


How Do We Navigate Uncertainty In These Perilous Times?
Investigating the Mysteries of the mRNA Vaccines

One of the great challenges in life is that many of the dilemmas we face have no clear cut answer, and frequently, diametrically opposed solutions to those dilemmas emerge which are both arguably correct but also arguably incorrect.
For instance, I know of more cases than I can count of someone “trusting” someone else they thought they had every reason to trust then get taken advantage of by that individual. Conversely, I know many people who have have been scammed in the past and are hence so distrustful they close the door to immensely beneficial opportunities that periodically come their way and greatly set themselves back in life by doing so.
Much of my life has revolved around a fascination over what constitutes “the truth,” and in this, I find a similar issue emerges. If you are too trusting of the sources you come across, you will inevitably come to believe falsehoods, whereas if you are too skeptical of the sources you encounter, you will inevitably fail to recognize critical truths.
As a result, a variety of schools of thought have emerged on how that challenge should be navigated. Unfortunately, regardless of the approach someone chooses to follow, in practice people tend to simply be more trusting of information which conforms to their pre-existing beliefs and more skeptical of that which diverge from them (which is commonly referred to as the “confirmation bias”).
Note the methods people use to filter information is discussed in more detail here.
Ultimately, there is no correct solution to this dilemma, as no matter how hard you try to calibrate yourself, you will either be too skeptical or too trusting of some of the information you come across. This in turn has led many to adopt the wise words “trust, but verify.”
My own solution to all of this has essentially been to do both. A third of my mind entertains and considers a lot of ideas which are quite out there, another third of my mind sees reason after reason to doubt everything I come across (and effectively debates those ideas with the first third of my mind), while the final third acts like a “judge” and tries to weigh which side is more correct.
Because of this, I consider a lot of things that I never speak about publicly, am ultimately undecided on many of them, and am much more selective in what I put forward publicly (e.g., on this Substack) because I feel it is critical I don’t put forward something I know in the back of my mind could be a falsehood.
This is similar to the experiences that has been shared by many leading figures in this movement. In the early days of COVID, they could tell something was amiss but were not sure just how bad things actually were and they simultaneously knew something had to be done to stop what was in the works. However exactly what needed to be done was much less clear, and each of them was terrified of putting forward the “wrong” solution, as doing so would ultimately hinder the correct one from making it to the public’s attention but simultaneously, doing nothing would guarantee a bad outcome for everyone.
For example, there were many promising therapies we all worked to promote to treat COVID-19 from the start (as we all recognized COVID would turn into a disaster unless an effective and already available treatment for it was found). Yet, despite working for months (starting in Dec 2019) to find that treatment, the one I ultimately settled on (and did a lot of work to have it become part of the standard of care for treating COVID-19) I no longer even use now as I’ve found much better options and I realized the preliminary data on the therapy I promoted was not as good as what we later saw in clinical practice.
Likewise, countless prominent figures in this movement have publicly stated (or shared with me personally) that they held back saying a lot of what they wanted to say because they felt doing so would receive so much pushback it would prevent them from being able to share a lot of what they could share and also felt was critically important to be heard.
Note: I share the above because the past conduct of many prominent figures in our movement (some of whom I know personally) has been used as a justification to call their present conduct into question. I believe that if one can grasp just how difficult it was to challenge the COVID cartel and how unclear the correct way to go about fixing things was, a lot of their early approaches become much more understandable.
The Mechanistic Trap
Frequently I will observe something appears to be happening but will not be able to explain why it is happening. Typically when this occurs, I assume one or more of the following is true:
•I am wrong and my observation is not real.
•The causality I appear to be observing (e.g., the increased anxiety sweeping my hospital immediately after an annual vaccination for all employees) is an artifact of something else I am not aware of (e.g., the actual causal factor is the current solar activity).
•The observation is real but my current scientific knowledge is lacking so I am not aware of an existing scientific explanation for the phenomenon.
•The observation is real, but it falls into an area which has not yet been sufficiently researched (which is more common than you’d think as there is an almost infinite number of things which could be researched).
•The observation is real, but it requires considering scientific paradigms that go beyond the scope of what orthodox science wants to consider the possibility of (e.g., this applies for many spiritual phenomena).
While this list might seem a bit excessive, I feel it is important to share because it lies in contrast to the default response of most scientifically trained individuals—when they observe something they do not have a (conventionally accepted) mechanism to explain, they reflexively dismiss the validity of the observation and deny that it is real. Since this often leads to the erroneous assumption something is not real, I’ve termed this behavior the “mechanistic trap.”
Note: from working in drug development I’ve come to appreciate one of the biggest issue with the drug regulators is the mechanistic trap, as it causes them to habitually refuse to consider many integrative therapies and likewise to rubber stamp many bad drugs with incorrect but nice sounding mechanisms (e.g., that anti-depressants “work” by increasing brain serotonin).
Navigating Uncertainty
A foundational concept in game theory is “unknown information,” which essentially says that if you know all the existing information, there is one “optimal” move to make, but once some information is not known, there is much more ambiguity as to what the correct move is. In turn, games tends to select their winners from those who best know how to navigate the game’s informational uncertainty.
In some games, the “uncertainty” is a product of being unable to see too many steps ahead. For instance, in tic-tac-toe, since there are a relatively few number of possible moves, if you start by taking a corner, unless your opponent takes the middle, you are guaranteed to win, whereas in games like chess (and even more so with go), there is are so many possible play sequences no human or computer has yet “solved” either game.
In many other games (poker being the classic example), we instead have uncertain information and countless methods, in turn, have been developed for leveraging that informational uncertainty to win (e.g., bluffing, reading the opponent and probability calculations).
For example, one of the most common dilemmas in investing is how high a risk you can tolerate. In turn, the highest rates of return are almost always seen with the riskiest investments (e.g., I’ve lost count of how many people I know who lost their life savings to some type of a Ponzi scheme like a sketchy hedge fund everyone in their social circle fell for because of the incredible financial returns it promised).
Note: one of the major problems with our economic system is that once you become too powerful, you gain an incredible informational advantage. For example, there are countless stories of politicians in Congress making incredibly successful investments in a stock immediately before passing legislation they had worked on that was expected to increase the value of their stock (this practice is known as insider trading). Likewise, many larger business interests can bribe politicians or regulators to make sure uncertain events in the marketplace will work out in their favor.
In my case, I typically go for low-risk low-return investments partly because I don’t need the high rates of return and more importantly because I do not want my focus and energy going to the something I do not believe benefits my soul or the world around me. However, in many other areas I really like working with unknown information and using the skills of inference to try and guess at what is happening.
These include:
•Trying to predict future events.
•Grasping the underlying currents precipitating a social dynamic.
•Uncovering a mechanism for an inexplicable physiologic process I am observing.
•Throughout my own meditation practice.
•Helping a challenging patient.
In each of these cases, I am drawn to engaging with the situation because I think the subject is fascinating, the process develops me and because it often allows me to do things I find to be highly meaningful (e.g., while a low rate of return for a financial investment is not a big deal to me, a low rate of recovery for a suffering patient I invested myself in healing is a big deal to me).
Note: I believe the slice of reality each of us ultimately sees is largely a product of our own emotional and unconscious biases. In my case, I am drawn to ambiguous things that don’t make sense as I frequently find when my understanding of that subject “expands” and opens me into a broader reality, my appreciation of life increases as well. As best as I can tell, this bias was a product of me never feeling emotionally satisfied within the conventional paradigm society feeds to all of us.
The Mysteries of Spike Protein Illness
Since COVID-19 emerged, and even more so once the vaccines hit the market, I’ve noticed a variety of highly concerning but perplexing things happen. This in turn created a situation where from the very start, I was certain something was amiss, but I could not provide a credible explanations for many of my observations.
Some of these included:
•Why did COVID-19 cause profound fluid stagnation in the body?
•Why did COVID-19 sometimes have major psychiatric or spiritual complications?
•Why did some people get very ill from COVID-19, but many others had nothing more than a cold—and more importantly why was it often almost impossible to predict which of these would happen?
•Why were massive and mysterious elastic clots repeatedly being found inside vaccinated individuals?
•Why were some people so much more susceptible to the effects of the vaccine than others?
•Why do the blood clots and sudden cardiac injuries created by the vaccine happen immediately in some and much later in others?
•Why does the vaccine spike protein seem to persist indefinitely in some but not others?
•Why is vaccine shedding occurring when this in theory should not be possible for the mRNA vaccines?
•Why does the vaccine, like COVID, frequently seem to affect the lungs and the blood vessel that feeds them?
Note: I have observed even stranger things too. For example, after I heard of dozens of reports of people turning magnetic from the vaccine, I waited until I heard about someone in my network who allegedly had this happen to them, and then traveled quite far to see them. In their case, I was able to verify they were magnetic, but it was an odd form of magnetism as they appeared to magnetize paramagnetic metals (so after a bit of time, that metal would stick to their skin and appeared to lightly pull something underneath their skin). I thought about this for a long time (e.g., I researched paramagnetism in detail) and I fully admit I had almost no confidence in any of the theories I put forward to explain how that could have happened.
Later, a colleague sent me an informal study from Luxemborg which found 29/30 vaccinated (with both mRNA and non-mRNA vaccines) were magnetic, while 0/30 unvaccinated were. A month later, James Thorpe MD conducted a detailed (and larger) study which found about 60% of both vaccinated and unvaccinated individuals were magnetic, leading Thorpe to conclude that humans have some degree of natural magnetism which had nothing to do with vaccination.
In turn, with many of the above points, I kept searching for answers and had faith that eventually, a decent explanation would surface. Conversely however, I was careful to not assert the validity of any of these observations until I had explanations I felt could substantiate my claims (as I felt it was irresponsible to espouse something that might not be true). For example, after months of deliberation, I put forward this hypothesis to explain the mysterious elastic clots found in the vaccinated and it is now viewed as one of the most likely explanation for this otherwise inexplicable phenomenon.
Similarly, until I felt I had a least a little bit of ground to stand on, I simply did not share the more inexplicable things I’d observed, as I felt doing so wouldn’t accomplish anything besides weakening my credibility and thus give people a reason to dismiss the important points I could share which did have stronger evidence backing them up. For example, in the initial log of vaccine injuries I spent a year compiling (which effectively launched this Substack) I deliberately avoided mentioning the shedding or magnetism as I was certain people would latch onto that and use it to dismiss the existence of all the other injured people I had documented.
Fortunately, I’ve come across quite a few mechanisms which do explain many of the inexplicable phenomena I’ve seen with the COVID-19 vaccines (e.g., the cause of the fibrous clots). Since many of them are relative to explaining some of the greatest concerns people have with the vaccine (e.g., “shedding” and “hot-lots”) the rest of this article will be devoted to discussing them.
Zeta Potential
One of the first mechanisms I identified to explain many of the inexplicable effects of the spike protein was that it had a highly adverse effect on the physiologic zeta potential. Before I go further, I would like to briefly explain what that means.
Anytime something mixes in water (and to some extent in other fluids) it has a few options. It can:
•Dissolve like salt.
•Not mix (and settle to the bottom like sand or to the top like oil).
•Become a colloidal suspension.
A colloidal suspension occurs when a substance in water breaks into small particles that are then prevented from coming together. Since they can’t come together, they distribute evenly throughout the mixture, and cause the liquid to change its characteristics (e.g., milk is a colloidal suspension of milk particles in water). Once this happens, the state of the colloidal suspension is determined by the balance of forces pulling the particles of the substance together and the forces pushing them apart.
Depending on the balance of those factors, the particles of the colloid can be completely dispersed from each other and hence relatively small, or clumped together and quite large (e.g., a kidney stone occurs when the same dispersed particles that are present throughout your body clump together in the kidney and create a solid kidney stone).
The primary forces that pull particles together are the force of gravity (as things will always separate by density), the inherent attraction between molecules (known as the Van der Waals force) and electric attraction between opposite charges. Conversely, the primary forces which separate particles are mechanical agitation (stirring things up), barriers which prevent the particles from contacting each other and matching charges which repel each other.
In most colloidal systems, the primary thing that determines their stability (separation) is if the dispersive negative charges outweigh the attractive forces (although this is complicated to calculate since certain ions like the positively charged aluminum ion have an exponentially larger attractive effect than other positive ions). Zeta potential in turn is used to quantify the net charge difference between a particle and its surrounding.

Since most colloidal systems depend on the mutual repulsion of negative charges (rather than positive charges), the more negative the zeta potential is, the “stronger” the solution’s dispersion is. In turn, the more negative the zeta potential is, the more dispersed the colloidal solution is, while the less negative it is, the more it all clumps together.
Note: Presently, I believe the reason almost all natural colloidal systems are negatively charged is because the liquid crystalline state of water that water forms on polar surfaces (e.g., those particles) is negatively charged and hence each particle is coated with a negative charge.
Since the fluid systems in the body are colloids, the current physiologic zeta potential can have immense consequence. For example, if the zeta potential of the blood weakens, larger and larger clots will gradually form which cause progressively more severe injuries.
Note: the nerves that control the muscles of the face and the movement of the eyes (CN III IV and VIII) are the most susceptible to being disrupted by microclotting. Since vaccines frequently impair zeta potential, deficits in those nerves (especially the abducens) are one of the most common symptoms of a vaccine injury and something I have seen numerous people develop after the COVID vaccines (it’s scary how common this nerve damage is once you learn to look for it).
Since you need a strong positive charge to disrupt the (negatively charged) physiologic zeta potential, and the fluid stagnation (e.g., clotting) I observed with COVID-19 (SARS-CoV-2) was not seen with the original SARS virus, this led to me to see if SARS-CoV-2 had any components that were:
•On its surface.
•Different from SARS-CoV-1.
•Had a strong positive charge density.
Once I realized that the spike protein met all of these criteria, I became very concerned that coming vaccines were being designed to mass produce the spike protein in the body. Since that time, the vaccines have proved themselves to be very dangerous, to have many of the side effects I’d associate with a severe impairment of the physiologic zeta potential, and published research has shown the spike protein is highly disruptive to zeta potential.
Conversely, I have also found that restoring the physiologic zeta potential (which we originally learned to do since it greatly improves the prognosis for a variety of diseases) was one of the most impactful things we could do to treat COVID-19 vaccine injuries.
Note: the effects of an impaired zeta potential are the easiest to recognize in the blood, but consequential adverse effects also occur throughout the other fluids of body (e.g., in the lymphatics).
Quality Control
Many people thought that producing the mRNA vaccines in the timeline dictated by Operation Warp Speed was nearly impossible and could only be achieved by cutting a lot of corners (e.g., by skipping many of the preclinical safety studies, running fraudulent clinical trials and not having the FDA inspect the vaccine manufacturing sites—something which FDA whistleblowers admitted was already a huge issue prior to Operation Warp Speed).
Since one of the greatest challenges with bringing a pharmaceutical to market is figuring how to correctly produce large amounts of it, for those with insider knowledge of the pharmaceutical industry, quality control of its manufacturing process was one of their greatest concerns with the COVID vaccines. In turn, throughout the vaccine rollout, we have had a variety of signs that vaccine toxicity varied by lot and the vaccines were not produced in accordance with good manufacturing practices.
Some of the evidence for the hot-lots included:
•Researchers repeatedly identified them in VAERS (and recently in a peer-reviewed publication), while anecdotally, we found those with vaccine reactions typically had received a “hot” lot.
•I and colleagues repeatedly saw countless cases of individuals having immediate and significant reactions to the vaccine but in contrast other cases where the individual had no reaction whatsoever, suggesting their injection had not contained the same vaccine. Furthermore, I saw a few cases of people who had been vaccinated at the same time (e.g., a husband and wife) who then developed “rare” and severe injuries (e.g., a heart attack for one and a stroke for the other) shortly after vaccination, which suggested the (hot) lot they had been vaccinated with had a much higher probability of injuring people.
Note: these observations were also supported by a lot of people I spoke to utilizing muscle testing around the country.
In addition to signs suggesting the presence of hot-lots (which could not exist if a consistent manufacturing process was followed) some of the other indications the mRNA vaccines were adulterated products included:
•Physical contaminants—Japan pulled 1.63M vials of Moderna’s vaccine after visible metal particles were found in them and when examining vaccine vials, Ryan Cole found glass shards in the vaccines. Both of these suggest the production of the vaccines was rushed to the point basic quality control steps were not taken.
•mRNA integrity—Leaked files from Europe’s FDA demonstrated that the drug regulators were aware much of the mRNA in the vaccines were mRNA fragments rather than the complete vaccine sequence. This suggests that the vaccine mRNA was poorly produced.
•mRNA stability—The mRNA was observed to break down quickly (e.g., into the previously mentioned fragments) and it was unclear how to prevent this.
Note: I suspect the obsession with ultra-freezing the vaccines at the start of the roll-out was a PR-ploy done by Pfizer to assuage the regulator’s concerns the mRNA was fragmented under the logic that the breakdown was only a result of inadequate temperature control after production, rather than also being an inevitable consequence of the manufacturing process. For example, we found evidence (which to the best of my knowledge was never refuted) that the data (Western Blots) Pfizer produced for regulators to demonstrate the mRNA vaccines were producing their intended protein product were in fact computer forgeries (which in turn suggests the actual proteins being produced were not what was advertised).
•Temperature control—Once the vaccines hit the market, the interest in ultra-freezing them rapidly waned and before long was largely forgotten. Similarly, more and more we observed vaccines being left out on a table all day long at vaccination sites. This again suggested people were receiving different vaccine doses as some contained mRNA which had more significantly broken down.
Note: since a large number of relatively untrained individuals administered the vaccine during the rollout, it is likely other steps were also incorrectly followed (e.g., aspirating before injecting, or drawing up the correct vaccine dose).
•Hot-lot distribution—In Europe, lots were found to be more toxic in Belgium (the vaccine production site for Europe). This suggested that the closer to the time of production a vaccine was injected, the more harmful it was (whereas later on much of the mRNA had time to break down and make less spike protein in the body). This was also demonstrated by data repeatedly showing mRNA vaccines in Sweden repeatedly and rapidly became less dangerous the further from their production time that they were injected.
•Vaccine production—when Ryan Cole did a recorded examination of the vaccines with Del Bigtree they found:
We looked at all the different vaccines and I think one of the conclusions we came away with is that it’s just a hodgepodge..there were vaccines that seems as though there were no particles within them, almost nothing there it was almost like a saline shot and then there were Pfizer’s that were just packed with them and you just get the sense that the manufacturing of this is totally inconsistent…some were more concentrated and some were less.
This suggests that there was either very poor mixing when the vaccines were packaged (leading to some having lots of the lipid nanoparticles and others none) or that the vaccine manufacturers were unable to produce enough vaccine to meet the existing orders and switched to packing placebo vials to meet their contracted orders.
•Empty nanoparticles—in one NMR examination of 4 vaccine vials, it was determined that the lipid nanoparticles, but not the mRNA, were present in each of the vials. This suggests that the vaccine was not prepared in a consistent manner, or that the manufacturers ran out of mRNA to fill the vaccines with.
•A citizen’s investigation (which has since been replicated) discovered that bacterial DNA plasmids were present in the vaccine. This was a consequence of the vaccine production process being switched after the clinical trials to a more scalable one that used genetically modified bacteria to mass produce the DNA that served as the template for the vaccine mRNA and insufficient purification steps being taken to remove them.
Note: more dangerous vaccine lots were also found to have higher concentrations of the plasmids.
In short, from the start, I was relatively sure the vaccine doses were not the same (based on the observations I made) but I couldn’t explain why and hence considered a lot of hypotheses (e.g., different mRNA doses were being done as a large scale experiment). Now that the dust has settled, I believe the most likely explanation was simply poor manufacturing, which is by far the most benign explanation as it suggests many were spared from the severe consequences of these vaccines (as they received “duds”).
Note: inconsistent manufacturing is actually a longstanding issue, especially in products which are not subject to as rigorous inspection. For instance, since all vaccines are “safe and effective” and simultaneously immune to lawsuits, much less of an incentive exists to monitor the quality of their manufacturing. To illustrate, in 2021, Christopher Exley’s team found that the aluminum content of childhood vaccines varied greatly from lot to lot (and the vaccine’s label), which in my eyes is significant since aluminum is the primary agent responsible for vaccine injuries.
Vaccine Distribution
Prior to COVID-19, one of the things which was well known about lipid nanoparticles is that they distribute unevenly throughout the body. In turn, one of my biggest questions with the COVID-19 vaccines was exactly where they would be distributed throughout the body as if they concentrated in specific organs, this indicated they would be much more toxic to those regions of the body.
Once the COVID vaccines came out, in addition to the numerous accounts of heart attacks and strokes, I kept on hearing the same story again and again from my colleagues—the vaccines appeared to most frequently be targeting the pulmonary arteries, and less frequently splenic artery, the renal arteries and the hepatic artery (e.g., I’ve now met multiple people who developed a splenic infarction after the vaccine).
This really puzzled me since I had heard the exact same thing about COVID-19 and long COVID—it also targeted the pulmonary arteries (particularly the right pulmonary artery). In both cases, mechanistically this just didn’t make sense to me, but since numerous colleagues who I knew didn’t know each other were reporting this to me, I felt it had to have some degree of validity.
For reference, the pulmonary arteries bring deoxygenated blood from the heart to lungs:
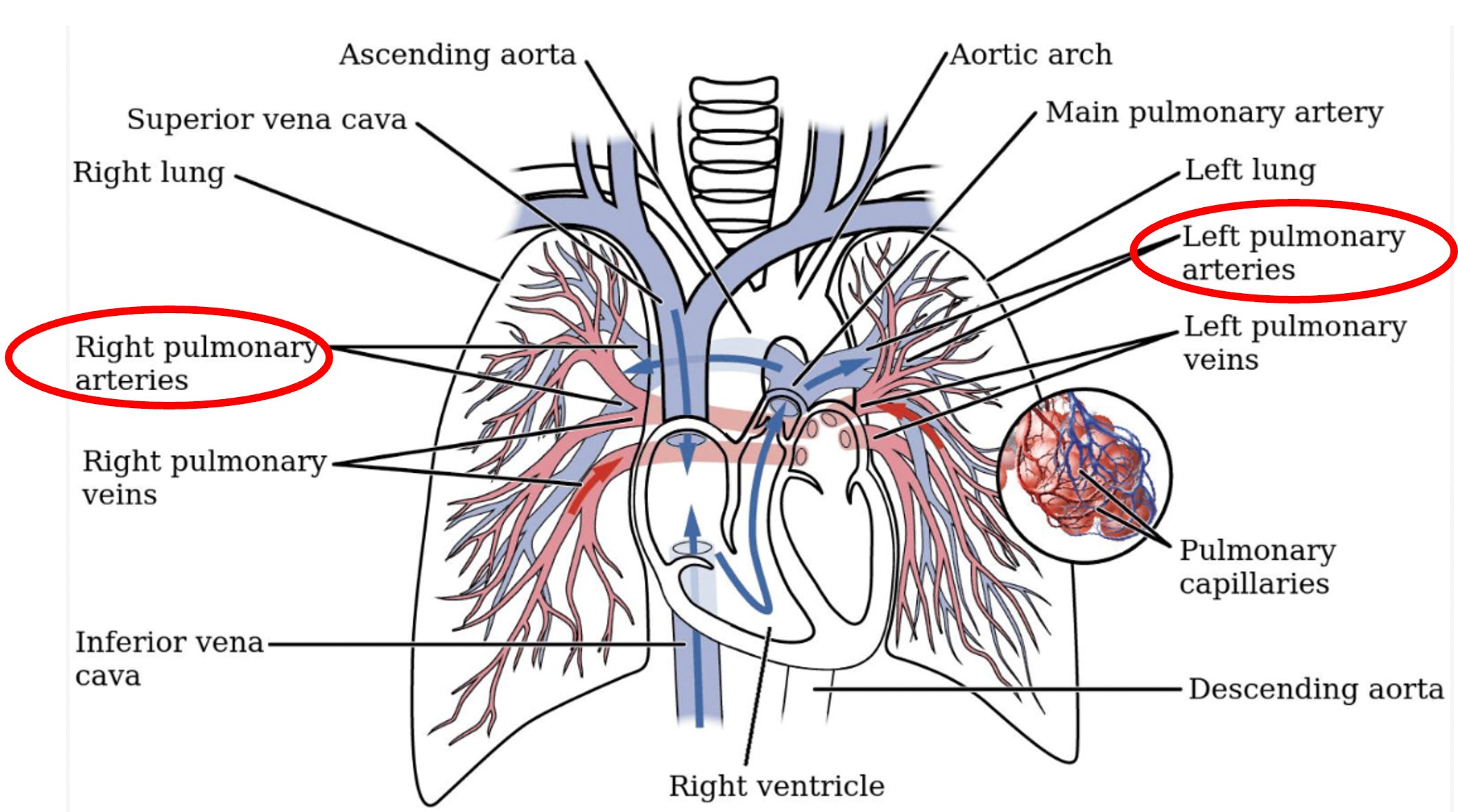
In the case of COVID, it seemed strange the virus would go to the pulmonary arteries since the blood flow out of the lungs (and hence where the virus should go) is through the pulmonary veins not the arteries. Conversely, with the vaccine from a circulatory standpoint, the only possible explanation I could think of for why the lipid nanoparticles (and their mRNA) might end up in the lungs was because the pulmonary vasculature was the first place that venous blood (which is likely what the injected vaccine feeds into) gets caught in a “sieve” and can’t travel further (hence why blood clots in the leg frequently cause potentially fatal pulmonary blood clots). Furthermore, since the right pulmonary artery, but not the left branches, I suspected that might explain why vaccine mRNA was more likely to hit the right pulmonary artery.
However, given that the circulatory explanations conflicted (as it supported the vaccine concentrating in the R. pulmonary artery but not a COVID-19 infection) I could see numerous holes with in this theory. Likewise, I would expect the vaccine damage to occur after the pulmonary artery, since blood (and clots) can still easily travel through this region of the circulation.
Alternately, since both the vaccine and SARS-CoV-2 shared the same spike protein, this made me wonder if the targeting of the pulmonary artery was because the spike protein had an affinity for that tissue. The most likely candidate would be the ACE2 receptor, so I then researched if the pulmonary arteries had a high concentration of the ACE2 receptor but found that while some of the existing research vaguely supported this theory, overall it clearly did not.
Note: the lungs (likely the kidneys) are known to have a high ACE2 receptor concentration. However, the spleen (which is also commonly affected by the vaccines) does not, which likewise challenges this hypothesis.
Since this was a rather confusing puzzle, I spent a while researching a variety of topics, such as the long forgotten Russian research which demonstrated that the heart has the ability to sort blood (e.g., fresh vs. old blood) and direct it to exactly where the body needs it.
Lipid Nanoparticles
One of the many design challenges with the COVID vaccines was finding a lipid nanoparticle which could safely carry the mRNA material into the cell. Many (e.g., Robert Malone, who spent years working with that technology) felt producing a safe lipid nanoparticle mRNA vaccine was impossible and eventually abandoned the approach. For instance to quote David Gortler and Robert Malone:
Many experimental cell culture studies performed over the decades since initial discovery suggest that these cationic [positively charged] lipids could be responsible for vascular damage, stroke or other toxicities associated with adverse events shown through various adverse event reporting databases. For example, published safety data sheets clearly state that the cationic lipids SM-102 and ALC-0315 are not for use in humans.
When I reviewed the leaked EMA files at the end of 2019, one of the first things I checked was exactly how the lipid nano-particles were formulated and the zeta potential of the final product—both because I was curious to see how they overcame this massive challenge and because I suspected the “solution” might predict the vaccine’s potential toxicity.
Note: I suspected the lipid nanoparticles were positively charged for three reasons.
1. They were made from cationic (positively charged) lipids (which was explicitly acknowledged within the EMA documents).
2. In some cases, individuals had heart attacks or strokes immediately after vaccination, which was a time frame where I did not believe it was possible for the mRNA to have already be producing enough spike protein for it to then leave the cells and create a cardiac event. This suggested something in the vaccine (e.g., the lipid nanoparticles) could already produce blood clotting—such as positively charged lipid nanoparticles collapsing the zeta potential.
3. I had seen numerous video under microscopes of the vaccine within seconds causing blood to clump together once it was mixed with it. This again argues against spike protein production causing that, especially since only white blood cells (which comprise a minority of the blood) can produce proteins from mRNA (red blood cells, the majority, can’t).
According to the regulator’s documents:
The zeta potential distribution for BNT162b drug product is narrow and monomodal. The average apparent zeta potential is around -3.13 mV, indicating the surface of the LNP is slightly negatively charged. The nearly neutral LNP surface supports the mechanism that BNT162b2 drug product avoids non-specific binding events in the blood compartment.
When I initially read this, I thought, that’s strange, I expected it to be the opposite. From reviewing that (and the rest of the documents), however, I realized there were a few key points I had not initially recognized.
First, the focus on the lipid nanoparticles appeared to be on efficacy, not safety, which led me to suspect it was quite difficult to make a lipid formulation which “worked” for the vaccine. As a result, I also suspected that if safety issues were discovered with the lipid nanoparticles, they were deemed to be a necessary trade off to make a “working” vaccine, and hence there might be some serious issues with the nanoparticles that were not being disclosed.
Second, while zeta potential is almost never discussed within medicine (which I believe is due to it opening the doors to a lot of awkward questions for the medical industry), it was mentioned in this document (due to zeta potential being a critical component for the vaccine to “work”). Furthermore, the final sentence of the above passage was a tacit admission that if the lipid nanoparticle’s zeta potential was different, it could cause issues.
Third, the language used to characterize it (“the average apparent zeta potential is around”) gave Pfizer a lot of wiggle room were a different zeta potential to later be discovered.
Furthermore, in the documents I also noticed they emphasized that all the lipid nanoparticles were “perfect.”
Screening studies were performed to confirm that the ALC-0315/ALC-0159/DSPC/CHOL at molar ratio 47.5/10/40.7/1.8 with a ratio of cationic lipid to RNA (N/P ratio) of 6.3 provide LNP with acceptable quality and stability. Physicochemical and biological properties were studied (density, viscosity, DSC characteristics). Moreover, size distribution and particle shape were studied showing a narrow distribution with a hydrodynamic radius and an almost spherical shape in the entire size distribution. The zeta potential was narrow and monomodal. The pegylated surface of the LNPs was studied showing consistence with the proposed LNP architecture: presence at the surface of PEG and hydrophilic head of ALC-0315.
When I compared everything I had observed to this passage, I hypothesized that the lipid nanoparticles weren’t “perfect” in real life, and instead many were somehow being composed of a much higher concentration of cationic lipids (e.g., due to them not being correctly formed or cationic lipids existing separate from their “neutral” nanoparticles).
Lipid Nanoparticle Distribution
Since this was an active area of focus for me, once it was released, I immediately reviewed a Japanese FOIA that contained the lipid nanoparticle biodistribution data for Pfizer’s vaccines.
I found this data quite interesting, as it validated a few things I’d seen (e.g., the previously mentioned spleen issues, the high rate of menstrual and fertility issues due to vaccine going to the ovaries, the periodic liver issues associated with the vaccine, and the bone issues I’d seen such as individuals developing multiple myeloma from the vaccine or existing bone marrow transplants failing). However, I simultaneously noticed, there were no indications in this data the lipid nanoparticles concentrated in the lungs.
Given all of this, I spent over a year being quite confused about the subject. However, a few months ago, I finally found the missing puzzle piece which tied everything together from a presentation by experts in the field of lipid nanoparticles (which I learned of from a Twitter thread a reader linked me to). Specifically, it was this slide (which referenced this study and this study):
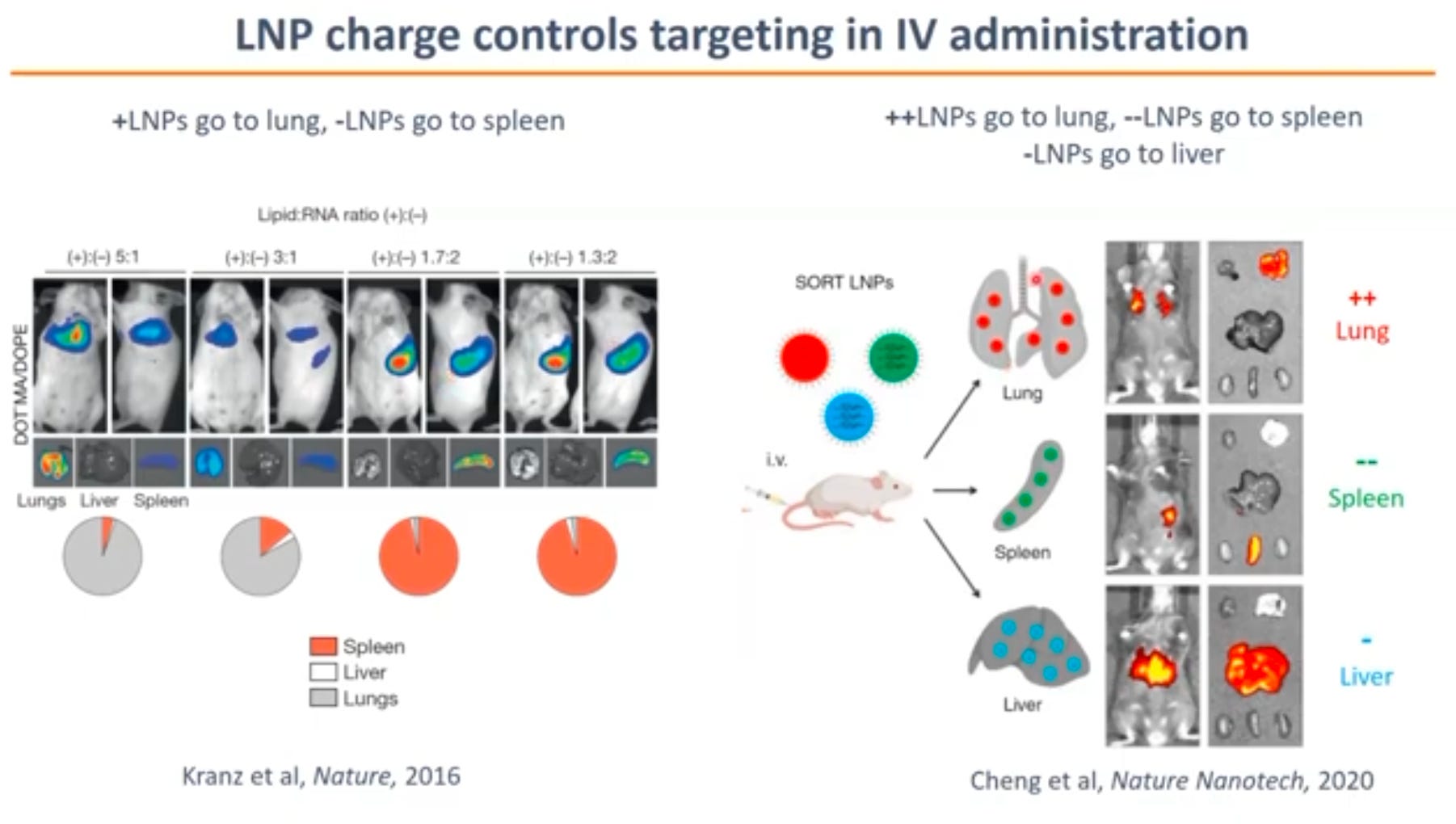
What this slide essentially says is that if lipid nanoparticles are positively charged, they will go to the lungs, whereas if they are negatively charged, they match the biodistribution data Pfizer provided to the regulators. Since my colleagues were consistently finding signs the vaccine was damaging the lungs, this suggested the lipid nanoparticles were instead positively charged.
At this point, I realized the quality control issues I’d noticed for the vaccine (and discussed above) must also apply to the lipid nanoparticles. Put differently, while Pfizer was able to carefully make high quality lipid nanoparticles in a carefully controlled setting which were “perfect” in form and slightly negatively charged (hence producing the biodistribution data Pfizer gave the drug regulators), once their production was scaled up, this was no longer possible to do and a high degree of variability then emerged in the particles.
For instance, I previously shared the NMR data which found the lipid nanoparticles in four vaccines that were examined had no mRNA in them. This results in very different lipid nanoparticles (as there is no negatively charged mRNA to interact with the positively charged lipids). This likewise suggests that some of the lipid nanoparticles had a much higher ratio of cationic lipids to mRNA than was intended.
Likewise, in the EMA documents, it was acknowledged that there were stability issues with the lipid nanoparticles which almost certainly would have come into play once production was scaled up and the storage of the particles could no longer be assured:
The PEGylated lipid ALC-0159 is preferably inserted at the LNP surface as a steric barrier to interactions with surfaces or other LNPs to avoid aggregation during storage.
Additionally, surface area is considered critical to avoid aggregation both during storage and with serum components in vivo. The ratio cationic lipid to RNA (N/P) is also critical for formation of LNP. An access [excess?] of cationic lipid is required and a ratio of about 6 is found reasonable.
The DP is stored frozen at the recommended storage temperature of -90 to -60°C. Stability studies are ongoing for the determination of DP shelf-life, see section P.8.
Quality Control
Throughout Operation Warp Speed, everyone’s focus (e.g., that of the media, the pharmaceutical industry and the drug regulators) was on getting the vaccine made, not ensuring that it was safe or effective.
For this reason, it became acceptable to mass produce a fairly non-understood technology and simultaneously cut corners on each step in the process so its orders could be filled in time to win the race to produce the first vaccine (e.g., in hindsight it’s almost comical those tested lipid nanoparticles didn’t have mRNA in them and many other vials were simply saline).
Likewise, it was known since early in the COVID-19 vaccine roll-out (due to VAERS) that different vaccine lots had radically different toxicities, which in turn showed the vaccines were not following the basic standards (e.g., good manufacturing processes) drug regulators always enforce for pharmaceutical products.
In short, I believe by far the most plausible explanation I’ve seen for most of the issues with the COVID-19 nanoparticles was simply poor quality control. This in turn I believe was made possible both by the global climate of fear which the media created around COVID-19 and the increasing tide of corruption within the Federal Government.
Conclusion
During COVID-19, many were presented with each of these choices:
•Should I isolate myself from the world to “avoid” COVID-19, or should I live my life and accept the risk of getting COVID-19?
•If you get COVID, should you risk going to the hospital or try to treat it with an allegedly effective treatment at home?
•Should you get an experimental vaccine or risk getting a severe case of COVID-19?
•If you will be fired for not vaccinating, is the risk of being harmed by the vaccine enough to take on the economic consequences of being fired?
In each case, one was required to make a difficult (and high stakes) choice in the face of uncertain information. Now that the information is much clearer (in all cases the former choice was “wrong”), it’s easy to judge those who made the “wrong” choice, but I believe it’s critically important to remember how different things were back then when much less of this scam had been exposed.
In turn, I would argue the people who went against the narrative at that time had the following in common:
•The courage to break from the herd and to be willing to take on the risk of making the “wrong choice.”
•A willingness (or eagerness) to work with uncertain information rather than becoming paralyzed by the ambiguity over what the right thing was to do.
•A mental flexibility that allowed them to change their position once it was no longer supported by the existing evidence rather than obstinately doubling down on the position they had already committed to and psychologically invested themselves in.
In the years to come, I expect we will face many more perilous trials where it will be critical to correctly navigate an unclear and immensely complex situation. In this article, I tried to share a few examples of how I have done this over the last few years in the hope they can provide some insights for you on how to do this as well.
In the second part of this series, I will explore one of the most puzzling questions we have faced, vaccine shedding, and build upon the ideas laid out in this article (along with a few others) as I feel they can shed an important light on this mystery.
Finally, I would like to thank each of you for your continued support of this publication (each of you makes my work here possible). I never imagined there would be so much receptivity to the forgotten sides of medicines I’ve tried to share here, or how many people it would affect (e.g., a few days ago RFK Jr. shared an article from here which was has now been seen by over a million people). Thank you.
What you're describing here, AMD, is demoralization writ-large: the inability to make good choices because the well of human experience has been deliberately contaminated in order to generate an ubiquitous atmosphere of fear, uncertainty, dread, and doubt which drowns out the ability to critically look at and think about a situation while drilling in hatred for those who see through and do not play along with the PSYOP (those who don't wear masks, or vaccinate, and take horse goo, etc).
None of this is surprising as with Obama's repeal of the Smith–Mundt Act, DARPA has been running nonstop PSYOPs on Americans for a decade and Washington DC has devolved into a propaganda giga-factory.
"You just have to flood a country's public square with enough raw sewage. You just have to raise enough questions, spread enough dirt, plant enough conspiracy theorizing that citizens no longer know what to believe." —Obama https://bitchute.com/video/71n5A6wu76D6 [44 seconds]
Ultimately, they want us dazzled. They want us at each others throats. They want us to lose all faith in the system and believe that there is nothing left worth salvaging. And they want us view each other as the enemy so that we ravage one other with maximum prejudice.
Meanwhile they will sit back, watch, and eat ze popcorn as the last bulwark against their dominion over the world - The United States of America - brings itself to ruin in a blaze of hatred and violence.
Don't fall for it: https://tritorch.substack.com/p/dancing-doctors-unclean-lies-unchained
You are an excellent researcher, prolific writer, eloquent communicator, epic hide-n-seek player, but this expresses exactly why I admire you: "more importantly because I do not want my focus and energy going to the something I do not believe benefits my soul or the world around me." It's all about soul. . .