

How DMSO Cures Eye, Ear, Nose, Throat and Dental Disease
Many of those "incurable" conditions respond remarkably to DMSO

•DMSO can often significantly improve one’s vision, treat conditions such as macular degeneration, retinitis pigmentosa, and at times allow blind individuals to regain their sight. It is also often very helpful for sore and strained eyes and relieves excessive irritation and inflammation, along with many other eye conditions (e.g., cataracts).
•DMSO frequently treats a variety of ear conditions such as tinnitus, hearing loss, airplane ear, and a variety of infections inside the ear (e.g., otitis media).
•DMSO often is very helpful for sinusitis and a variety of infections of the nose and throat. Likewise, it is extremely helpful in dentistry, both for cleaning the mouth (e.g., by preventing bleeding gums), and by allowing the mouth to rapidly heal after dental surgeries.
•In this article, I will review the evidence supporting each of those uses, along with the data demonstrating the safety of these methods of DMSO administration and instructions on how to do them.
DMSO is a phenomenally effective medicine that can treat a wide variety of common, debilitating, or incurable conditions, which allowed it to rapidly take the country by storm (as both the public and the medical community saw its results and rapidly embraced it). Unfortunately, the widespread enthusiasm behind something that completely changed medicine and allowed people to care for themselves independently was unacceptable to the FDA. For the next two decades, the agency went to incredible lengths to suppress it (e.g., it actively defied Congress for over 16 years) and eventually made DMSO become a Forgotten Side of Medicine.
Note: extensive data shows that DMSO is a very safe substance with negligible toxicity.
In turn, one of the truly ironic things about this was that many of those who attacked DMSO later needed it. For example, the pioneer of DMSO discusses how Former President Lyndon Johnson sought his help in 1971 —after his FDA commissioner had just spent almost three years weaponizing the FDA against anyone wishing to use DMSO (which in turn set the stage for many of the police-state tactics the FDA would illegally use against natural medicine in the decades to come).
Note: in the previous article I erroneously stated this conversation took place in 1981 not 1971 (at which point LBJ was deceased).
I have now received hundreds of unbelievable reports from readers (which can be read here) of what DMSO did for them—many of which are almost identical to what people reported fifty years ago before the FDA wiped DMSO off the map.
For context, the majority of those reports were for the most common uses of DMSO, such as chronic pain, acute injuries, and arthritis (discussed further here). However, as discussed here, DMSO is also immensely valuable for a variety of circulatory and neurological disorders (e.g., varicose veins, hemorrhoids, Down Syndrome, and Parkinson’s)—all of which readers here reported significant improvement from. Likewise, (as discussed here) DMSO also helps various autoimmune conditions.
In this article, I will focus on another group of conditions DMSO was found to be extraordinarily effective—those within the head.
Note: headaches were covered in a previous article and will not be discussed here.
Cause or Effect?
There are two common ways to view medical problems someone has—as a specific disease process of a particular part of the body or as one manifestation of a systemic issue. Neither approach is entirely correct, as in some cases, you need one more than the other, but our medical system is very much biased towards the first one.
This, I would argue is in part because this makes medicine easier to practice (e.g., a specific set of symptoms goes with a specific drug rather than having to go the extra mile to figure out what is causing a nebulous set of symptoms), and in part because it makes it possible to sell far more patentable medicines (as by viewing each symptom as a different disease, far more diseases exist to market products for). Unfortunately, this also frequently lends itself to a situation where modern medicine “treats the symptoms rather than the cause.”
I personally believe that most chronic disease processes can have a variety of ways they manifest throughout the body. Typically the manifestation you see is a result of a pre-existing weakness in the body being the first spot to give out after a stressor is put on the entire body (e.g., one of the most common symptoms individuals with COVID vaccine injuries had was a pre-existing site of minor inflammation or an old scar becoming highly inflamed). Similarly, I believe this paradigm answers a critical question medicine never quite addresses—why do some people get so sick from the same thing that others quickly shrug off?
In turn, I’ve tried to focus on the forgotten areas of medicine that I believe often underlie various seemingly unrelated disease processes. For example, I believe that microcirculation is critical for health, but since it is not easy to measure, our focus instead has gone to blood pressure—which while sometimes useful for determining circulatory health, often is not. In turn, I’ve provided a variety of strategies for improving the microcirculation (e.g., improving the physiologic zeta potential). Beyond cardiovascular health improvement, many readers here who did that reported a variety of other chronic symptoms also having noticeable and unexpected improvement.
Note: all the previous also holds true for the cell danger response—a defensive mechanism cells go into where their mitochondria shut down that can only be treated by finding a way to coax the mitochondria out of it.
DMSO is also a systemic agent that has the ability to address some of the common root causes of disease. Because of how dramatically it helps injuries, arthritis, and chronic pain (of which I’ve received many remarkable testimonials from readers you can read here), those are its typical uses. However before long, many patients on DMSO would report some other chronic issue they never thought could improve also begin getting better (which likewise, many readers here have noticed). These reports caused the early pioneers of DMSO to begin researching other novel uses of DMSO.
In this article, I will look at the variety of remarkable benefits that have been observed for DMSO for conditions within the head. These results, I believe are a product of DMSO:
•Being able to increase microcirculation and treat circulatory or neurological disorders(e.g., strokes, traumatic head injuries, spinal cord injuries, and dementia or mental disability).
•Being able to re-awaken cells that were dormant or on the verge of dying due to a previous stressor.
•Being able to increase parasympathetic activity.
•Having strong anti-inflammatory properties.
•Having anti-bacterial properties.
•Being able to easily pass through biological membranes without harming them and spread throughout the body (while also carrying anything mixed with it into the body).
DMSO and the Eyes
Many DMSO users have noticed that their vision improved while they used it for something else (e.g., see this, this and this testimonial from a reader here), which in turn inspired physicians to begin applying it to the eyes of patients with vision problems.
Note: to my knowledge, every route of administration for DMSO except intrarectally has been researched. Of these, the only one that ever caused issues was nebulizing it (as rats who regularly breathed DMSO eventually developed toxicity). As a result, the DMSO field has recommended against nebulizing it, although I periodically read cases of individuals who had a positive response to nebulized DMSO
Ocular DMSO Distribution
The logic behind putting DMSO in the eyes is that a much stronger dose can get to the eyes than what would arise from systemic applications of DMSO. To evaluate DMSO’s distribution (and that of its metabolic breakdown products), radioactive forms of DMSO (DMSO synthesized from either 35S or 3H or both) were placed in animals and then their entire bodies were monitored for radiation emissions.
In one study, it was noted that while DMSO tended to distribute evenly throughout the body (typically being at a lower concentration in the tissue than in the blood), in the iris and ciliary body, it matched the blood’s concentration, while in the cornea (the surface of the eye), after 2 hours it was 2.2 times higher than the blood in rabbits and 4 times higher in rats. In other words, DMSO specifically concentrates in the cornea when administered into the body (after which it rapidly cleared), suggesting that DMSO is indicated for treating corneal and uveal diseases.
Note: concentrations did not increase with repeated administrations (indicating DMSO does not accumulate in the body).
More importantly, that study helps to explain why consuming DMSO can often directly impact and improve eye health.
Conversely, in another study, rats eyes were exposed to DMSO, and it was found regardless of the route of administration or the concentration used, DMSO rapidly cleared from the eyes:
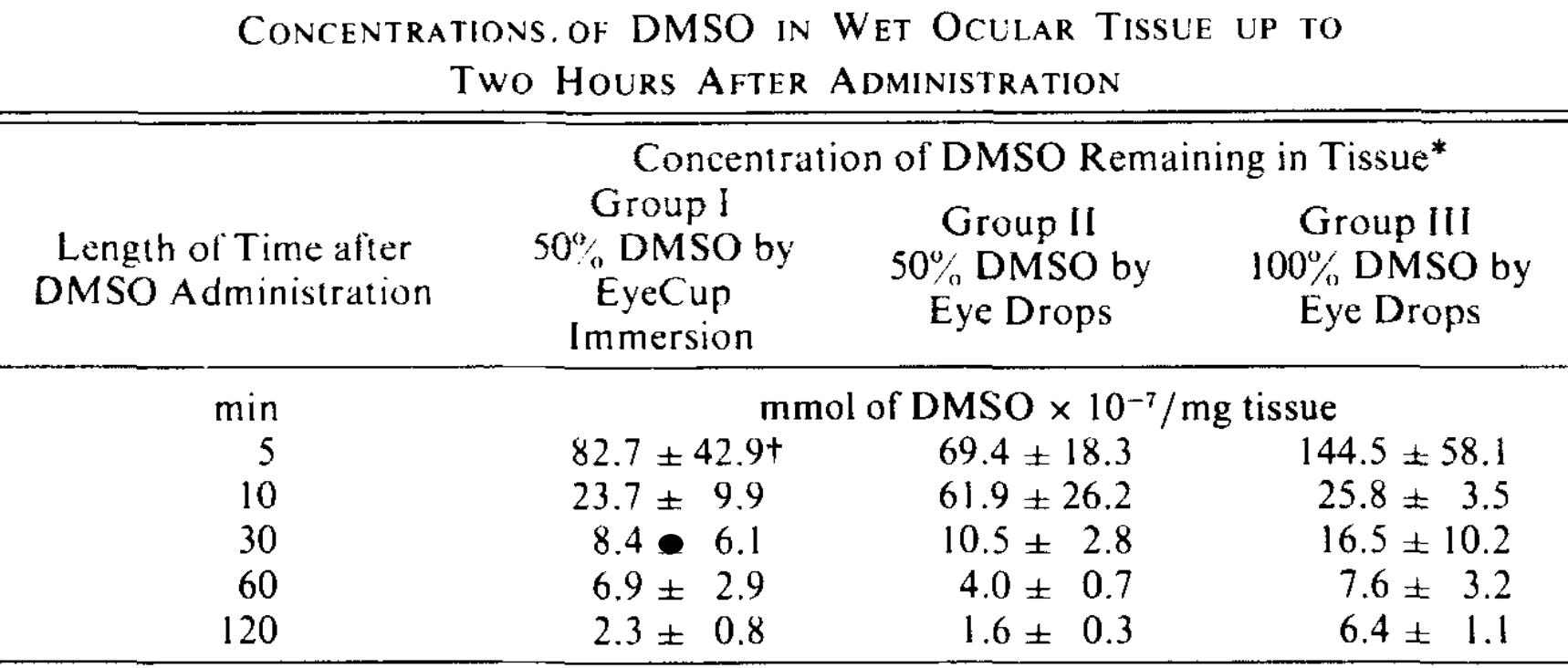
This in turn, suggests that DMSO can rapidly extract things from the eyes that should not be there (e.g., excessive fluid) as whatever is in the eye will be drawn out into the rest of the body with the DMSO that leaves the eyes.
Note: DMSO has also long been used to preserve corneas, which will be transplanted to someone else, again indicating that DMSO is relatively non-toxic to the cornea.
DMSO Eye Safety
Since the idea of putting DMSO into the eyes understandably makes one uneasy, I’ve tried to locate all the safety data relating to this. Regarding the systemic administration of DMSO, there was a longstanding concern that DMSO could (temporarily) change the refractive index of the eyes. This finding was found in certain animals at very high doses of DMSO but never, despite extensive evaluation, found in monkeys or humans (e.g., see this study). For those interested, I summarized all the data on DMSO induced lens changes here, and the most detailed summary I found of exactly what changed in animal lenses can be found here.
Note: in humans, when DMSO was taken each day at 3-30 times the standard dose (achieved by covering the entire body in DMSO), 9% of participants experienced burning or aching eyes. This (like the previously mentioned effects) I suspect is due to the fact DMSO will concentrate in the cornea, but at the same time, realistically will never be an issue for a DMSO user because the effect only appears at very high doses (and has no real consequence besides the temporary irritation).
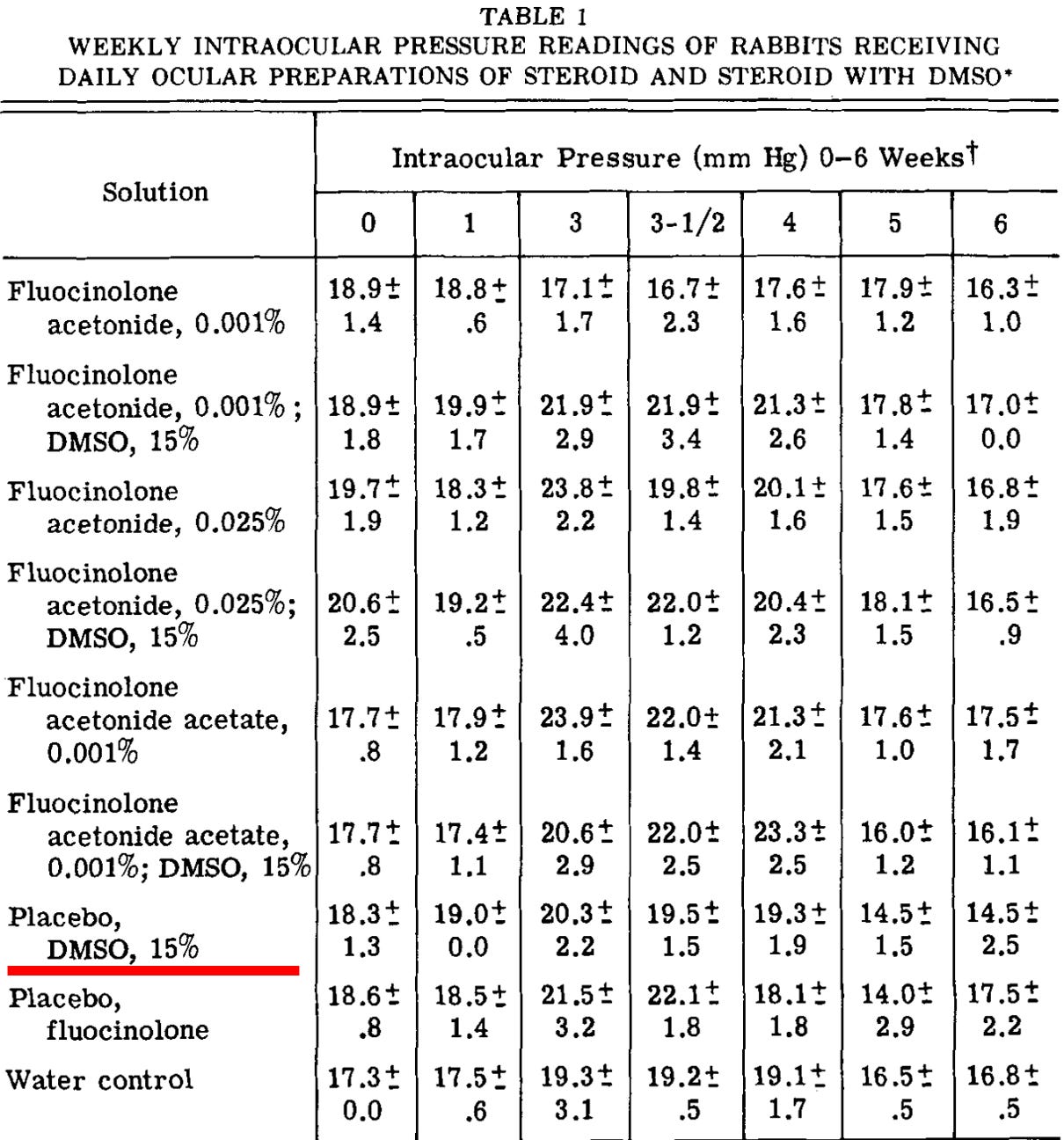
A few animal studies have been conducted which evaluated the effects of applying DMSO directly to animal eyes. The most detailed study put various combinations of steroids, 15% DMSO, or a saline placebo into rabbit’s eyes. A wide range of parameters inside the eyes were studied (e.g., regular body weights, intraocular pressure, retinoscopy, ophthalmoscopic, and biomicroscopic examinations alongside dissection of the eyes and examinations of their contents) alongside ones outside the eye (e.g., urine volume, urine composition, blood work, autopsies of organs) were then assessed. From this, it was found that 15% DMSO created no adverse effects, but did:
•Increase urine volume—DMSO alone increased it by 14.6%, while when added to varying concentrations of fluocinolone acetonide (a steroid), it increased by 4%, 29%, or 58% (which again illustrates that DMSO moves into the bloodstream after being applied to the eyes).
•Cause a slight decrease in urea in the aqueous humor of the eyes (which was small enough that it may have been due to chance).
•Decrease intraocular pressure (which is often quite helpful for the eyes).
Additionally, this study also applied 30% and 100% DMSO to rabbit eyes. In both cases, no evidence of change was seen in any part of the eye (the iris, cornea, lens, retina, conjunctiva, and lids), but 100% DMSO was observed to cause temporary lacrimation (tearing).
A separate paper on the known toxicology of DMSO also noted that:
•A Draize eye test (applying DMSO to an animal’s eye and keeping it on the eye) resulted in a slight conjunctivitis (eye irritation) which disappeared after 24 hours.
•One study found ocular instillation of 0.1 ml of 100% DMSO in rabbits caused reversible irritation of conjunctivae, while another author failed to observe this effect.
•Administering high doses of DMSO to rats (14.5g/kg) through the air resulted in hyperemia and eye inflammation.
.
•In humans, two drops of greater than 50% DMSO applied to the eye caused a temporary burning sensation and vasodilation; concentrations of less than 50% exhibited no toxic effects.
Another study found that DMSO gave eye drops at 66% concentration to four patients, and one of the four experienced a temporary burning each time the drops were applied. Likewise, varying degrees of irritation and burning occurred as higher concentrations were used. However, no damage (as shown by a fluorescein stain) occurred to either their eyes or the animals in the study after ocular DMSO applications.
That same study also gave 4 rabbits 90% DMSO to the eyes six times a day, and then after 2 weeks, DMSO at 66% six times a day. At 90%, 2 of the rabbits experienced a temporary severe conjunctival injection (red eyes from swelling and inflammation of the blood vessels in the eye), but no keratitis (inflammation of the cornea) or damage to the lens was observed, and of the 6 total rabbits who received ocular DMSO, 3 had some degree of conjunctival irritation from DMSO.
I will now discuss two human studies that evaluated both the safety and efficacy of applying DMSO to the eyes, both of which found no toxicity from doing so.
DMSO and Eye Inflammation
One study reported giving topical DMSO to 108 patients (for a total of 157 eyes) at a higher concentration than others used. That author noted that no toxicity or eye issues were observed, including in patients with pre-existing eye issues (e.g., 8 glaucoma patients who frequently had their intraocular pressure rise when given a steroid did not have it rise from DMSO and likewise 17 patients with pre-existing cataracts did not have them worsen from DMSO).
In that study, of the 43 whose results were listed in detail, 3 had improved vision (including one who was blind prior to DMSO treatment). Additionally, 4 severe cases of episcleritis (which had previously failed to respond to the use of corticosteroids) all responded to DMSO topically, and 4 cases with chronic corneal edema all exhibited some improvement on this regime. Other types of eye inflammation were also studied (e.g., conjunctivitis, keratitis, and uveitis). Still, the therapeutic response was more varied, leading to the investigator concluding more standardized approaches needed to be developed to assess DMSO’s benefits.
Note: somewhat similarly, I received a report of a dog that developed an eye ulcer from a scratch, making the dog blind, and a veterinarian wanting to remove the eye to spare the dog from further suffering. The owner however, went against the vet’s advice, and after a month of applying DMSO, it was cured and the dog’s sight returned.
Note: DMSO has also been used in conjunction with antibiotics to eliminate organisms from the anterior segment of the eye from patients with inflammatory eye diseases, to treat inflammatory diseases of the eyelids, and when combined with monomycin to treat corneal burns.
Retinitis Pigmentosa and Macular Degeneration
Retinitis pigmentosa (RP) refers to a group of genetic disorders that cause gradual vision loss (starting in the periphery). It results from rod cells in the eyes not secreting a substance that prevents cone cells in the eye from dying (through apoptosis). It affects 1 in 4,000 people and is thought to be incurable, with the exception of one subtype of RP (comprising between 0.3-1.0% of cases), which has a $850,000 gene therapy that works about half the time (although others are in the pipeline).
Since RP is “incurable,” it immediately caught a few doctor’s attention that their patients with it had their vision improve while receiving DMSO for something else. This prompted a series of clinical studies a preliminary 1973 investigation that found DMSO did indeed help this condition.
That author then published a larger 1975 study where he shared:
When his DMSO treatment was started (February 10, 1972), this patient could see hand motion only with his right eye, and had a visual acuity of 20/200 (Snellen) in his left eye. Five days later (February 15, 1972), his vision was measured as 20/70 + 1 in the left eye, and he could count fingers at 5 ft with his right eye. Three months later, his visual acuity was 20150 in the left eye. This patient has continued his treatments daily, except for a 1-week trial interval without DMSO. He noted that his vision began to get worse during this interval, and when he restarted treatment, his vision returned to the level he had just before discontinuance. His most recent visual acuity measurement (January 2, 1974) is still 20/50 in the left eye, and he is able to count fingers at 6 ft with his right eye.
Following this, 50 more patients with RP or macular degeneration received DMSO applied to the eyes, of whom 22 had improved visual acuity, 9 had improved visual fields, and 5 had improved dark adaption, 2 continued to worsen, while the rest noticed no changes in their vision (which could potentially mean DMSO stopped the degenerative process).
To evaluate for toxicity, the eyes were examined through serial fundus photography and slitlamp photomicrography, and no adverse tissue reactions were noted. Patients often reported temporary stinging (usually 20 to 30 sec) and occasional burning and dryness of the skin of the lid (likewise a reader here reported when applying DMSO to the eyes, they have a temporary stinging which quickly disappears, while another reported no issue with using a DMSO eyewash).
Additionally, patients in this study also reported a “glare or blur effect” in their vision that was often accompanied by an increased sensitivity to light, or photophobia. This typically lasted for a few days to weeks, after which it disappeared and was replaced with an improved ability to get around at night, and improved visual acuity experienced as better perception of contrast.
The author also stated they had initiated a controlled clinical study and were in phase III clinical trials with the FDA (which is where the above data originated from), but I could not figure out what happened to it.
Note: the author of that paper suspected that DMSO was helping here by rescuing dormant cells in the eye which would otherwise eventually die.
Conversely, a follow up controlled study was unable to detect a clear benefit for DMSO in patients with retinitis pigmentosa, did find a complete lack of toxicity from applying DMSO to the eyes.
Human Case Studies
In addition to those two studies, a variety of individual case histories support DMSO’s value for the eyes.
One author reported on DMSO being used by Stanley Jacob for more severe cases of eye damage such as:
•A man who had been blind for more than 30 years after having dynamite explode in his face who started seeing flashes of light after applying DMSO to the head.
•A man who lost sight in the right eye (along with other functions of the eye like focusing) and gradually lost it in the other after an almost fatal impact by an automobile while skating down the road. After trying DMSO for hair loss, he noticed a sensation in the back of his right eye, so Stanley Jacob decided to try applying DMSO to that eye, eventually settling on a high concentration (that stung for several minutes, caused tears, and left the eyes bloodshot for about 20 minutes). After this, sight rapidly returned to the right eye.
•A man who had been blind for many years in one eye (only able to distinguish light and dark) regained his sight in that eye with DMSO (e.g., he demonstrated this by walking unaided in public areas and describing objects and events while his good eye was covered).
•A man who was almost blind (leading to him being completely dependent on others like his wife to take him anywhere, cut his meat or keep his house clean) after a year on DMSO regained his sight and no longer needed assistance to do anything (which was of great relief to his family).
Note: these results led to Jacob testing DMSO on a series of patients with incurable blindness. Sadly, in many cases (which ophthalmologists had pronounced incurable), regardless of the remarkable results, the ophthalmologists tended to insist there was either no improvement or it was just a coincidence.
Ophthalmologist Norbert J. Becquet, M.D., of Little Rock, Arkansas, reported to the American Academy of Medical Preventics (AAMP) in May 1980 that he had great success using DMSO in treating cataracts and other eye problems. "I've treated two hundred patients in the last year for macular degeneration, macular edema, and traumatic uveitis…In using DMSO, glaucoma drugs are potentiated, including those required for treating wide-angle glaucoma. But DMSO alone is better for macular degeneration.
Note: AAMP is now called ACAM, and other ACAM physicians at that meeting also stated that DMSO treats cataracts and glaucoma. Additionally, in a recent article, I discussed DMSO’s value for treating uveitis (so it will not be discussed here).
Another author who has worked with many doctors using DMSO reported that they’ve found applying DMSO to the eyes seems to help with a variety of vision issues and eye pain, and that typically, there will be a stinging sensation for 30-40 seconds after applying DMSO to the eyes, after which the eyes typically feel better than before treatment. Likewise, he also cited a Los Angeles doctor who had several patients who were able to read fine print more easily after only one week of applying DMSO to their eyes.
Note: that author also frequently applies DMSO to his own eyes when they feel tired and notices an immediate and rapid improvement. Likewise, one reader here who started taking DMSO for Parkinson’s noted they had less discomfort due to more eye irrigation.
In one case he cited, a 90 year old man who was unable to read (due to macular degeneration and other eye problems) who was treated daily with DMSO eye drops (along with oral DMSO) and after a month, could resume reading his books (along with thinking more clearly, and his whole body feeling better).
In another case, a 78 year old man had a variety of eye problems that were making it difficult for him to walk around his home. His doctors told him that since there was nerve damage to his eye, nothing could be done, and he should not waste his money on any unproven treatments. However, that man decided not to give up and convinced another doctor to try applying DMSO to his eyes (along with oral DMSO). At the start, he was 20/200, then in two weeks 20/100, two weeks after that 20/70, and then eventually 20/50 with glasses, allowing him to regain his independence (which persisted along with him being in excellent health for a man in his 80s).
Similarly, a reader here who had always been nearsighted reported that after taking DMSO internally for a few months, they stopped being able to see clearly through their glasses and then realized their vision had normalized (e.g., they could see the smallest print quite clearly) and had not needed reading glasses since.
Another author reports that patients on DMSO sometimes report an improvement in their eyesight as an unexpected but pleasant side effect (e.g., he cited a woman no longer needing her glasses the morning after she took DMSO). He found DMSO was often helpful for macular degeneration.
Note: the most common terminology for this condition (age-related macular degeneration) is AMD. Had I realized at the start that this was also the abbreviation of “A Midwestern Doctor,” I would have chosen a different name (and likewise, that is why I always refer to the condition as macular degeneration rather than AMD).
That author reported success using DMSO to treat eye conditions such as, macular degeneration, macular edema, uveitis (inflammation of the middle structures of the eye) due to trauma, cataracts, glaucoma, and various retinal diseases.
In turn, many DMSO doctors would use DMSO for perplexing eye conditions when they weren’t sure what to do. Likewise, readers here have reported that DMSO helped with a variety of other challenging eye conditions. For example:
•A firefighter injured his upper eyelid after some hot tar fell on it, which caused chronic inflammation that did not respond to any treatment from his doctor. After 10 years, he tried topical DMSO, and within a week it was gone forever.
•A reader has a very rare condition (less than 200 cases have been reported) that causes the eye to randomly spasm and jump all over the place (which makes it very difficult to drive) and is thought to be linked to migraines or concussions (both conditions I associate with impaired blood flow in the head). It’s considered to be essentially incurable, but after reading this series, he decided to try using DMSO applied as an eye drop and found it would stop the episodes.
•One reader who found DMSO helped many other symptoms they had, began applying DMSO drops to the eyes because they had symptoms of a vitreous detachment (floaters and flashes), and afterward noticed that they had less floaters and flashes, resulting in a clearer field of vision.
DMSO and the Ears
To establish the safety of DMSO in the ear, a study gave the eardrums of 10 volunteer prisoners five drops of 50% DMSO (in water) or 60% DMSO (in glycerin) three times per day for 74 days. During each application, they first laid on their side (with the ear facing up) for 15 minutes, then had a cotton plug placed in the ear so they could stand up but not have the DMSO leak out (which was then removed an hour later). Various tests and examinations were performed, and no signs of toxicity were detected besides a transient decrease in white blood cells (which regressed on its own and may have been related to a circulating infection in the prison). Once that study established the safety of putting DMSO directly into contact with the ear’s tympanic membrane, a variety of other studies were conducted utilizing a similar approach.
Note: a 2014 rat study found that applying 1% DMSO to the middle ear did not cause any adverse changes to the inner ear, while a zebrafish study found DMSO did not injure the hair cells in the ear.
Impaired Hearing
I believe poor hearing often results from impaired circulation to the ear, and in turn, you will sometimes encounter people who report their hearing improves as a side effect of DMSO usage. For example, after reading an earlier article about how to use DMSO to heal circulatory disorders (e.g., strokes) and starting oral DMSO, this reader reported:
Within 5 days several things were noticeable a) I pass water far more easily, b) my hearing accentuated, c) my eyesight improved somewhat, d) my mind was that much sharper and e) my blood pressure dropped from 160/90 to 150/80 and I just sense my heart is that much better.
Likewise, I recently spoke to a friend of Stanley Jacob who told me that he had success in treating hearing loss with DMSO and that they vaguely remembered Jacob had also treated cases of tinnitus with it.
Tinnitus
Like macular degeneration, most of the treatments I have come across that help tinnitus also improve circulation to the affected sensory organ. Additionally, I have seen many signs suggesting tinnitus is linked to excessive sympathetic activity (e.g., many other treatments I’ve seen help tinnitus address this component of the disease), which again argues for DMSO’s role in this condition (as by being an acetylcholine esterase inhibitor it increases parasympathetic activity).
While numerous patients with tinnitus have reported DMSO helped them (or their tinnitus improved incidentally from DMSO), I only know of one study that formally evaluated it.
In it, fifteen patients with tinnitus of unknown origin were selected for a study (while 2 hearing voices and 3 with tinnitus preceded by acoustic trauma or an aneurysm of the internal carotid were excluded). Each had tinnitus for a prolonged period (6 months was the shortest amount of time) and had not been able to adapt to the noise. At baseline, their characteristics were:
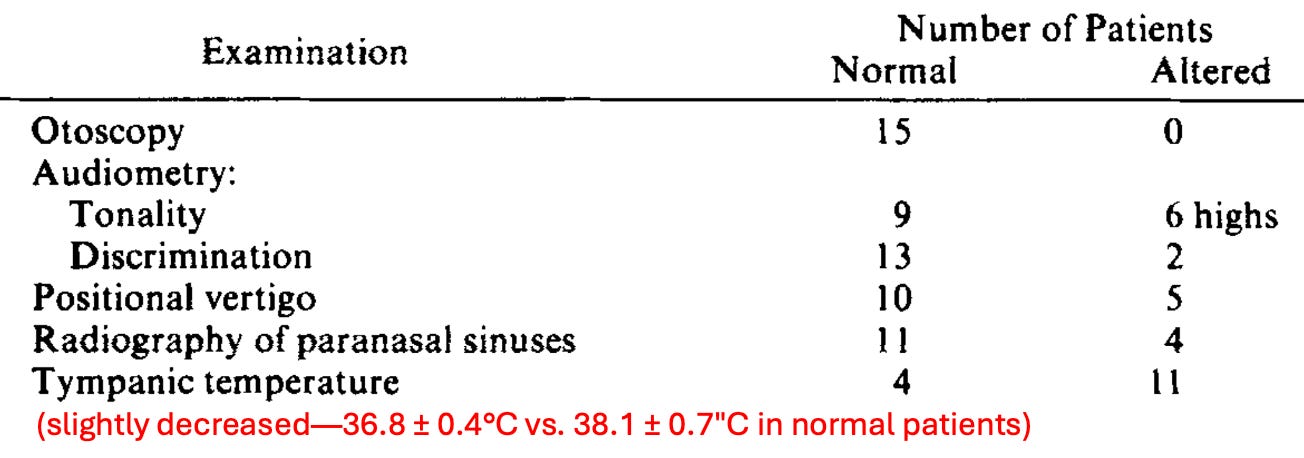
Note: in 3 cases, the ear ringing was localized approximately between 3,000 and 4,000 Hz, with an intensity of between 15 and 30 dB. In 12 cases, it was masked with a "white" noise between 10 and 12 dB.
Following one month of receiving a spray with DMSO and a few other drugs, all significantly improved.
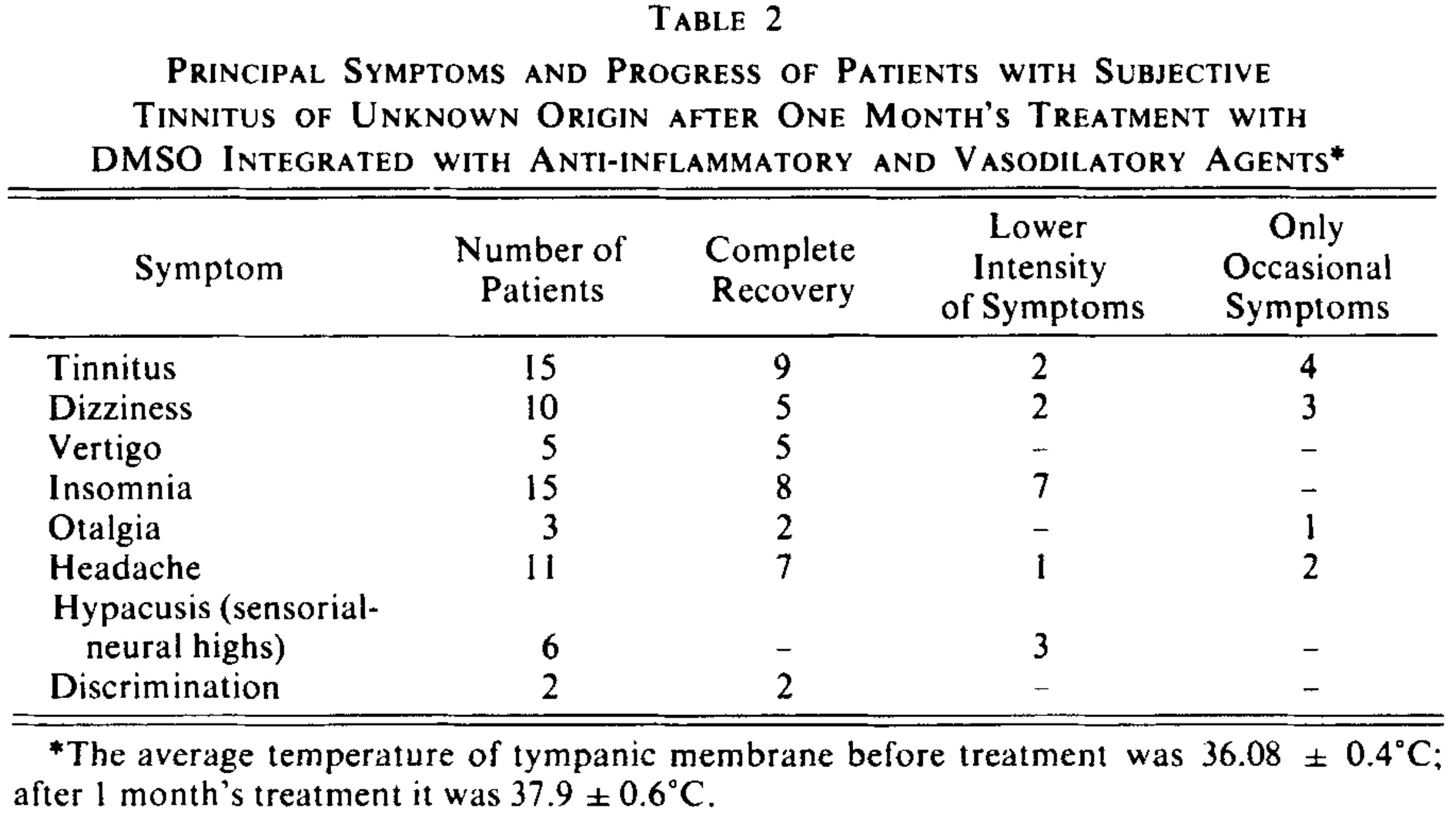
Note: this improvement was sustained for at least a year.
The increase in tympanic membrane temperature coinciding with an improvement of tinnitus made the investigators suspect poor blood flow (which DMSO improves) was linked to tinnitus. Likewise, in the four patients who only had occasional symptoms, they reported their symptom reoccurrence was tied to exposure to cold weather in the morning, further strengthening the circulatory hypothesis. Additionally:
A notable improvement was observed in the patients who at the beginning of the treatment had suffered from dizziness and positional vertigo. The insomnia of eight patients disappeared, and seven slept better. There was also improvement in headache and otalgia (the latter was not related to temporal-maxillar articulation). Very noteworthy was the modification in the sensorial-neural hypacusis of some of the patients, as expressed subjectively by the patients and confirmed by audiometric examination.
Note: at the 1974 symposium, this author also presented a paper on how DMSO could be used to treat hearing loss.
Another author reported on a clinic in New York City that treated a number of tinnitus patients with DMSO. They noted that in most cases, their ear noises were immediately reduced with DMSO, and that in most cases, the patients were permanently cured within a month, and if it recurred, a second course of DMSO would typically eliminate their tinnitus much faster than the original treatment. Additionally, in many cases, the patients did not report they had tinnitus until they shared that systemic administration of DMSO had improved their tinnitus (which then was fully improved with targeted DMSO treatment).
Airplane Ear (Aerositis)
Some individuals have immense difficulty tolerating altitude changes (to the point their eardrums can rupture), which in some cases follows an infection that inflames the Eustachian tubes, making them unable to open and accommodate the pressure changes created by increased elevation (which can be extremely painful—I know people who stopped flying because of it).
In 1967, a former president of the Aerospace Medical Association reported that DMSO could treat aerositis and aerosinusitisby spraying into their noses.
DMSO and Head Infections
One ENT doctor observed that DMSO would often significantly calm inflammation from an infection in the head (including severe ones that were difficult to treat with antibiotics). However, the improvement often only lasted for 2-4 hours. However, when he mixed DMSO with an antibiotic, it frequently eliminated the infection in a dramatic fashion (e.g., the eardrum of an otitis media patient would begin shrinking in 10-15 minutes)—especially if the infection was treated early. Unfortunately, because of how rapidly the symptoms often improved, it often caused patients not to follow up when they needed to for the subsequent treatment.
Note: mixing an antibiotic with DMSO increases its potency, in part because it more easily travels into the body (e.g., in this study, the antibiotic was dissolved in DMSO, directly applied to the eardrum, and then was able to enter the ear), partly because DMSO has its own antibacterial properties, and partly because DMSO decreases antibiotic resistance in bacteria (which will be discussed later in this series).
Additionally, he also found:
•Because of the marked drying up activity of DMSO, a subsequent treatment with a high-fat cortisone ointment was sometimes necessary to use afterward when treating otitis media.
•For irritating nasal infections or inflamed hair follicles, that the feeling of tension and pain significantly diminished within half an hour of DMSO and typically, 2-4 applications were required.
•That infections of the throat (e.g., tonsillitis) required internal applications of DMSO onto the inflamed area (rather than from the outside) and that cases with edema frequently had dramatic results (e.g., edema of the uvula often disappeared within hours).
•Significantly facial injuries (all of which had accompanying hematomas and included 2 traumatic hematotympanums and 2 hematomas of the nasal septum) had excellent responses (e.g., the hematomas and swelling distinctly improved on the first day, and the healing process as a whole was reduced to about half to a third of the average time and the 2 nasal septum hematomas did not require an incision or lead to colliquation).
•Three patients who had lost their smell were treated with DMSO. One had a striking response and immediately regained it; the other two had temporary improvements after each administration of DMSO.
•Many patients with stomatitis apthosa (canker sores) have a good response to DMSO. Unlike the other applications, 60% DMSO (applied as a spray) was used.
He then compiled all of his cases:
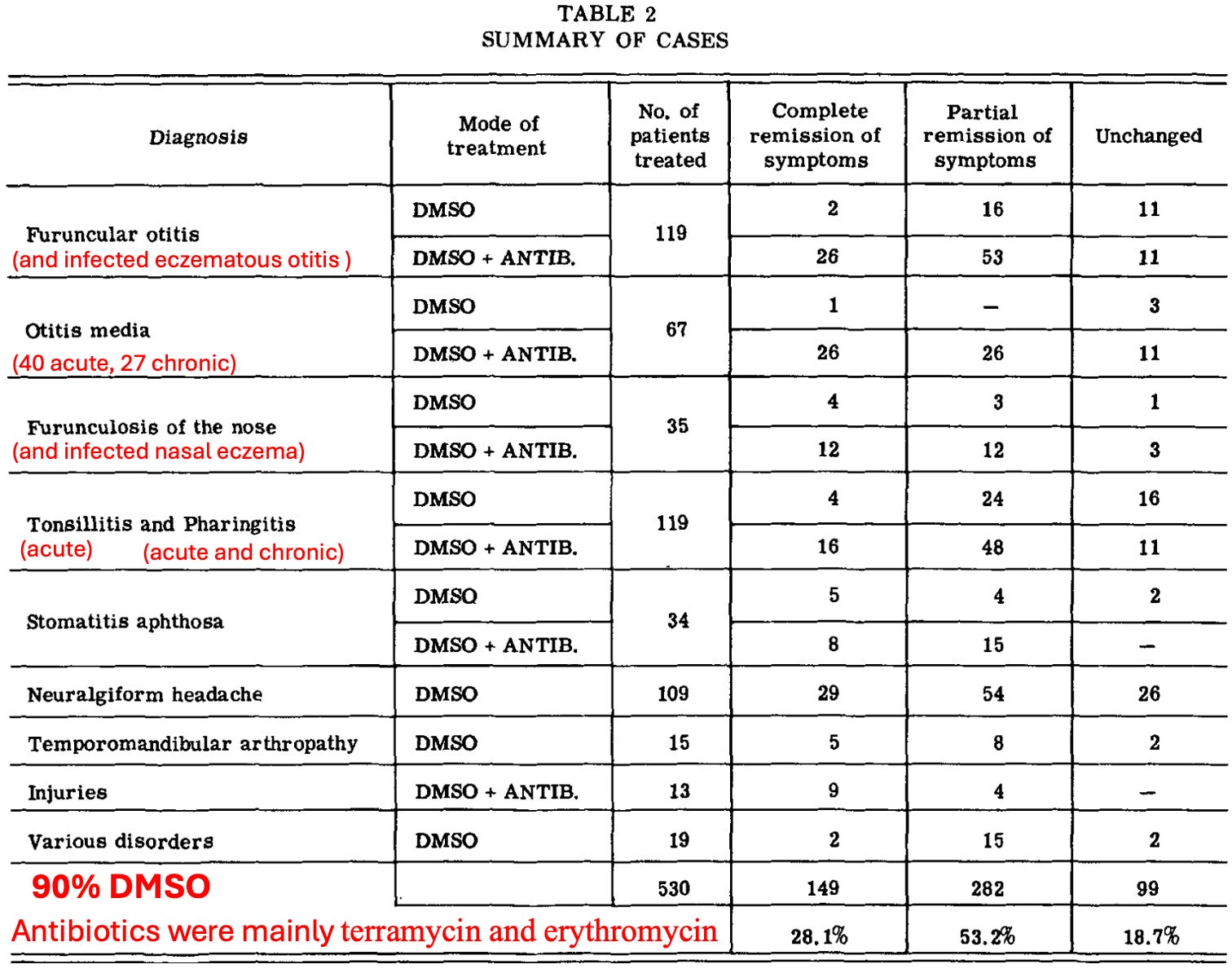
Note: most of the poor responses in otitis media were in chronic cases. Of the 27, 4 had a “very good” response, 13 had a “distinct improvement” (but generally relapsed in a short time), 10 had “no change” and 1 became worse.
A similar Russian study gave DMSO with success to 69 children (37 girls and 32 boys) with otitis media and 17 with maxillary sinusitis. In the otitis media cases, 30-50% DMSO (sometimes mixed with an antibiotic) was poured into a cleaned ear (under slight pressure) and typically passed through the eustachian tube into the nasopharynx (throat). In suppurative otitis media, there was a rapid cessation of pussy discharge from the ears, a return of hearing, and a normalization of the blood. In purulent inflammation of the maxillary sinus, 30-50% DMSO was given by injection, and cures were achieved in 4-8 days in the majority of cases, with the treatments usually lasting long term.
Finally, one approach for treating middle ear infections is to puncture the ear drum with a needle and drain it. Since this is quite painful, this doctor decided to try swabbing a drop of DMSO mixed with tetracaine against the ear drum, as DMSO both potentiates local anesthetics and can allow them to pass through the eardrum without needing to puncture it (which would be immensely painful for any child). In turn, at the 1966 annual meeting of the American Academy of Ophthalmology and Otolaryngology, shared that had done this one 107 patients with serous otitis and 50 with purulent otitis media, of whom 80% had no pain, and 20% only had slight pain.
Puncturing a child’s ear almost always requires putting them under anesthesia, which makes the procedure more costly and has its own set of complications, so having a way to perform the procedure while avoiding anesthesia would be of great benefit.
Sinusitis
DMSO has often been observed opening blocked nostrils within a few minutes due to its antibacterial and anti-inflammatory effects, which allow it to reduce swelling in the sinuses and promote the healing of inflamed tissue. In addition to the previously mentioned studies where it showed benefit for sinusitis:
•A large DMSO study included 7 female patients (aged 43-66) who had had sinusitis for 1 week to 9 months and received DMSO. Of them, 2 had a good response to it, and 5 had an excellent response. Likewise,
•In 1965, Merck sent out guidance to their investigators on what they had learned from treating approximately 4,000 patients for up to 18 months. In it, they mentioned one of the conditions DMSO had shown efficacy for was sinusitis and that “A dilute solution to the nasal mucosa has resulted in the discharge of a great deal of infected material from the sinuses and relief of pain.”
•A 1992 Russian study found administering 10% DMSO to the sinuses followed by local oxygenation, within 2 years, 49 out of 52 children had a complete recovery (including all cases of maxillary sinusitis) whereas many controls receiving standard treatments did not.
DMSO in Dentistry
Many people find DMSO to be an excellent mouthwash or toothpaste, and when DMSO is used on the gums, they are much less likely to bleed. Additionally, DMSO can often relieve pain from a toothache until a dentist is seen, and pain in the oral cavity can be alleviated by swilling the mouth with a DMSO drink solution.
Likewise, some dentists in practice find DMSO (or DMSO combined with an antibiotic) very helpful for pain, infections, and swelling in the mouth, as well as for saving teeth that are starting to loosen from periodontitis. In turn, three authors have reported on dentists using DMSO in their practices:
•Stanley Jacob reported on a Portland dentist who specialized in restorative work and found that applying DMSO after a dental procedure consistently eliminates the pain (from intrapulpal inflammation) that some patients often experience after dental (even in those who have undergone a full day of restorative work.
•Another author reported other dentists use DMSO in a similar manner (e.g., for pain, infections, and swelling issues or after teeth extractions—where it is either applied to the gum or outside on the cheek or on the jaw next to the extraction site) and frequently combine it with other medications (e.g., antibiotics). Additionally, he cited a dentist in New York who applies DMSO to areas that will be x-rayed to prevent the damage the x-ray could cause (as DMSO has been shown to do this).
•Another author reported that pioneering dentists are dropping DMSO into empty tooth sockets after extractions, especially those for wisdom teeth, as it stops post-extraction swelling.
A variety of papers have also been published on DMSO’s value in dentistry:
• A 1969 Polish study followed, this evaluated 32 male and female patients (ages 18-45) with periodontal disease. In 13 of the patients, the disease only involved bleeding and swollen gums. In the other 19, the oozing and painful pockets of infection extended deep into the gum, sometimes involving the dental nerve, bone, and loose teeth. After cleaning and repairing the teeth as much as possible, the patients were treated with DMSO every other day for 7-10 treatments.
Compared to controls, this resulted in “remarkable improvements.” Specifically, there was a total elimination of pain, decreased bleeding, and gum adherence to teeth in those patients with superficial disease. At the same time, those with deep infections reported less inflammation and disappearance of painful symptoms, but none of them had very loose teeth firm up.
Note: a preliminary version of this study can be found here.
Following this, many others were also written outside of America:
•The earliest one I know of was conducted in 1968 and showed DMSO improved the pulp of monkey’s dental teeth. Three weeks later, that author then published a study that found DMSO improved 75% of pulpitis cases, while DMSO plus oxyphenylbutazone (a drug for gout) or chloramphenicol improved 85% of cases, while placebo only improved 50% of cases, and five months later published another paper on using a DMSO combination for pulpitis.
Note: this author conducted controlled studies on using DMSO for pulpitis for 10 years (e.g., he also published this, this, this, and this study).
•A 1981 Russian study found DMSO mixed with azathioprine treats periodontosis.
•A 1981 Russian study mixed DMSO with oxacillin and ectericide was able to significantly accelerate the healing of a dry socket (an unhealed wound following a dental extraction).
•A 1983 Russian study of 222 people (176 had acute serous limited pulpitis and 46 — chronic fibrous pulpitis) found 70% DMSO placed into cavities was effective in 98.4% of acute cases and 89.3% of chronic cases, and that in most cases, this benefit persisted. Additionally, of 9 of the 16 cases with chronic fibrotic pulpitis benefitted from DMSO.
•A 1983 Bulgarian study found 15% DMSO mixed with a herbal extract treated periodontal disease.
•A 1986 Russian study found a DMSO containing paste treated deep caries.
•A 1987 Russian study showed how DMSO mixed with indomethacin can treat generalized periodontitis
•Another 1987 Russian study found DMSO helps deep caries and acute focal pulpitis
•A 1988 Russian study found of adolescent patients found DMSO plus procaine treated chronic parenchymatous parotitis (inflammation of the salivary glands).
•A 1993 Russian study found DMSO plus short-acting insulin and 5% calcium pantothenate (B5) safely treated 42 patients ages 23 to 62 with chronic parenchymatous parotitis.
•A 1998 Russian study found 50% DMSO with 2.5% orthophene stopped type I and type II autoimmune inflammation in the periodontium.
Applying DMSO to the Head
While applying DMSO to the body will often create positive effects on conditions in the head since DMSO spreads through the body, it is often necessary to apply DMSO directly to the area where the issue occurs so a higher concentration of DMSO can reach the area. In turn, many of the principles for using DMSO I’ve highlighted throughout this series hold true for the local applications to the head, but there are also a variety of unique considerations.
For example, people often will have things on their faces they do not want to transmit in the body such as:
•Contacts
•Metallic residues from the nose pads of glasses.
•Make-up
•Dyes or chemical cleaning products in the hair.
Because of this, things like contacts must be taken off before using DMSO and you should ensure the area it is applied to has been cleaned beforehand if any chemical residue may have been left there.
Note: it’s also important that each thing you use to dilute DMSO is also chemical free (so don’t pour it with plastic spoons, don’t use plastic droppers, and be sure to use purified water to dilute it).
Likewise, the face is one of the most sensitive parts of the body to DMSO, so typically topical applications need to be started at a low concentration and gradually increased rather than a high concentration of DMSO immediately used on the face (especially stronger gels), as otherwise the skin may get irritated and make the user not want to use DMSO.
In the final part of this article, I will discuss the protocols that have been developed for each of the conditions listed throughout this article (e.g., macular degeneration, tinnitus, sinusitis, aerotitis, and dental hygiene), where to source the best DMSO for doing so alongside some other related approaches I’ve come across over the years that I’ve found really help these conditions.
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.