DMSO and cooling is the most commonly described therapy [in the scientific literature], particularly in small anthracycline extravasations” and a 2005 review recommended using 99% DMSO to treat them (as did a 1993 article).
Because of this, several animal and human studies (typically with doxorubicin—which used to be called adriamycin) have been conducted over the years, all of which found that DMSO treated these injuries. The animal studies include:
•A 1981 rat study of doxorubicin extravasations showed that daily topical applications of 1 ml 90% DMSO for 2 days produced a small decrease in ulcer diameter, whereas 10% DMSO with 10% α-tocopherol produced a significant reduction in ulcer diameter.
•After testing ten agents to see if they could treat ulcers created by intradermal doxorubicin (in pigs and rats), a 1982 study determined that DMSO was the only one that did. A different study (which used intradermal mitomycin C to create skin ulcers in mice) likewise found DMSO was the only agent that healed the resulting ulcers (and prevented them if given beforehand). Another study in pigs found that DMSO prevented doxorubicin induced ulcers from forming, while a fourth found DMSO healed vinorelbine extravasation injuries in rats.
•A 1984 and 1987 pig study that found DMSO treated extravasation injuries.
•A 1992 and 2013 rat study that found DMSO protected against doxorubicin injuries.
Comparable results have also been seen in humans such as:
•A 1983 case report detailed a striking improvement after DMSO was given for a daunorubicin extravasation (along with another 1983 case report where DMSO was used to treat a doxorubicin extravasation injury).
•A 1989 series of 4 patients with extravasation injuries found that DMSO, ice, and a steroid injection prevented ulcerations and tissue death.
•A 1991 series of two patients showed DMSO was extremely effective for healing the severe skin necrosis caused by the accidental extravasation (leaking out of a blood vessel) of mitomycin C, a rare but serious complication of the drug estimated to occur in 0.01-6% of infusions. Additionally, DMSO was found to work for extravasations that were only detected days after the initial infusion.
•A 1994 case report detailed two cases of DMSO successfully treating extravasation injuries
•A 2001 case report found DMSO healed an extravasation injury (of epirubicin and two other chemotherapy drugs).
Finally, a few human trials have also corroborated these results:
•A 1987 study reported treating eight patients who had an extravasation from either anthracycline or mitomycin C with a topical combination of 10% alpha-tocopherole acetate and 90% DMSO and found in all cases this prevented subsequent tissue necrosis from occurring (suggesting DMSO should be used to prevent the complications which frequently follow anthracycline).
.•A 1988 study gave topical DMSO for anthracycline extravasations every 6 hours for 14 days to 20 patients, which prevented all of them from developing ulcerations. In the 14 who were evaluated at 3 months, there was no sign of residual damage in six patients, while a pigmented indurated area remained in ten.
•A 1995 study gave topical DMSO (for 8 hours a day over 7 days) alongside 3 days of intermittent cooling to every patient who experienced an extravasation over a 3.5 year period (which was either from doxorubicin, epirubicin, mitomycin, mitoxantrone, cisplatin, carboplatin, ifosfamide or fluorouracil). Of those 144 patients, 127 could be evaluated, of whom only 1 ultimately developed an ulceration from the extravasation and none experienced side effects from DMSO (beyond temporary skin irritation and a breath odor).
•A 1996 study of ten successive patients who experienced extravasation from chemotherapy were given DMSO and alpha-tocopherol, all of whom avoided ulceration or tissue death.
•A 2004 study of 147 patients with extravasations of anthracyclines (which typically leads to 28% developing ulcerations), found 99% DMSO caused only 1-2% of them to develop ulcers.
Lastly, a 2007 study explored applying DMSO and α-tocopherol as a gel rather than a liquid solution to treat extravasation injuries (which appeared to hold promise).
Other Injuries
A few other studies have also been conducted on DMSO mitigating the effects of chemotherapy:
•DMSO was found to prevent doxorubicin cardiac toxicity.
•In two cases, DMSO successfully treated palmar-plantar erythrodysesthesia resulting from doxorubicin treatment.
•Doxorubicin is sometimes injected into the eyelid to treat eye spasms. DMSO prevented the skin death often associated with this treatment.
•DMSO was shown to protect against the birth defects caused by hydroxyurea
•DMSO was found to reduce the carcinogenicity of chlorambucil (as this chemotherapy often causes a secondary tumor to form after the initial treatment).
•Bleomycin is well-known for injuring the lungs (e.g., causing pulmonary fibrosis). In a 1985 rat study, DMSO was observed to prevent most of the damage bleomycin caused to the lungs and prevent the weight loss associated with its administration. However, in a follow-up study (that used a different dosing regimen), DMSO was instead found to increase the toxicity of bleomycin.
Note: a third 1987 study also evaluated the effect of bleomycin on pulmonary fibrosis.
Potentiating Medications
One of the major problems with chemotherapy is that since it’s given to the whole body, much of it goes to the wrong target (e.g., healthy cells) particularly when very high doses need to be used (e.g., to overcome the blood-brain barrier). As such, over the years, approaches have been developed to lower the amount of a generally toxic chemotherapy drug that needs to be given as, higher (standard) doses of chemotherapy frequently can be more harmful than the cancer itself.
For example, since cancer cells have more insulin receptors than normal cells (as this allows them to take more sugar out of the blood stream) chemotherapy can be mixed with insulin so that it is disproportionately taken up by cancer cells. As a result, over the decades, many have found this allows them to use much lower (non-toxic) doses of chemotherapy to cure their cancers (e.g., see this website).
DMSO essentially does the same thing (as do a few other natural cancer therapies we utilize). Still, unfortunately, despite an immense amount of promising research on DMSO and cancer, there was minimal follow-up in the decades that followed. Along these lines, the only doctor I know who publicly wrote about it (e.g., see this book) would use DMSO in conjunction with insulin potentiation therapy (e.g., by mixing DMSO right into the chemotherapy infusion syringes or saline bags), and prioritized its use for brain cancers (as DMSO could get the chemotherapy there).
In turn, the rationale for this was that DMSO passes the blood brain barrier and concentrates inside tumors (e.g., this study found a 1.5X increase in brain tumors), and when used as a contrast agent, DMSO has been found to be able to detect brain tumors that cannot be detected with conventional contrast agents (e.g., gadolinium). In contrast, DMSO and 5-FU were not observed to cross the blood-brain barrier (which may have been due to the dose used).
Note: because the standard contrast agent used for MRIs (gadolinium) causes some recipients to develop significant chronic illnesses, I try to avoid unnecessary scans. As such, I’ve patiently waited for an alternative contrast agent to be developed (e.g., there are decades of data showing manganese based contrasts are a safe and effective alternative to gadolinium1,2,3 but despite this, we are still a long way from it being available).
DMSO and Chemotherapy
When the FDA clamped down on all DMSO research, quite a few promising studies had emerged that suggested DMSO could considerably lower the doses of many common chemotherapy agents (thereby making them far less toxic and hence far more survivable). Unfortunately, all of that got swept away and unfortunately, in the many pushes that followed to make DMSO legal again, its uses for cancer were rarely focused upon (and thus became almost completely forgotten).
Note: when reviewing this section, it is important to remember that DMSO can increase the potency of chemotherapy drugs, so in many cases lower doses are needed (which in turn requires working with a doctor who is either familiar in this area or one who wants to read this article and can monitor you during the treatment to determine the correct dose). Additionally, most of the research on DMSO for using DMSO to potentiate chemotherapy drugs was done on the older ones that are less tumor specific, and as a result, may not be as applicable to the newer drugs.
Combination Therapies
•A 1975 study of 65 patients with incurable cancers (most of which had received conventional therapies) were given a low dose of cyclophosphamide mixed in DMSO with GABA, GABOB, and acetylglutamine either intravenously (typically) or intramuscularly (rarer). Objective or subjective remissions were obtained in 57 of the 65 patients (e.g., many went from being in extreme pain to being pain free), and almost all of those with lymphomas or breast cancers had complete recoveries, while about half of those with other incurable cancers recovered.
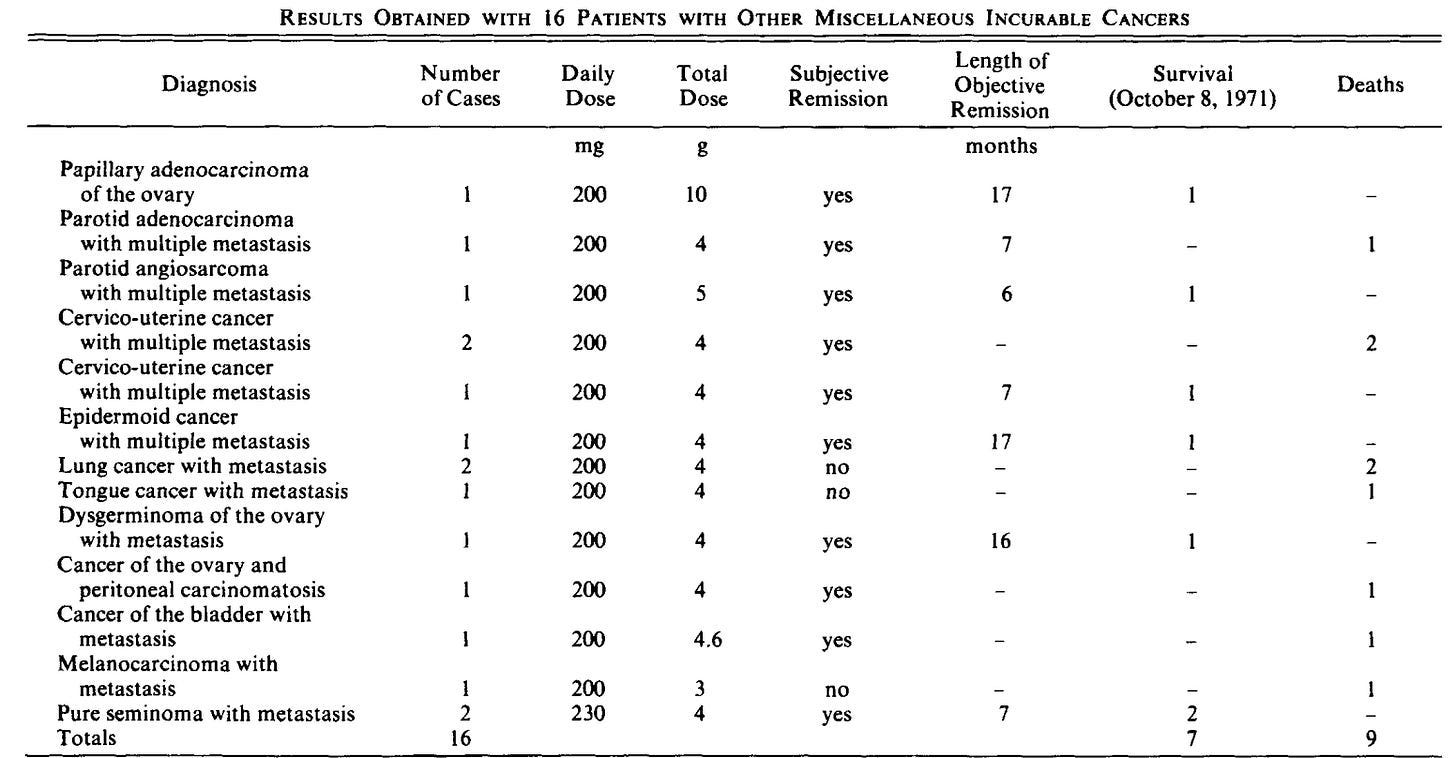
Note: this study also found patients who could not tolerate cyclophosphamide were able to with DMSO.
•A 1975 rat study found that oral DMSO increased the potency of cyclophosphamide, which in turn required lowering the cyclophosphamide dose to avoid creating toxicity (which the authors felt could potentially create a safer and more effective dosing regimen for cyclophosphamide). They also found DMSO increased the survival times in advanced cancers by potentiating the following drugs 6-mercaptopurine, Methotrexate, Chlorambucil, Vinblastine, Procarbazine, CCNU, MCCNU, BCNU, Daunomycin, Nitrogen mustard, Dianhydrogalactitol, Norbornyl, and Adriamycin. In contrast, no benefit was seen with cytosine arabinoside, vincristine, and 5-fluorouracil (all of which did not have the lowered toxicity threshold observed for cyclophosphamide).
Note: an ambitious follow-up project was made to test various other anticancer drugs. However, just as clinical trials were scheduled to start, they were halted by a jurisdictional dispute within the FDA.
•A follow-up 1983 study then determined that DMSO did not increase the toxicity of any chemotherapy drug but did temporarily increase (for 2-3 hours) its initial levels in the body
In summary, we believe that DMSO modifies the pharmacology of CPA [cyclophosphamide] in the rat by increasing the systemic availability of CPA and enhancing diffusion of the drug across tissue membranes. It likewise accelerates drug efflux from the plasma, which correlates with the observance of little increase in drug toxicity when it was used together with DMSO in the therapeutic studies described above. The ability of DMSO to increase the effectiveness but not the toxicity of certain antineoplastic compounds is probably the result of a rapid pulse of compound through the tumor tissue.
Additionally, that study also found that:
These changes primarily occurred when oral DMSO was given concurrently with an oral form of the chemotherapy drug.
Certain tumors had a higher response to DMSO being added in than others.
DMSO being added reduced the overall growth of the tumors.
It was unclear if these results also held true for humans, as two small human studies (this one and this one) did not observe them.
•A 1987 study of patients with cervical cancer found that applying metronidazole dissolved in DMSO to the cervix increased the tumor’s regression following radiation therapy.
•A 1988 study provides the most detailed data on how DMSO potentiated chemotherapy agents (particularly against breast cancers) along with shedding light on the innate anticancer activity of DMSO:
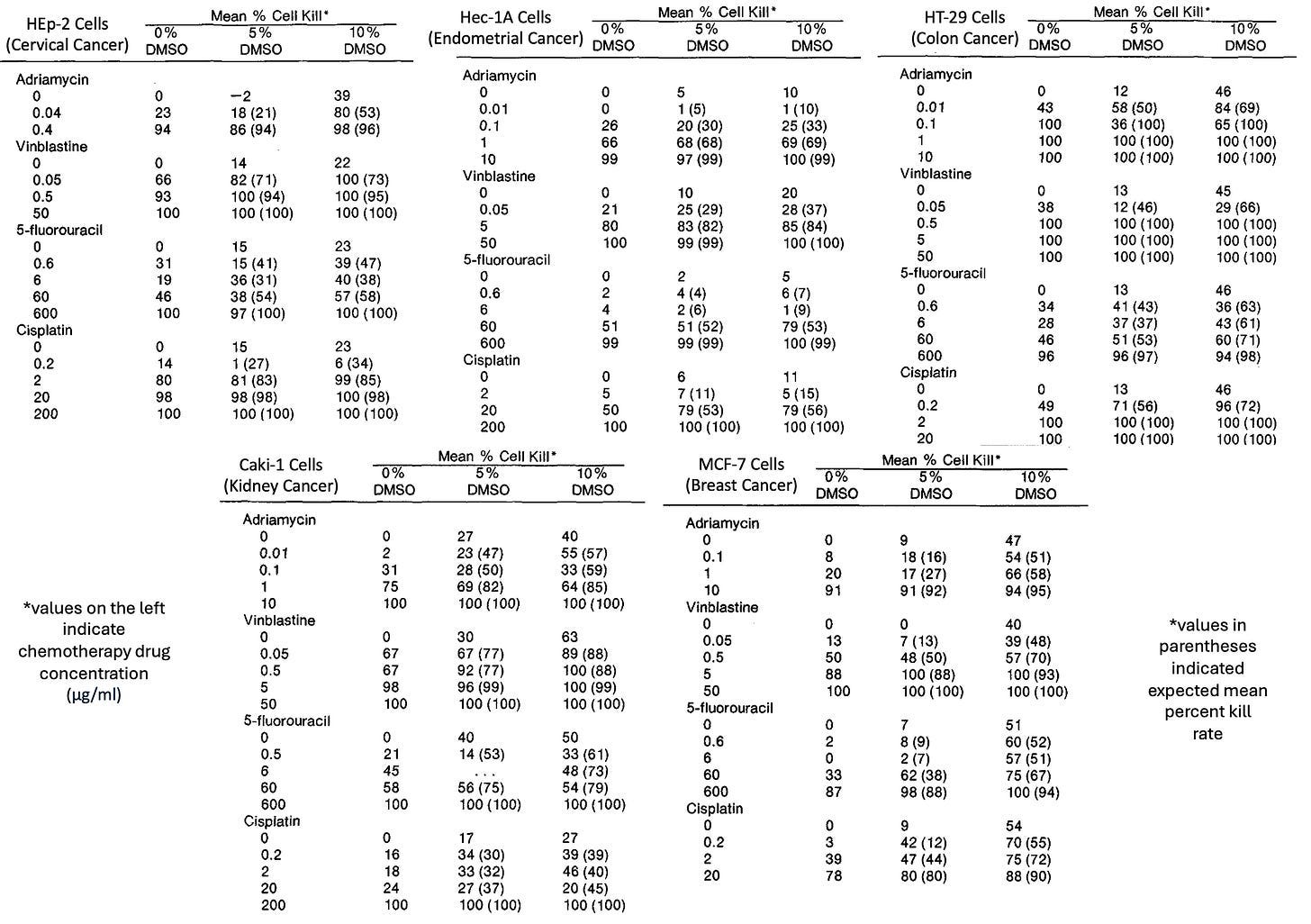
Note: a follow-up study by those authors found that 10% DMSO greatly enhanced the potency of a variety of anticancer drugs on ovarian cancer cells.
•In rats treated for bladder cancer with doxorubicin, adding 10% DMSO caused a 7.1 fold increase in bladder concentration (while 50% caused a 12.1 fold increase) and a 9.3-9.6 fold increase in the lymph nodes. Mixing doxorubicin in 5% DMSO reduced the amount of doxorubicin needed to eliminate cancer by 44%.
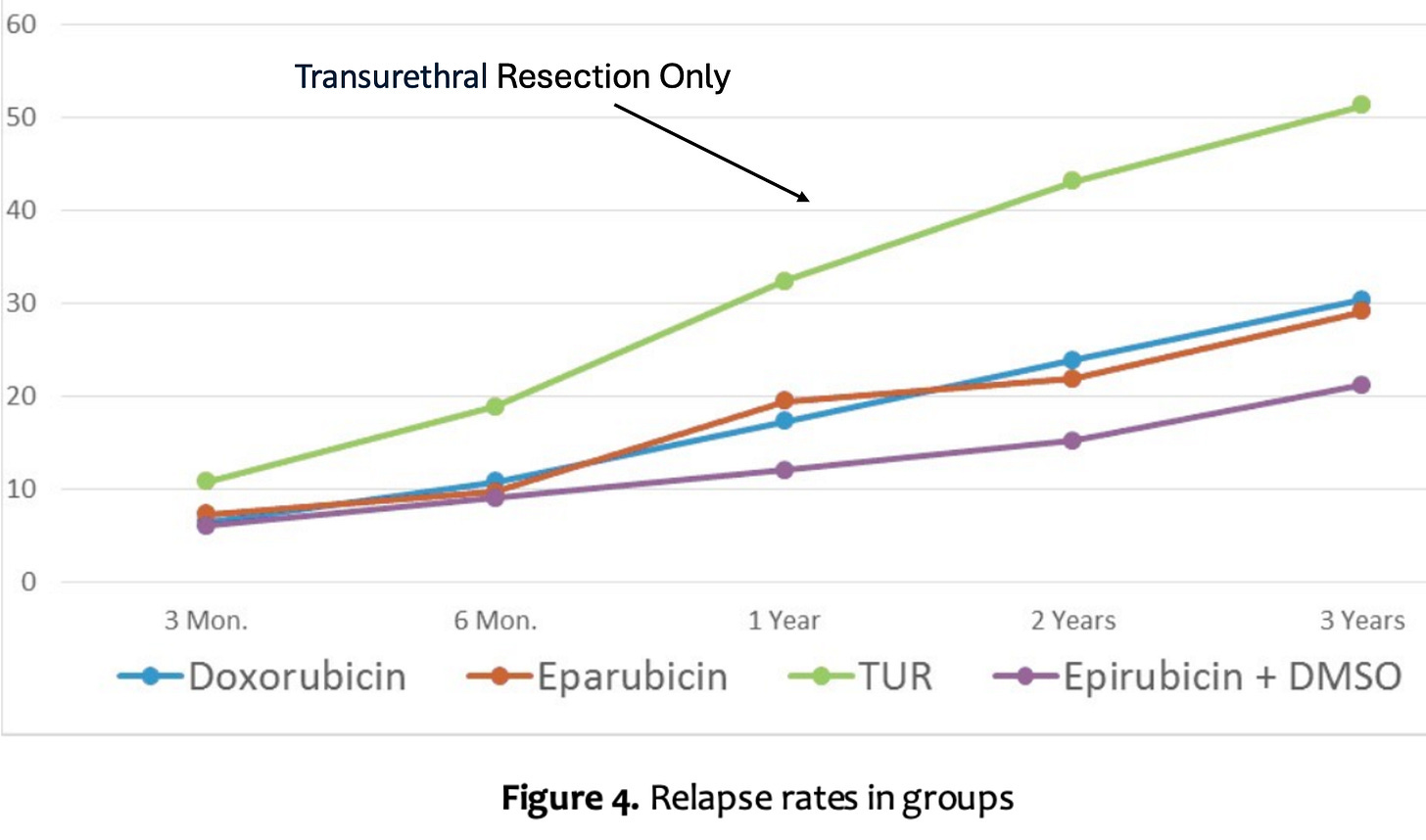
•A 2021 Ukrainian study of 52 patients with bladder cancer who had it surgically removed found that giving intravesical DMSO in conjunction with chemotherapy significantly reduced the 5 year recurrence, and there were no side effects from doing so.
Cancer Barriers
One of the major issues with treating cancers is that cancer cells can become resistant to chemotherapy. In light of this, the results from a 1969 study are quite insightful.
After observing that cancerous epidemical cells (unlike normal cells) were able to resistant cytotoxic (chemotherapy) drugs entering them by creating a fibrin-like “cytoplasmic barrier,” that study discovered that mixing the drugs with DMSO allowed them to penetrate cancerous cells (a result also found in another 1969 study and a 1971 study).
Furthermore:
•A 1983 study found that cancer cells had a disordered cytoskeleton (which is now well recognized) and an impermeable barrier around the cell that resisted chemotherapy drugs from entering.
When DMSO was given, it allowed drugs to enter the cells. It dramatically increased the potency of cytoskeleton-targeting drugs (e.g., making 1/30th to 1/1000th of their usual dose be needed), disrupting cancer cells by causing their disorganized cytoskeleton to swell. Lastly, the authors reported great success with intravenous DMSO-vinblastin (which caused tumor masses to necrotize rapidly).
Note: vinblastin works by targeting the microtubules.
•A later 2022 study (mentioned earlier in this article) found that 1% DMSO significantly altered the cytoskeleton of melanoma cells (e.g., how they attached to their extracellular surroundings) but not normal cells, and that when DMSO was combined with CaS (which releases ions that can trigger programmed cell death), the there was no noticeable effect on the skeleton of normal cells, but there was heavy disruption to the cytoskeleton of cancerous cells.
Note: it is well known that healthcare workers who routinely administer chemotherapy periodically have accidental exposures to it (e.g., via vapor inhalation), so organizations like the CDC and NIOSH have worker guidelines about it (as these exposures increase the risk for a variety of issues including cancers). Since DMSO will cause chemotherapy drugs it is mixed with to be absorbed through the skin, it is crucial to be extremely cautious when administering it with chemotherapy drugs (particularly when applying it topically).
Cisplatin Studies
One of the most extensively tested DMSO combinations is with cisplatin, a drug that has shown significant promise for pairing with DMSO, but is also a concern as DMSO can bind to platinum containing drugs (cisplatin, carboplatin, and oxaliplatin) and partially inactivates them. As a result, some authors believe DMSO should not be taken concurrently with these drugs, but other data argues against that position. The cisplatin studies are as follows:
•A 2015 mouse study showed DMSO reduced the kidney toxicity of cisplatin, increased its reduction in tumor size and increased the survival time in animals who received it. Likewise, this study found DMSO increased cisplatin’s efficacy and decreased its toxicity.
•A 2019 lung cancer cell study also showed DMSO increased cisplatin’s efficacy..
•Another 2019 study found that DMSO doubled the toxicity of cisplatin to lung cancer cells (thereby making a much lower therapeutic dose needed) and reduced the cancer cell’s resistance to chemotherapy drugs.
•A 1995 study of rats with experimentally induced bladder cancer found combining DMSO with cisplatin decreased the depth of cancer invasion compared to cisplatin alone or to placebo.
•A 2015 study found 0.1-0.3% DMSO reduced the efficacy of Cisplatin against CML.
•A 1991 rat study found that giving DMSO with cisplatin reduced its kidney toxicity (and weight loss) but did not reduce its toxicity to carcinosarcoma.
•A 2008 study found that mixing cisplatin with DMSO reduced both its neurotoxicity and toxicity to cancer cells, with the decrease in neurotoxicity being approximately twice the reduction in cancer cell toxicity. It also significantly decreased cisplatin’s toxicity to the kidneys and slowed its elimination from the body.
•After a 1997 study noticed a delivery system for cisplatin was causing no toxicity in dogs with osteosarcoma, the investigators suspected the DMSO component of the delivery system was responsible. Then they were able to verify that there was reduced anticancer activity for cisplatin when it was mixed with DMSO.
•A 2022 study found DMSO caused a fourfold reduction in cisplatin’s toxicity to E. Coli bacteria (cisplatin is also toxic to bacteria).
•In a 1982 study of dogs with bladder cancer, mixing DMSO with cisplatin caused a threefold increase in how much was absorbed into the bladder muscle (which is similar to what this study found).
•A 2014 rat study found that DMSO did not enhance Cisplatin’s toxicity to the inner ear, while a 2013 zebrafish study found DMSO enhanced cisplatin’s toxicity to the ear’s hair cells.
Other Chemotherapy Studies
DMSO has also been shown to enhance the efficacy of a variety of other cancer drugs:
•A 1975 study found DMSO in conjunction with ifosfamide treated carcinosarcoma in rats.
•A 1981 cell study found that DMSO did not increase cyclophosphamide’s toxicity, but potentially reduced its efficacy against lung cancer.
•A 1986 study found DMSO increased acute lymphocytic leukemia (ALL) sensitivity to nitrogen mustard in a dose-dependent fashion (the compound cyclophosphamide is derived from).
•A 1989 study found that DMSO enhanced the ability of cisplatin, 5-FU and cyclophosamide to slow aggressive (implanted) prostate cancers.
•A 1994 case report detailed two AIDS patients with Kaposi’s sarcoma who were successfully treated with topical DMSO mixed with bleomycin with no toxicity being observed.
•A 1998 study found that DMSO increased the potency of 5-fluorouracil and doxorubicin.
•A 2001 study found that DMSO induced differentiation in human breast cancer cells and increased their sensitivity to doxorubicin.
Note: a computer modeling study concluded DMSO may counteract Tamoxifen’s anticancer effects.
•A 2004 study found that DMSO caused a 71.7% growth inhibition of breast cancer cells at 96 hours and improved the safety and efficacy of the cancer drug gemcitabine.
•A recent study found that DMSO significantly reduced the growth of prostate cancer cells, and this effect increased when it was given concurrently with nelfinavir.
Lastly, DMSO when combined with 5-fluorouracil (5-FU) has repeatedly been found to treat skin cancers and warts. For example, this 1967 study found DMSO significantly increased 5-FU’s potency and made 5% able to locally treat keratoacanthoma, superficial basal cell and early stage squamous cell carcinoma without causing any adverse effects and likewise, this study used DMSO to enhance 5-FU’s ability to treat seborrheic keratosis (something which also responds to DMSO alone).
Note: a few studies have found DMSO can sometimes increase the carcinogenicity of a cancer causing substance if given concurrently with it and DMSO worsening or preventing something’s carcinogenicity was highly dependent on how each was applied.1,2,3,4
Photodynamic therapy
Photodynamic therapy works by mixing a photosensitizer (e.g., 5-ALA) in tumors with light so that a reactive chemical is generated, which destroys the cancer. Since DMSO aids in the formation of the reactive agents, it has repeatedly been found to enhance this treatment:
•A 1995 study found that mixing 5-ALA with 2% EDTA and 2% DMSO eliminated 85.4% of BCCs (in 48 patients), 100% of superficial SCCs (in 5 patients), and partially improved 2 ulcerated SCCs. Additionally, using DMSO and EDTA (when compared to not using it) was found to more than double the response to 5-ALA photodynamic therapy.
•Another 1995 study treated 763 BCCs in 122 patients, using either 5-ALA, 5-ALA with DMSO as a pretreatment, or 5-ALA plus DMSO plus EDTA. DMSO plus EDTA was shown to improve significantly 5-ALA penetration depth, doubled ALA-induced porphyrin production (a key part of photodynamic therapy), and in patients with nodulo-ulcerative lesions, the response rate went from 67% to above 90% (for lesions less than 2mm thick) and from 34% to 50% (for lesions more than 2mm thick).
•In a 2009 study, DMSO plus 5-ALA photodynamic therapy was found to entirely eliminate 55 out of 60 basal cell cancers (with a good cosmetic outcome), of which 81% did not recur after 6 years (with 91% not recurring if two rather than one treatment was given).
•In another 2009 study, 19 cases of Bowen's disease (early SCC) and 15 BCCs received a single course of 5-ALA with DMSO and EDTA (activated by a 630nm diode laser). At 3 months, 91.2% of the tumors were gone, while at 60 months, 57.7% of Bowen's disease and 63.3% of BCCs had not recurred.
Note: natural therapies (discussed below) have also been shown to be highly effective skin cancer treatments when combined with DMSO.
Other Pharmaceutical Combinations
Other (less toxic) drugs have also shown promise for cancer when combined with DMSO. For example:
•Since cervical cells can easily be gently scraped off and examined, a team of researchers evaluated how a variety of substances caused them to transform into cancers or caused cancerous cells to differentiate into normal cells. From this, they found that while DMSO alone did very little, if it was combined with a small amount of dexamethasone, within 2-3 weeks, it rapidly transformed the cancerous cells (e.g., carcinomas in situ or metastatic cervical cancers lesions) to normal ones and healed the surrounding tissue (e.g., malignant tissues, typically red, granular, and friable, became smooth, pink, and resilient with diminished bleeding and vascularity), and at the time of publication, reported successfully treating six out of six patients, including one with metastatic cancer.
Note: DMSO in combination with colchamine has also been used to treat skin cancer.
•A 2015 study found that DMSO significantly increased the toxicity of organotin polyethers on various cancer cells.
•One approach to eliminating cancers is using a magnetic molecule that can be heated with a magnetic field. When a 2021 study attached that substance to DMSO, it was found to be an effective treatment for cervical cancer and significantly enhance the potency of the cancer drug carmustine.
•In a 2002 study, animals exposed to cancer-causing nitrosamines and treated with polyene antimycotics combined with DMSO showed significant cancer-fighting effects. After 5 months, 76% of these animals survived, compared to only 35% survival in the untreated control group.
Note: occasionally research papers emerge on new DMSO containing drugs (e.g., ruthenium based ones) that effectively eliminate cancers (e.g., this 1989 study, this 1994 study and this 2012 study where one selectively targeted metastastic tumors, or this 1995 study, this 1998 study, this 2022 study, this 2022 study and this 2023 study).
Natural Combination Therapies
In the same way DMSO potentiates chemotherapy, it can also enhance natural compounds. For example:
•A 1969 study found that DMSO, when combined with heat and vitamin A, selectively targeted cancer cells (and facilitated the release of lysosomal enzymes).
•A 2018 study found that DMSO and a plant extract selectively arrested cell growth and induced cell death of colon cancer cells.
•A 2023 study found that when fatty acids were isolated from the urine of healthy cows and mixed with DMSO, it was an effective therapy against breast cancer cells, while when this combination was instead tested on Human Gingival Mesenchymal Stem Cells, no toxicity was observed.
In turn, while DMSO shows great promise in many of the approaches thus far highlighted throughout this article, I believe its greatest value is to be combined with a potent natural substance. This is because a few of those substances have demonstrated remarkable efficacy in treating cancer, are much more accessible, and are far safer than the conventional options (particularly considering the risk of DMSO accidentally bringing an unwanted toxin into the body).
In the final part of this article, I will cover the most remarkable natural DMSO combinations for cancer and how they can be used (e.g., for skin cancer), along with guidance for some of the topics mentioned throughout the article (e.g., radiation and CT scan protection, cervical cancer therapeutic combinations and other natural ways to potentiate chemotherapy) along more general instructions for DMSO sourcing and dosing common DMSO applications (e.g., pain or arthritis) and other cancer treatment approaches.
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.