

DMSO Transforms The Treatment of Infectious Diseases
How DMSO can treat many challenging infections

Story at a Glance:
•Dimethyl Sulfoxide (DMSO) is a remarkably safe naturally occurring substance that has a variety of remarkable properties that make it well suited to treating a variety of challenging medical conditions (e.g., pain, injuries, wounds, strokes, spine injuries, autoimmune conditions, cancer, and internal organ diseases).
•DMSO has broad antimicrobial properties, protects the body from microbial toxins (e.g., from C. diff), eliminates antibiotic resistance, and serves as a vehicle that can bring antimicrobials deep into the body and treat otherwise inaccessible infections.
•DMSO significantly enhances the treatment of many common bacterial infections (e.g., of the head, mouth, and skin) and many severe bacterial infections that require hospitalization (e.g., tuberculosis, sepsis, peritonitis, severe lung infections, osteomyelitis). In many cases, this has allowed an individual requiring an amputation of a chronically infected area to instead fully recover.
•DMSO has significant antiviral properties, which have most extensively been studied for herpes and shingles (both of which it excels in treating), but also in a variety of other conditions (e.g., feline panleukopenia, one of the most deadly conditions cats face.
•DMSO has significant value in treating challenging fungal and parasitic infections. Additionally, evidence suggests its utility in treating cancer and autoimmune disorders arise from DMSO’s unique antimicrobial properties.
•In this article, we will review the body of evidence showing DMSO’s remarkable contributions to the treatment of infectious diseases and provide guidance on how DMSO can be used to treat many of the conditions listed in this article.
Introduction
DMSO is a remarkably safe and naturally occurring substance (provided you use it correctly) that rapidly improves a variety of conditions medicine struggles with — particularly chronic pain. For reference, those conditions included:
Strokes, paralysis, a wide range of neurological disorders (e.g., Down Syndrome and dementia), and many circulatory disorders (e.g., Raynaud’s, varicose veins, hemorrhoids), which I discussed here.
A wide range of tissue injuries such as sprains, concussions, burns, surgical incisions, and spinal cord injuries (discussed here).
Chronic pain (e.g., from a bad disc, bursitis, arthritis, or complex regional pain syndrome), which I discussed here.
A wide range of autoimmune, protein, and contractile disorders such as scleroderma, amyloidosis, and interstitial cystitis (discussed here).
A variety of head conditions, such as tinnitus, vision loss, dental problems, and sinusitis (discussed here).
A wide range of internal organ diseases such as pancreatitis, infertility, liver cirrhosis, and endometriosis (discussed here).
A wide range of skin conditions such as burns, varicose veins, acne, hair loss, ulcers, skin cancer, and many autoimmune dermatologic diseases (discussed here).
In turn, since I started this series, it struck a cord and has now been seen by millions of people, and I have received over 1400 reports of remarkable responses to DMSO many readers have had (which can be read here).
This begs an obvious question — if a substance capable of doing all of that exists, why does almost no one know about it? Simply put, like many other promising therapies, it fell victim to a pernicious campaign by the FDA which kept it away from America despite decades of scientific research, Congressional protest, and thousands of people pleading for the FDA to reconsider their actions. Consider for example, this 60 Minutes program about DMSO that aired on March 23, 1980:
DMSO and Infectious Diseases
DMSO has a variety of unique properties that make it incredibly well suited to addressing microbial infections (e.g., bacteria, fungi, viruses, and parasites).
These include:
•While non-toxic, it has an antiseptic effect that is harmful to microorganisms, especially the smallest ones (mycobacteria, cell wall deficient bacteria, and viruses). This property appears to be the most beneficial for herpes, shingles, and other complex conditions, which I believe have a microbiological component (e.g., cancer and autoimmunity).
•It can remove the antibiotic resistance of bacteria. This is particularly helpful in widespread problematic infections that have gradually developed a resistance to many existing antibiotics (e.g., tuberculosis) and challenging infections that are not responding to antibiotics (e.g., ones that would otherwise require an amputation).
•It can further increase the sensitivity of already susceptible microorganisms to antimicrobial agents.
•It can deliver antimicrobial agents to areas that are typically difficult to reach (e.g., deep in a bone) and also directly to regions that would otherwise require a systemic application of the medication.
•It can increase circulation to many parts of the body, something which is often critical for resolving illnesses (as a healthy blood supply allows the immune system to enter and heal diseased areas). Likewise, pretreatment with DMSO has been shown to increase the immune system’s ability to resist a subsequent infection.
•Much in the same way DMSO protects cells from a wide variety of lethal stressors, it can also protect them from the harmful effects of bacterial toxins (e.g., with the most pertinent applications studied being for sepsis and clostridium difficile). Likewise, it can also mitigate the toxicity of antimicrobial agents taken for a prolonged period.
Many of these properties are exceedingly unusual and can completely transform the practice of medicine. I will now provide much of the data substantiating the above claims.
Note: unless otherwise specified, all pharmaceuticals listed here are antibiotics.
Shingles and Herpes
Since many people struggle with Herpes (HSV-1 or HSV-2) and Shingles (Herpes Zoster), especially the pain which follows shingles (known as post-herpetic neuralgia or PHN), DMSO has been extensively studied for these uses. For instance, as discussed previously, there was a brief boom in DMSO research (during the 1960s and 1970s many pharmaceutical companies realized DMSO was a remarkable drug for them to sell) that was then abruptly shut down by the FDA banning virtually all DMSO research so they would not have to deal with the influx of new drug applications (as DMSO had so many remarkable uses).
Immediately prior to this ban, Merck for example, which had made significant investments in testing DMSO, sent out a guidance to all of their investigators detailing what they had learned after roughly a year of testing and over 4,000 patients which included:
Herpes Zoster has responded most favorably.
DMSO in turn, has been repeatedly found to treat herpes throughout the body (e.g., on the face and the genitals), shingles, and post-herpetic neuralgia.
Note: DMSO has also been found to be quite helpful for aphthae (canker sores).
DMSO alone works for these ailments, but is even more effective when combined with an antiviral, particularly when combined with 5-iodo-2'- deoxyuridine (IDU), an antiviral that has poor penetration into tissues
For example, at a 1980 Congressional Hearing, one researcher, Dr. Scherbel of the Cleveland Clinic (a highly respected dermatologist), was asked if DMSO could be used for shingles. He stated that they’d found acute shingles responds to DMSO alone in a high percentage of patients, that acute vesicular lesions dry up rapidly, and that with the application of DMSO, they never saw post-herpetic neuralgia follow shingles (which is a major complication of the disease).
Note: Stanley Jacob also mentioned that while the FDA was stonewalling DMSO, DMSO plus IDU was an approved topical prescription in England and Ireland. Sadly, it is still not available in North America.
Herpes Simplex
A 1965 study used 1% IDU in 90% DMSO (and 10% distilled water) in 7 patients with severe cutaneous Herpes simplex infection and noted significant improvement in all cases, with the only side effect being slight skin irritation from the solution.
After preliminary research suggested 5% and 10% idoxuridine (IDU), an antiviral when mixed with 100% DMSO showed promise in treating primary herpes in guinea pigs, a 1966 RCT (randomized controlled trial) of 21 patients with recurrent herpes was conducted. It found DMSO halved the durations of herpes, and when given with 5% idoxuridine, cut them into a third (whereas idoxuridine alone did not do anything).
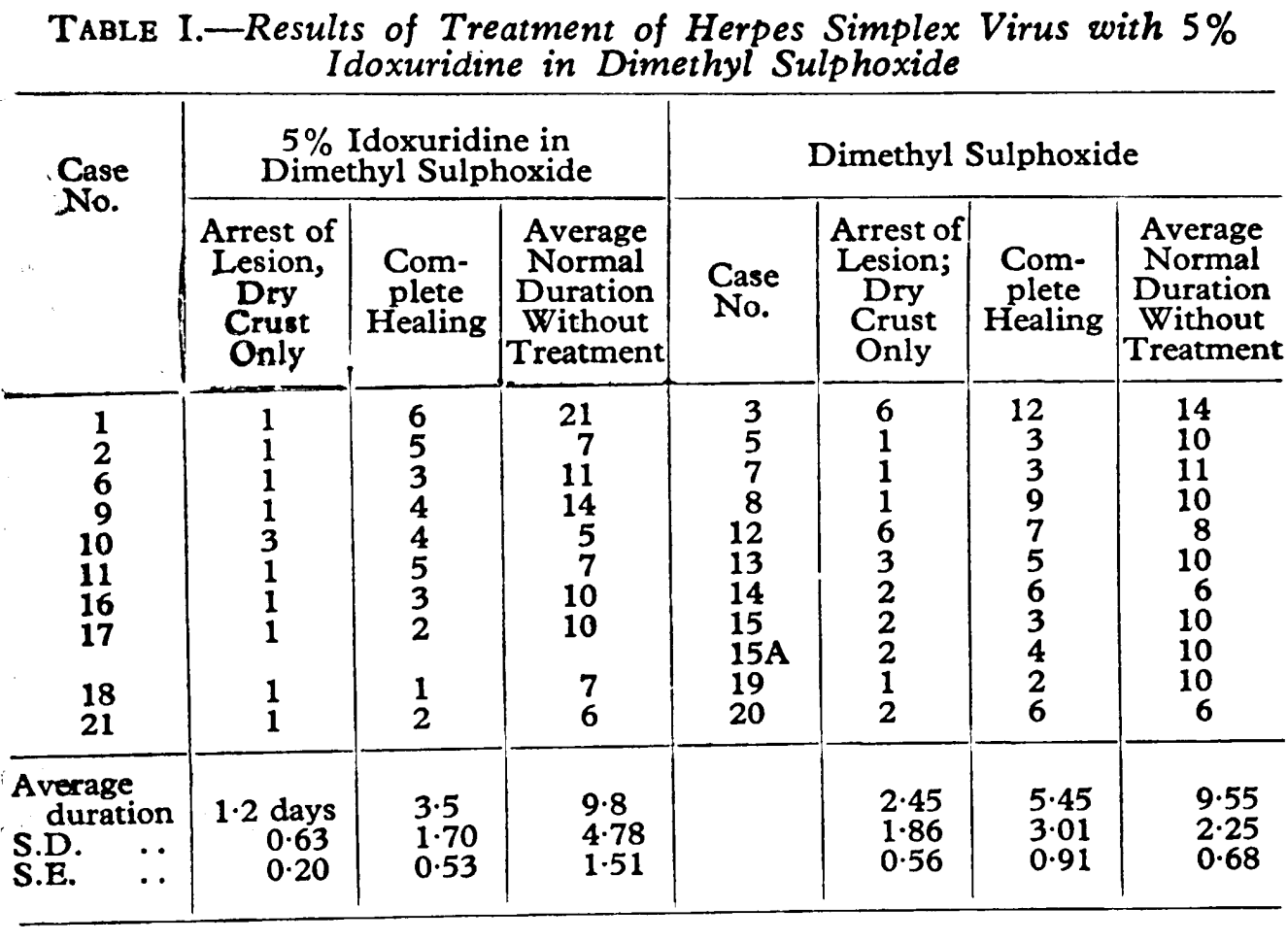
Additionally, there were no recurrences within 6 months in the DMSO IDU group (whereas 1.7 on average were expected) and only 4 recurrences happened in the 11 person DMSO only group.
•A 1967 study found DMSO plus 5-IDU was more effective for treating early severe herpes simplex lesions than DMSO alone).
In 1972, a physician reported success using 100% DMSO and 5% IDU to treat severe herpes simplex in 5 patients.
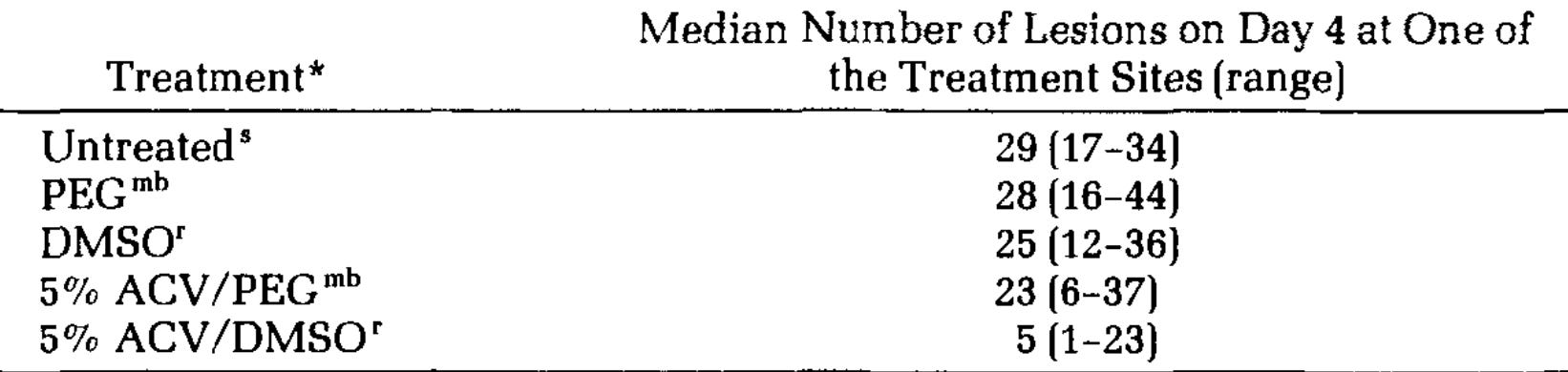
A 1983 study found that DMSO effectively brought acyclovir (ACV) into the skin, caused a moderate reduction in herpes lesions, and dramatically reduced them when combined with acyclovir.
Note: DMSO also helps herpes fever blisters, and DMSO with IDU has been reported to be effective in treating HSV whitlow (herpes on the fingers).
A 1990 RCT gave 80% DMSO mixed with 15% IDU to 301 immunocompetent female patients experiencing a recurrence of genital herpes, which reduced the mean duration of pain by 1.3 days and the healing time to loss of crust by 1.7 days. When only classic herpes lesions (vesicle, ulcer, or crust formation) were evaluated, a greater effect was seen (the duration of pain was reduced by 2.6 days and the healing time to normal skin by 2.3 days).
A 2002 cell study found 0.65% DMSO reduced herpes viral replication by 50% (while 1% mostly stopped it) and did so in a manner suggesting it inhibits multiple viral replication points, suggesting that this inhibitory effect was synergistic and that it could affect both early and late stages of an infection. Specifically, DMSO reduces the virus’s ability to infect cells, markedly inhibits viral DNA replication, and blocks the transcription of many HSV-1 genes.
Note: this open access study provides a very detailed analysis of how DMSO inhibited each aspect of herpes viral replication.
Note: while DMSO has not been studied for human viral encephalitis (e.g. from herpes), it has been used as a therapy for equine herpesvirus-1.
Shingles and Post Herpetic Neuralgia (PHN)
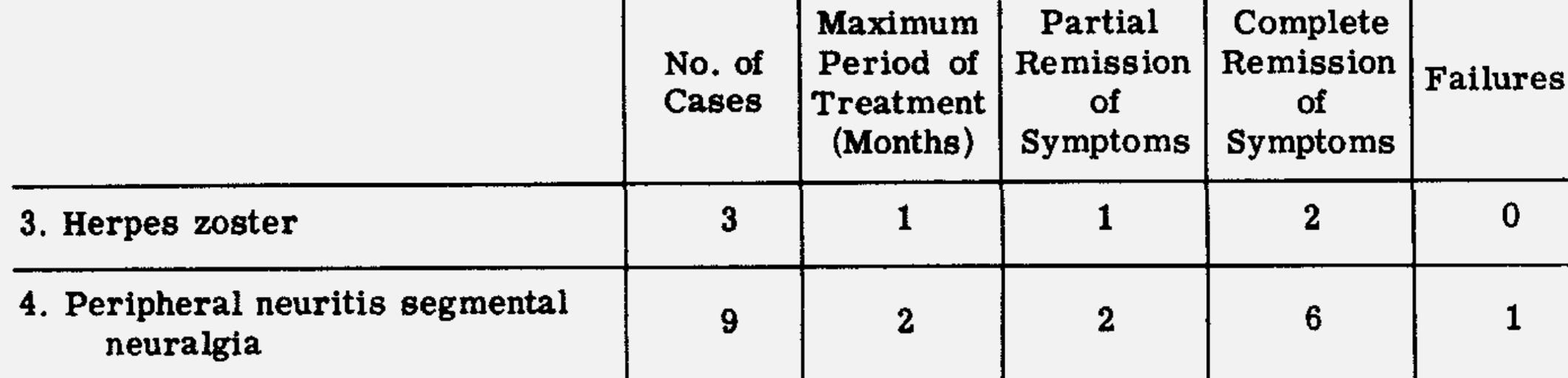
In 1967, a German investigator reported DMSO yielded generally good results in 10 of 11 shingles and PHN cases.
A larger 1967 study of 4180 patients included a few shingles patients who had a positive response to DMSO.
Two 1970 RCTs showed that both 5% and 40% IDU in DMSO were effective over 4 days of repeated applications in reducing shingles, but that 40% IDU was more effective (as was continuous rather than intermittent treatment). With both 5% and 40% IDU, there was a large reduction in the duration of pain (likely due to DMSO’s ability to eliminate pain), whereas, in the 40% IDU group, there was also a significant reduction (30%) in the time the lesions took to begin healing was seen, along with how long the vesicles took to dry (28.6%), and how long it took to complete (35%).
The patients were delighted, for the pain disappeared within a median of two days.
Note: the authors previously tried using IDU without DMSO for herpes simplex and saw no benefit from that treatment.
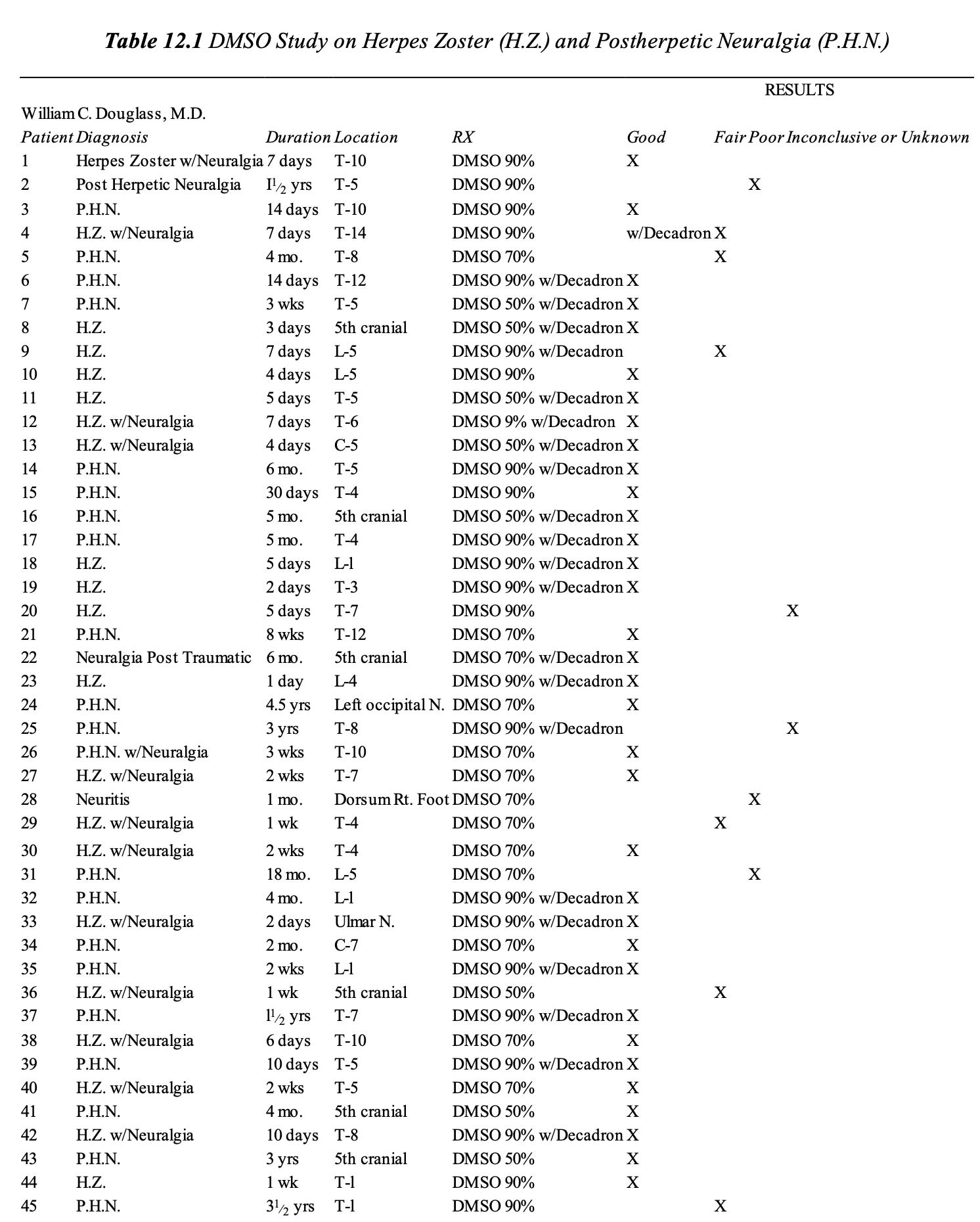
In 1971, Dr. William Campbell Douglass (a pioneer in the integrative medical field) conducted an unpublished study (presented in this book) that showed shingles was highly responsive to DMSO (73.3% had a good response to treatment and 13.3% had a fair response to treatment), and that the sooner DMSO is used, the better the response will be.
Note: there are other methods to use DMSO to treat herpes which can give an even faster response.
A 1974 RCT of 118 patients with shingles found 100% DMSO and 5% IDU applied every 4 hours for 4 days. It significantly shortened the vesicular phase, healing time, and duration of pain, and it significantly improved post-herpetic neuralgia. Additionally, no greater benefit was seen with 25% IDU, and the only side effects (seen in 2 patients) were transient tender redness in three patients and "urticarial" edema with dermographia.
A 1979 study found that 40% DMSO plus IDU created a small but significant improvement in the healing of shingles.
A 1981 trial gave 46 shingles patients either DMSO or DMSO mixed with 5% IDU. Compared to DMSO alone, DMSO plus IDU significantly reduced the time it took pain to improve, and significantly fewer new vesicles developed.
A 1992 RCT of 171 patients with non-severe shingles (which had been present for less than 4 days) found that compared to acyclovir, 40% DMSO topical mixed with IDU was a superior treatment for how quickly all vesicles dried, how long moderate-intense pain, hyperaesthesia and itching lasted, and how long reducing medications were required, how frequently new vesicles appeared, and in preventing post-herpetic neuralagia.
Additionally, Stanley Jacob has also reported being able to treat chronic post-herpetic neuralgia (which had been present for over 2 years).
Note: one of the rarest and most severe complications of shingles (where the face becomes paralyzed) is Ramsay Hunt Syndrome, a condition which became more common after the COVID vaccines (e.g., it affected Justin Bieber). Recently, one reader successfully treated it with DMSO.
Combined Studies
A 1969 study gave DMSO to 37 patients with herpes simplex, shingles, chickenpox, and smallpox vaccine rashes, all of whom healed in approximately one-third of the normal time. Newer cases healed rapidly, while older herpes simplex cases took longer to heal and tended to recur (although if the recurrence was treated promptly, it healed quickly, and there was no future recurrence). Post-herpetic neuralgia sometimes occurred in shingles patients, but it was shorter than normal (of the 11, one had it for 3 weeks, one for 7 weeks, and one for 6 months).
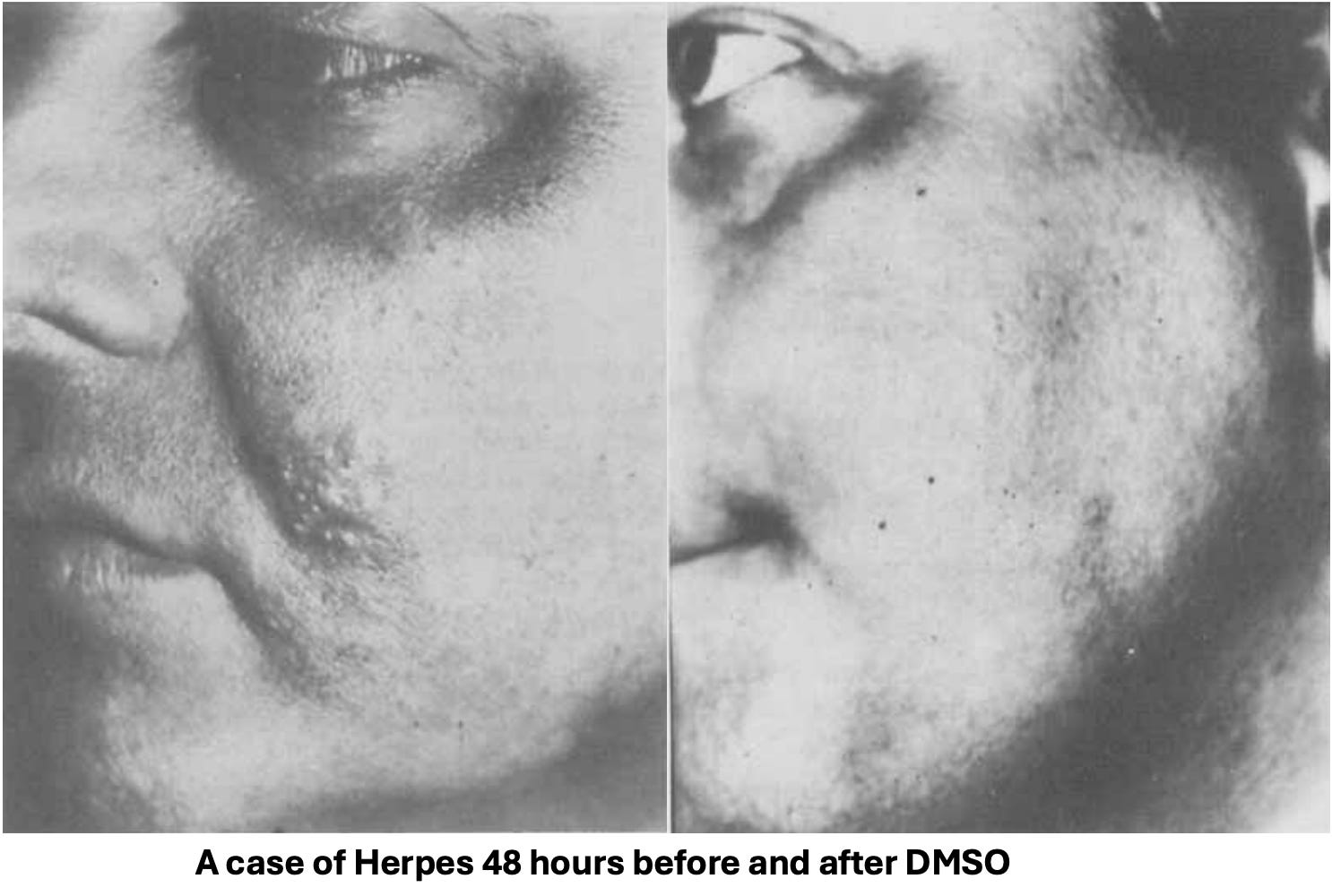
A 1975 study reported on 152 patients with a wide range of dermatologic conditions who received a topical DMSO spray (with no side effects except temporary intense pain in two of the recipients).
•Shingles (7)—all 7 had dramatic results within 48 hours (often completely disappearing).
•Herpes simplex (4 on the penis, 4 on the lips, 2 on the cheeks)—all 10 had dramatic results within 48 hours (often completely disappearing).
DMSO IDU Studies
A 1977 review determined that adding IDU to DMSO does not create any additional toxicity or side effects compared to DMSO alone.
A 1986 study established that DMSO dramatically increases the penetration of acyclovir and IDU into the skin:
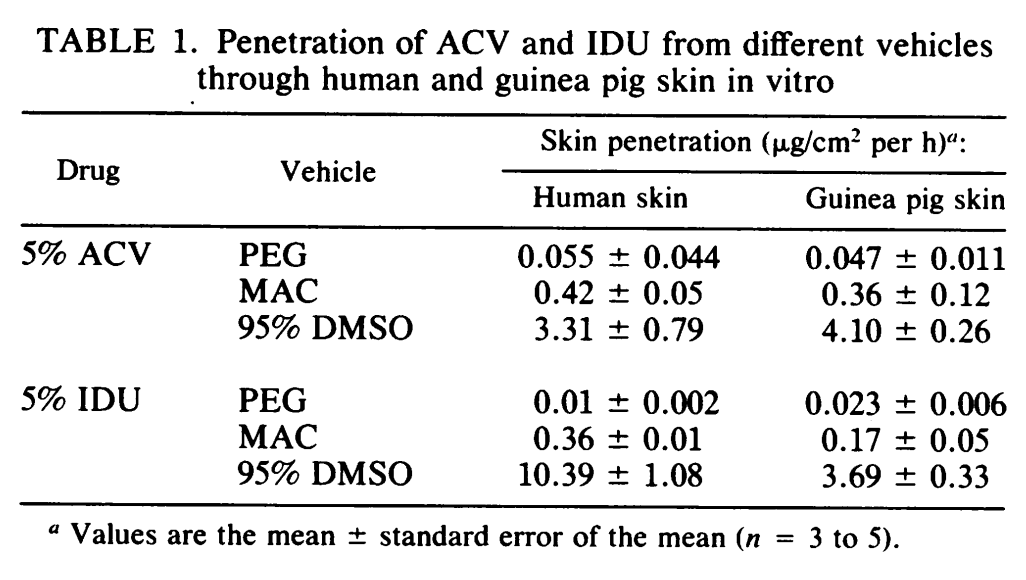
In 1988, investigators determined that the maximum benefit of IDU mixed with DMSO was likely to be at 20% IDU, higher concentrations of IDU did not result in more IDU reaching the area. However, in most studies, 5% or 40% IDU was tested.
DMSO and Bacterial Infections
DMSO has six properties that make it useful in treating bacterial infections.
First, data suggests DMSO increases bacterial cell membrane permeability and concurrently creates changes in the cell indicative of damage to its membrane. In addition to directly eliminating bacteria, it also reduces their ability to prevent antibiotics from entering them. In turn, existing data shows DMSO has a much greater ability to increase the potency of antibiotics that target structures inside bacteria rather than ones that target their cell wall (e.g., penicillin).
Note: this property is particularly important for tuberculosis as it has a robust external barrier that impairs antibiotic entry.
Second, by increasing membrane permeability, it can also make bacteria more susceptible to taking up the nucleic acids of lethal bacteriophages (viruses that kill bacteria and have been extensively researched outside of America due to their efficacy in treating a wide range of bacterial infections).
Third, DMSO can often simply dissolve bacteria and cause their contents to leak out.
Fourth, DMSO can interfere with the normal functioning of bacteria. A 1977 study, for instance, found that it interferes with the production of membrane proteins that E. coli (and other bacteria) need for metabolism.
Fifth, as discussed throughout a previous article, DMSO greatly improves circulation (which, when impaired often leads to chronic infections).
Sixth, in the same way DMSO can protect cells from various lethal stressors (discussed here), DMSO effectively mitigates the harmful effects of many bacterial toxins.
Additionally, while many concerns existed that DMSO’s anti-inflammatory properties might cause immune suppression, this has not been the case. A 1984 mouse study for example, found that giving DMSO prior to injecting E. coli or L. monocytogenes did not suppress the immune response to it, increase the lethality of either bacteria, or impair the body’s clearance of the infection, hence eliminating concerns that it could reduce a needed immune response (as DMSO is anti-inflammatory).
Conversely, DMSO in some instances, has been shown to enhance the immune response. For example:
•The oxidative burst (where highly reactive oxidative chemicals like peroxynitrite are briefly generated) is utilized by immune cells to eliminate invading microorganisms. Unlike many other antioxidants, DMSO enhances the bactericidal properties of it.
•In 1966, it was reported that giving mice oral DMSO 8 days prior to infecting them with typhus made them more resistant to the infection.
Note: the same researcher also repeatedly demonstrated that giving a typhoid vaccine while a latent typhoid infection was present would trigger immune suppression, which would cause acute typhoid to develop.
Common Microbes
DMSO has been extensively tested against common infectious bacteria (e.g., staph, strep, E. coli, pseudomonas), both by itself and in combination with antibiotics (e.g., a 1986 article discussed DMSO’s potential for being combined with antibiotic therapies) along with other antimicrobial therapies.
That research and the pertinent data are as follows:
In 1964, Stanley Jacob reported that 20% DMSO had a bacteriostatic effect (growth inhibiting activity that does not kill bacteria) against E. coli, Staph aureus, and Pseudomonas cultures, and that 1% DMSO made resistant tuberculosis more sensitive to antibiotics.
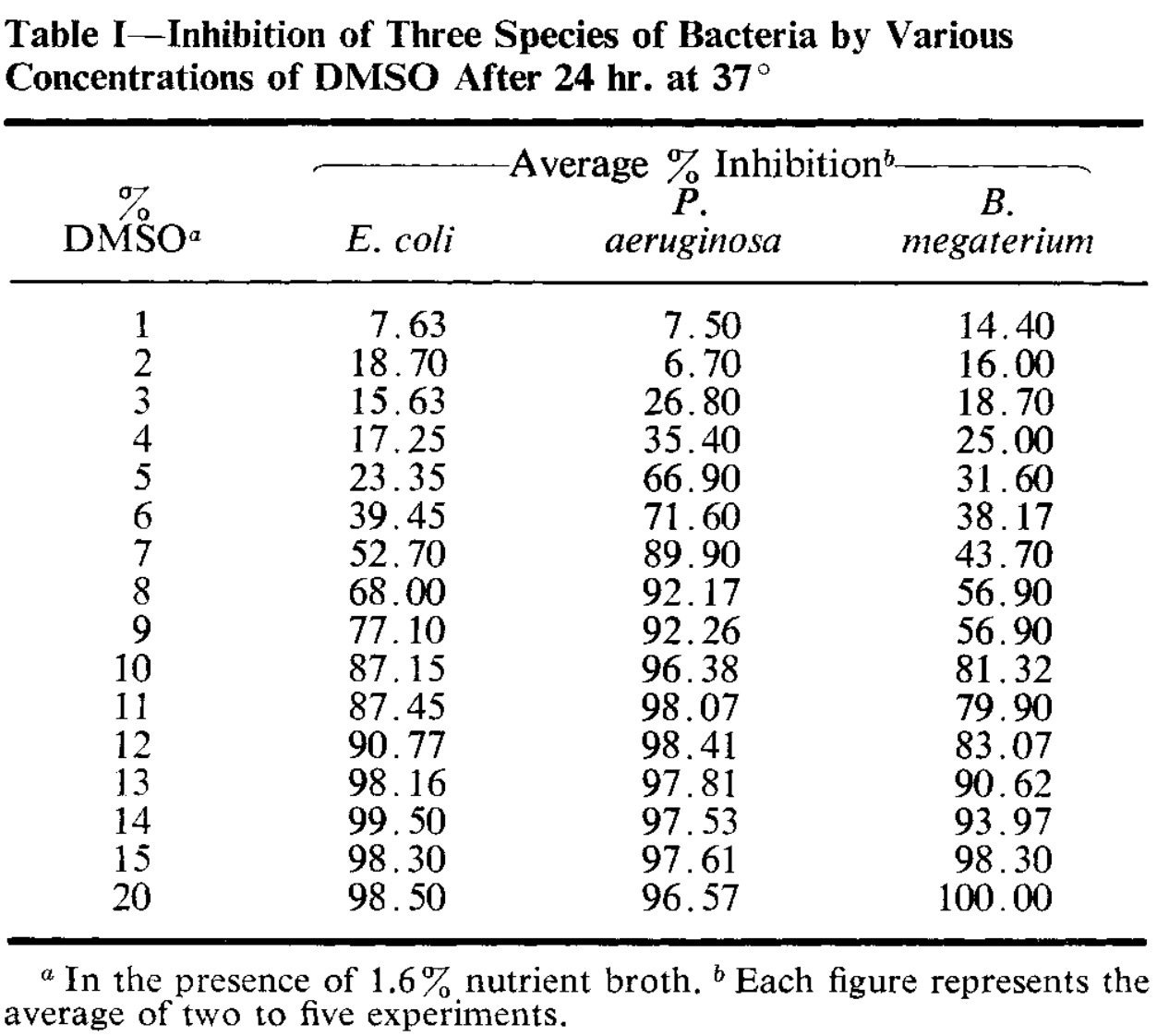
A 1965 study found DMSO’s minimal inhibitory concentration (MIC, a common way to assess how potent antibiotics are) was 50% for Staph Aureus and between 30-40% for Staph epidermidis, β-hemolytic strep, Corynebacterium acnes, other Corynebacterium species (normal skin residents), Alcaligenes faecalis, E. coli, and Proteus bacteria, and that applying 90% DMSO to the armpit three times per day for three days eliminated 90% of the bacteria. Additionally, at 20% DMSO was bacteriostatic, and an hour of exposure to 60-75% of DMSO was required to kill those bacteria—all of which led the investigators to conclude DMSO was a low-potency antibiotic.
A 1966 study found that 5% DMSO increased bacterial antibiotic sensitivity, both in antibiotic sensitive strains and in many antibiotic resistant strains. For example, all 4 strains of colistin-resistant pseudomonas became sensitive, while resistant E. coli did not become penicillin sensitive. Additionally, DMSO inhibited bacterial growth by itself.
In 1966, another investigator found DMSO’s MIC for S. Aureus was 30%.
A 1967 study tested DMSO’s inhibitory effect against various microorganisms, and found at sufficient concentrations that it caused those organisms to dissolve into a sediment.
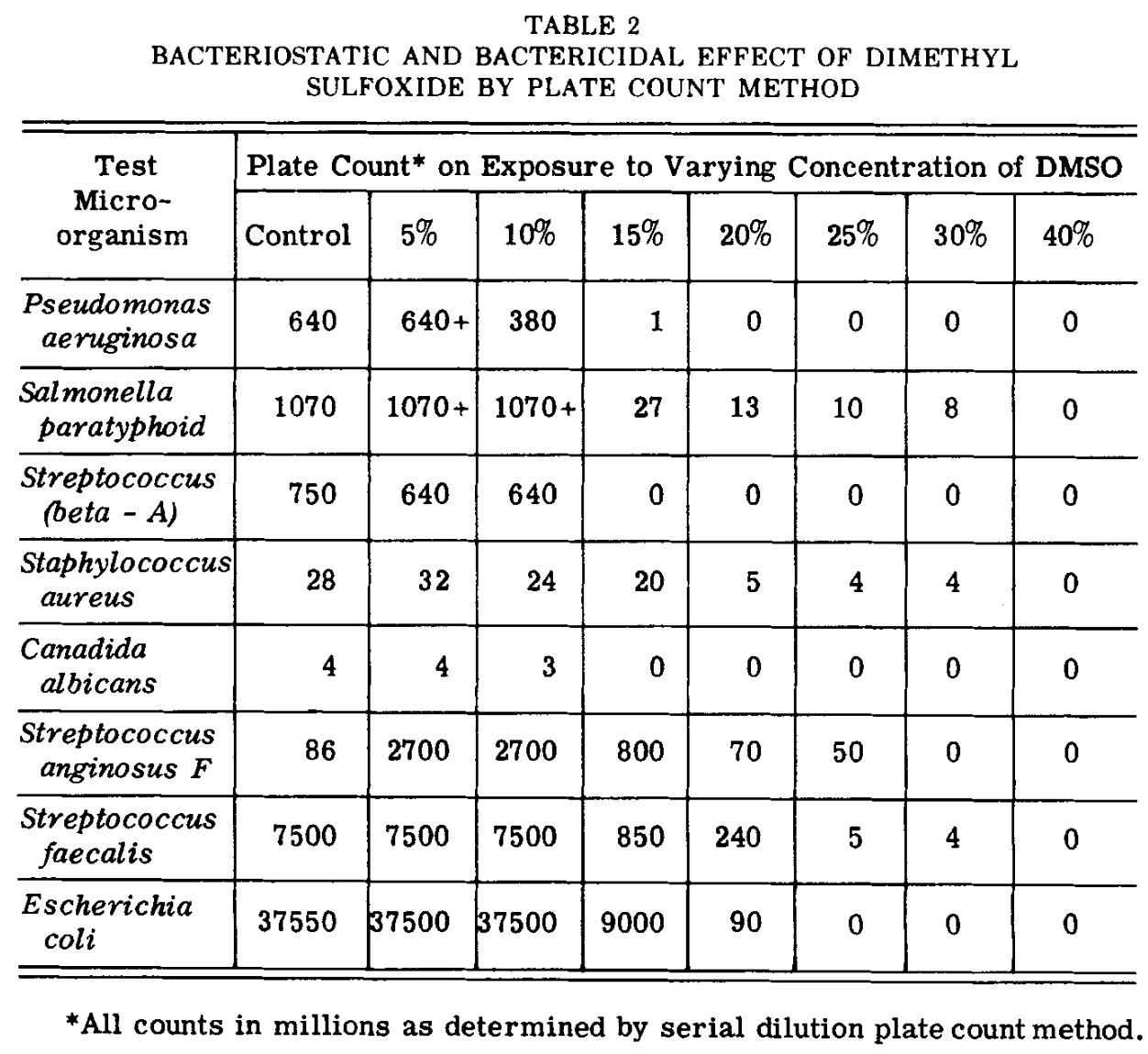
Note: a few other organisms were also tested. For each, DMSO’s bacteriostatic concentration was: Aerobacter cloacae (20-30%), Proteus vulgaris (20-30%), Salmonella schottmulleri (10-30%), Strep. pneumoniae (4-5%). Given that Strep. pneumoniae is involved in a variety of challenging conditions, its high sensitivity to DMSO (which was seen at 4% but not 1% DMSO) holds promise for those infections.
A 1967 study reported that for antifungal and antibacterial applications, the effectiveness of dimethyl sulfoxide increases sharply above 70%.
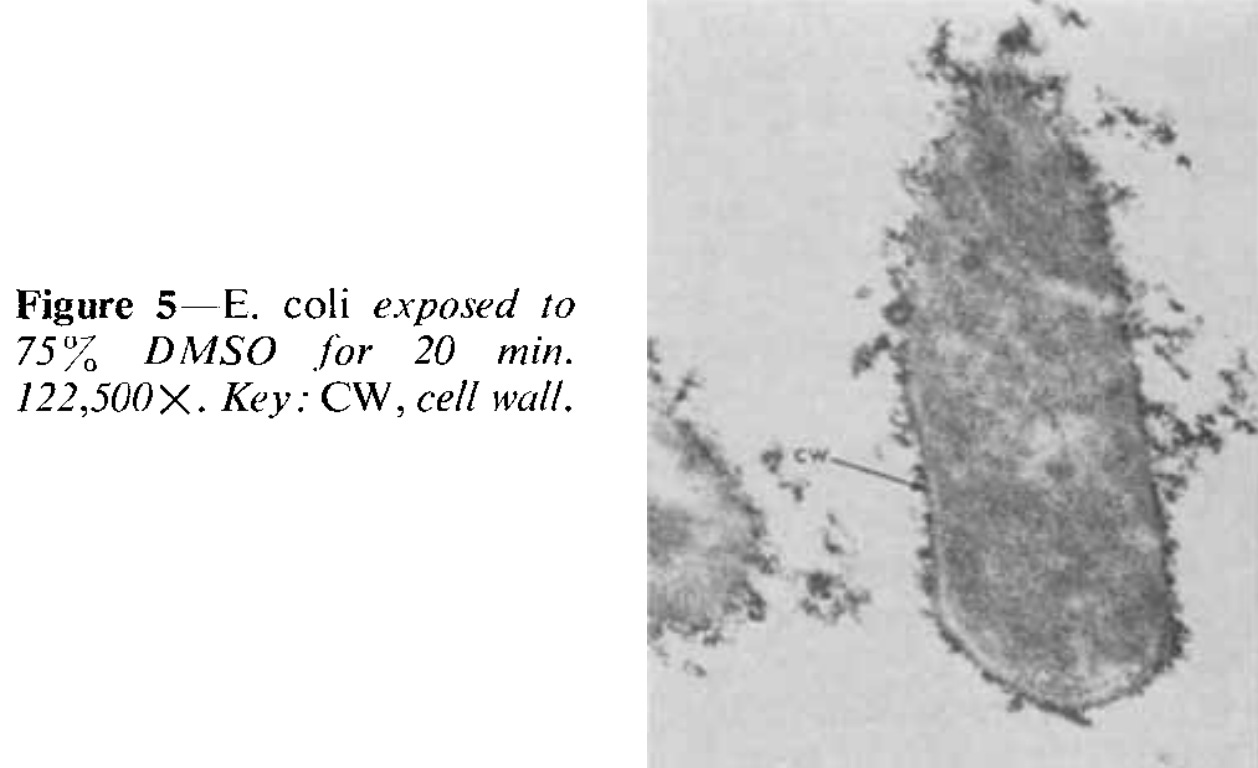
A 1969 study found that 75% DMSO was bactericidal (mainly by causing their internal contents to leak out), while 15% was sufficient to stop bacterial growth.
•A 1972 study discussed using DMSO to treat staph infections in young children and a 1973 study discussed using it to treat deep staph infections in young children
•A 1975 study from that DMSO dramatically lowered the minimal inhibitory concentration of streptomycin in resistant E. coli, causing it to go from over 5000 µg/ml to 7.5 µg/ml. The investigators concluded this effect was most likely due to DMSO increasing membrane permeability to streptomycin.
•A 1989 study found that DMSO enhanced the efficacy of iodopiron in eliminating pseudomonas bacteria (demonstrated by electron microscope observations of the damage done to those bacteria), leading the investigators to propose using it to treat burn patients.
Note: this 1986 study also used an electron microscope to evaluate the effect of DMSO on bacteria (in this case Staph aureus).
•When antimicrobial photodynamic therapy (PDT) was used in a 2005 study to treat mice with third-degree burn wounds one day after they had been infected with Staph aureus, adding DMSO to PDT eliminated 98% of the bacteria, whereas without DMSO, there was only a marginal dose-dependent reduction of the bacteria.
•A 2012 study found that when DMSO was mixed with an antiseptic alcohol (isopropanol) it made it 10-100 times as potent (and in some cases even more) at preventing microbial growth (of common microbes). It also found that DMSO’s inhibitory effect rapidly increased with DMSO concentration (with 10% DMSO being sufficient for isopropanol to inhibit all growth).
•A 2018 study tested DMSO against a variety of bacterial strains and found that DMSO exhibited varying degrees of pronounced antibacterial activity.
•A 2024 study found 0.4% DMSO inhibited S. aureus growth, 0.3% inhibited E. coli, 0.2% inhibited C. albicans growth.
DMSO and Head Infections
Since DMSO is effective in eliminating many common microbial infections, it has shown great promise in ENT (ears, nose, and throat) medicine, as many of those diseases result from infections with common bacteria and the inflammatory response to them (particularly since it is often challenging to get antibiotics to the site of the infection—something DMSO helps greatly with).
Note: a significant part of this section and the one on dental infections is from a previous DMSO article.
Much of this was demonstrated in the 1967 publication by an ENT doctor who observed that DMSO would often significantly calm inflammation from an infection in the head (including severe ones that were difficult to treat with antibiotics).
However, the improvement often only lasted for 2-4 hours. However, when he mixed DMSO with an antibiotic, it frequently eliminated the infection in a dramatic fashion (e.g., the eardrum of an otitis media patient would begin shrinking in 10-15 minutes)—especially if the infection was treated early. Unfortunately, because of how rapidly the symptoms often improved, it often caused patients not to follow up when they needed for subsequent treatments.
Additionally, he also found:
•Because of the marked drying activity of DMSO, a subsequent treatment with a high-fat cortisone ointment was sometimes necessary to use afterward when treating otitis media.
•For irritating nasal infections or inflamed hair follicles, the feeling of tension and pain significantly diminished within half an hour of DMSO and typically, only 2-4 applications were required.
•That infections of the throat (e.g., tonsillitis) required internal applications of DMSO onto the inflamed area (rather than from the outside) and that cases with edema frequently had dramatic results (e.g., edema of the uvula often disappeared within hours).
•Significantly facial injuries (all of which had accompanying hematomas and included 2 traumatic hematotympanums and 2 hematomas of the nasal septum) had excellent responses (e.g., the hematomas and swelling distinctly improved on the first day, and the healing process as a whole was reduced to about half to a third of the average time and the 2 nasal septum hematomas did not require an incision or lead to colliquation).
•Three patients who had lost their smell were treated with DMSO. One had a striking response and immediately regained it; the other two had temporary improvements after each administration of DMSO.
•Many patients with stomatitis apthosa (canker sores) respond well to DMSO. Unlike the other applications, 60% DMSO (applied as a spray) was used.
He then compiled all of his cases:
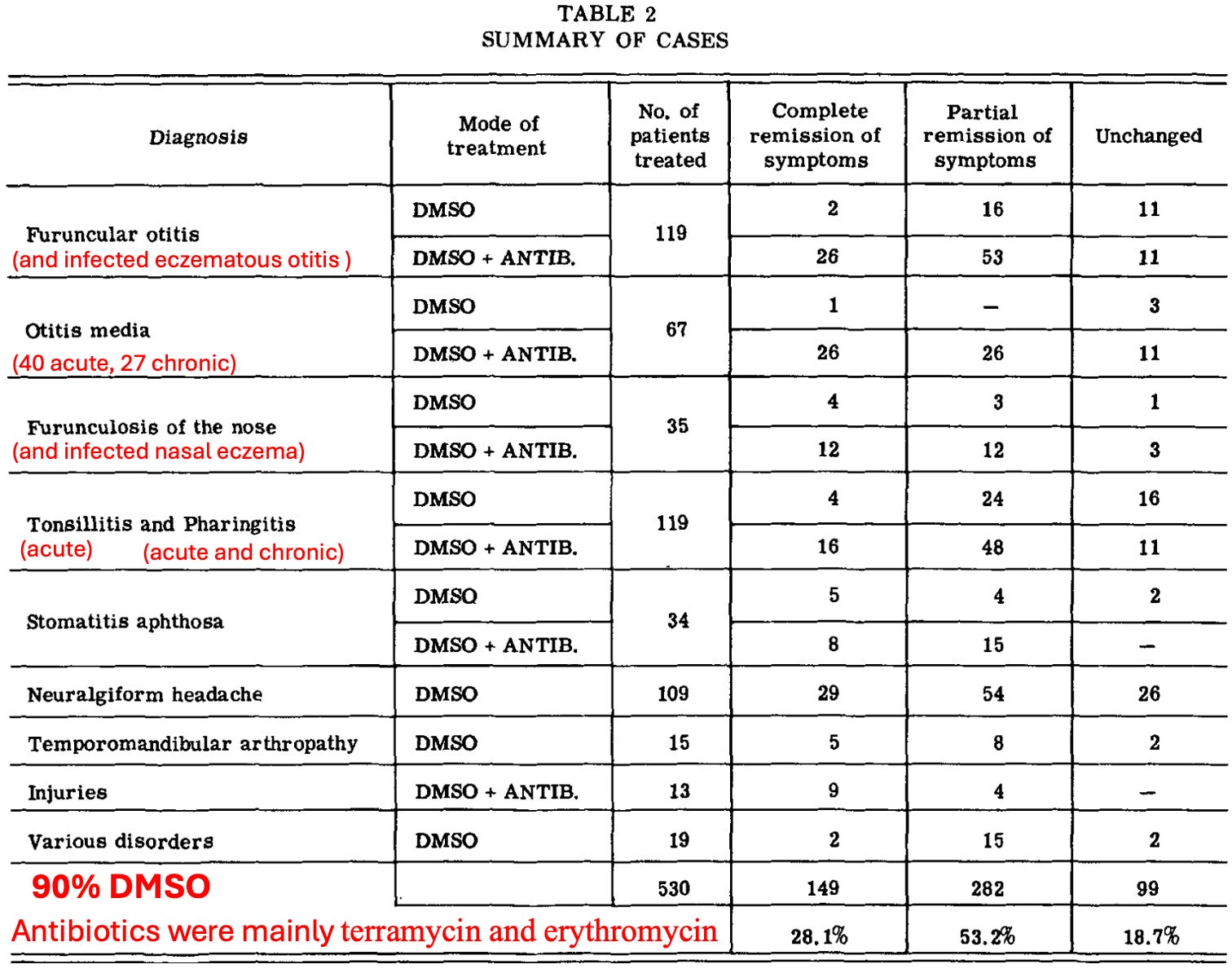
Note: most of the poor responses in otitis media were in chronic cases. Of the 27, 4 had a “very good” response, 13 had a “distinct improvement” (but generally relapsed in a short time), 10 had “no change” and 1 became worse.
•A similar 1969 Russian study gave DMSO with success to 69 children (37 girls and 32 boys) with otitis media and 17 with maxillary sinusitis. In the otitis media cases, 30-50% DMSO (sometimes mixed with an antibiotic) was poured into a cleaned ear (under slight pressure) and typically passed through the eustachian tube into the nasopharynx (throat). In suppurative otitis media, there was a rapid cessation of pussy discharge from the ears, a return of hearing, and a normalization of the blood. In purulent inflammation of the maxillary sinus, 30-50% DMSO was given by injection, and cures were achieved in 4-8 days in the majority of cases, with the treatments usually lasting long term.
•Finally, one approach for treating middle ear infections is to puncture the ear drum with a needle and drain it. Since this is quite painful, this doctor decided to try swabbing a drop of DMSO mixed with tetracaine against the ear drum, as DMSO both potentiates local anesthetics and can allow them to pass through the eardrum without needing to puncture it (which would be immensely painful for any child). In turn, at the 1966 annual meeting of the American Academy of Ophthalmology and Otolaryngology, shared that had done this one 107 patients with serous otitis and 50 with purulent otitis media, of whom 80% had no pain, and 20% only had slight pain.
Puncturing a child’s ear almost always requires putting them under anesthesia, which makes the procedure more costly and has its own set of complications, so having a way to perform the procedure while avoiding anesthesia would be of great benefit.
Eye Infections
DMSO can help a variety of eye conditions (e.g., macular degeneration or inflammation of the eyelids), and in one 1976 study was combined with antibiotics to successfully treat inflammatory infections of the anterior (front) part of the eye.
Additionally, according to multiple DMSO authors, pink eye (e.g., a virus) will resolve after a few applications of DMSO.
Sinusitis
DMSO has often been observed opening blocked nostrils within a few minutes due to its antibacterial and anti-inflammatory effects, which allow it to reduce swelling in the sinuses and promote the healing of inflamed tissue. In addition to the previously mentioned studies where it showed benefit for sinusitis:
•A 1967 DMSO study included 7 female patients (aged 43-66) who had had sinusitis for 1 week to 9 months and received DMSO. Of them, 2 had a good response to it, and 5 had an excellent response. Likewise,
•For sinusitis, Merck’s 1965 investigator guidelines stated:
A dilute solution to the nasal mucosa has resulted in the discharge of a great deal of infected material from the sinuses and the relief of pain.
•Rhinoscleroma is a rare chronic infection of the upper respiratory tract, particularly the nasal cavity that is caused by Klebsiella rhinoscleromatis and can require drastic surgery. This researcher reported DMSO can dissolve the bacteria’s polysaccharide capsule, greatly increasing their sensitivity to antibiotics and a patient's response to antibiotic therapy. That researcher authored a 1968 study which included a series of 25 patients who all were cured by DMSO plus antibiotic therapy, during which diseased mucous tissues began falling away during the second week of treatment (and a combination of DMSO and prednisolone was used to prevent scar tissue from forming in the respiratory tract). Long-continued monitoring of the patients showed no acute ill effects of treatment on the blood, urinary tract, respiratory system, eyes and ears.
•A 1992 Russian study found administering 10% DMSO to the sinuses followed by local oxygenation, within 2 years, 49 out of 52 children had a complete recovery (including all cases of maxillary sinusitis) whereas many controls receiving standard treatments did not.
Note: Stanley Jacob MD (a pivotal DMSO researcher) reported having “excellent results” using DMSO to treat sinusitis.
Dentistry
Many people find DMSO to be an excellent mouthwash or toothpaste, and when DMSO is used on the gums, they are much less likely to bleed (discussed further here). Additionally, DMSO can often relieve pain from a toothache until a dentist is seen, and pain in the oral cavity can be alleviated by swilling the mouth with a DMSO drink solution.
Likewise, some dentists in practice find DMSO (or DMSO combined with an antibiotic) very helpful for pain, infections, and swelling in the mouth, as well as for saving teeth that are starting to loosen from periodontitis. In turn, three authors have reported on dentists using DMSO in their practices:
•Stanley Jacob reported on a Portland dentist who specialized in restorative work and found that applying DMSO after a dental procedure consistently eliminates the pain (from intrapulpal inflammation) that some patients often experience after dental (even in those who have undergone a full day of restorative work.
•Another author reported other dentists use DMSO in a similar manner (e.g., for pain, infections, and swelling issues or after teeth extractions—where it is either applied to the gum or outside on the cheek or on the jaw next to the extraction site) and frequently combine it with other medications (e.g., antibiotics). Additionally, he cited a dentist in New York who applies DMSO to areas that will be x-rayed to prevent the damage the x-ray could cause (as DMSO has been shown to do this).
•Another author reported that pioneering dentists are dropping DMSO into empty tooth sockets after extractions, especially those for wisdom teeth, as it stops post-extraction swelling.
A variety of papers have also been published on DMSO’s value in dentistry:
•A 1969 Polish study followed, this evaluated 32 male and female patients (ages 18-45) with periodontal disease. In 13 of the patients, the disease only involved bleeding and swollen gums. In the other 19, the oozing and painful pockets of infection extended deep into the gum, sometimes involving the dental nerve, bone, and loose teeth. After cleaning and repairing the teeth as much as possible, the patients were treated with DMSO every other day for 7-10 treatments.
Compared to controls, this resulted in “remarkable improvements.” Specifically, there was a total elimination of pain, decreased bleeding, and gum adherence to teeth in those patients with superficial disease. At the same time, those with deep infections reported less inflammation and disappearance of painful symptoms, but none of them had very loose teeth firm up.
Note: a preliminary version of this study can be found here.
Following this, many others were also written outside of America:
•The earliest one I know of was conducted in 1968 and showed DMSO improved the pulp of monkey’s dental teeth. Three weeks later, that author then published a study that found DMSO improved 75% of pulpitis cases, while DMSO plus oxyphenylbutazone (a drug for gout) or chloramphenicol improved 85% of cases, while placebo only improved 50% of cases, and five months later published another paper on using a DMSO combination for pulpitis.
Note: this author conducted controlled studies on using DMSO for pulpitis for 10 years (e.g., he also published this, this, this, and this study).
•A 1972 study and a 1973 study by the same authors found DMSO increased the sensitivity of gingival (gum) infections to stretomycin.
•A 1981 study found DMSO mixed with azathioprine treats periodontosis.
•A 1981 study mixed DMSO with oxacillin and ectericide was able to significantly accelerate the healing of a dry socket (an unhealed wound following a dental extraction).
•A 1983 study of 222 people (176 had acute serous limited pulpitis and 46 — chronic fibrous pulpitis) found 70% DMSO placed into cavities was effective in 98.4% of acute cases and 89.3% of chronic cases, and that in most cases, this benefit persisted. Additionally, of 9 of the 16 cases with chronic fibrotic pulpitis benefitted from DMSO.
•A 1983 study found 15% DMSO mixed with a herbal extract treated periodontal disease.
•A 1986 study found a DMSO containing paste treated deep caries.
•A 1987 study showed how DMSO mixed with indomethacin can treat generalized periodontitis
•A 1987 study found DMSO helps deep caries and acute focal pulpitis
•A 1988 study of adolescent patients found DMSO plus procaine treated chronic parenchymatous parotitis (inflammation of the salivary glands).
•A 1993 study found DMSO plus short-acting insulin and 5% calcium pantothenate (B5) safely treated 42 patients ages 23 to 62 with chronic parenchymatous parotitis.
•A 1998 study found 50% DMSO with 2.5% orthophene stopped type I and type II autoimmune inflammation in the periodontium..
Tuberculosis
Despite over a century of work, Tuberculosis remains the worlds most deadly microbe (e.g., in 2023, it was estimated to have killed 1.25 million people). This is largely due this tiny bacteria’s unique characteristics making chronic tuberculosis infections quite challenging to eliminate and its high aptitude for developing resistance to the antibiotics that eliminate it.
Because of this, once the early DMSO researchers realized that DMSO could remove antibiotic resistance, their focus immediately went to tuberculosis (a decision which has also been influenced by the recognition DMSO is more effective at eliminating smaller bacteria). In turn, a variety of studies have demonstrated DMSO’s utility for this challenging infection.
Non-Human Studies:
•According to Stanley Jacob, at a 1966 DMSO symposium, it was reported that pretreating tuberculosis bacteria in 5% DMSO made them 200 times more sensitive to streptomycin.
•A 1974 study of guinea pigs infected with isoniazid resistant tuberculosis found that while all guinea pigs treated only with isoniazid died within 80 days (with tuberculosis throughout their tissues), if a single oral dose of DMSO was given 2 weeks prior to isonizaid, they all survived (and a year later were still alive). This suggested DMSO could remove tuberculosis’s resistance to isonizaid. In a followup 1976 study, they then took cultures from tuberculosis patients and found that 5% DMSO made 19 of the 61 isonizaid resistant strains become susceptible to isoniazaid and 19 of the 19 rifampin resistant strains susceptible to rifampin.
•A 1980 study found that DMSO and 5-fluorouracil enhanced the antibacterial effects of isoniazid and streptomycin on tuberculosis bacterial cultures.
Note: DMSO has also been shown to prevent rifampin from degrading for at least 8 months, which suggests it will not disrupt the antibiotic’s potency if administered concurrently
•A 1995 study found DMSO combined with a tuberculosis antibiotic (which was washed away prior to applying other antibiotics) made multi-drug resistant tuberculosis (both in test tubes and within macrophages) much more susceptible to other tuberculosis antibiotics (isoniazid rifampicin and streptomycin). Specifically, non-lethal doses of ethambutol and 2-5% DMSO caused a 4-64 fold increase in the sensitivity to other antibiotics (4-16X for rifampicin, 16-33X for streptomycin and 4-16X for isoniazid), while isoniazid and 2.5% DMSO caused an 8 fold increase in susceptibility to other tuberculosis medications.
To quote those authors:
Our data indicate that the agents that modify cell wall permeability can enhance the susceptibility of multiple drug resistant strains to drugs to which they were originally resistant. This could provide a new approach to treating drug resistant tuberculosis.
Note: ethambutol works by inhibiting tuberculosis cell wall synthesis, thereby removing its barrier to other antibiotics entering.
•A 2013 study found 50% DMSO caused an approximately 50% decrease in mycobacterium tuberculosis growth.
Additionally, a 1982 study tested 27 antiobiotic resistant isolates of myobacterium avium-intracellulare, finding that 27% were resistant to rifampin and streptomycin, 81% resistant to isoniazid and ethambutol and 96% resistant to ethionamide. Once 2.5% DMSO was used as well, all the antibiotics affected 26-30% more cultures (except for ethionamide, which only had an 11% increase, going from 96% being resistant to 85% being resistant). Three isolates were inhibited only in the presence of DMSO plus a drug, six isolates demonstrated growth inhibition without any enhanced effect due to DMSO, while the remaining eighteen isolates were sensitive to at least one drug in the presence of DMSO and to different drugs in the absence of DMSO.
Note: tuberculosis is also a mycobacterium, and the antibiotics tested in this study are also used to treat tuberculosis.
Human Studies:
•A 1969 study of 32 patients with destructive pulmonary tuberculosis and endobronchial tuberculosis gave them nebulized streptomycin and penicillin mixed in 10% or 25% DMSO. Of the 32, 14 showed an absence of tuberculosis secretion and most showed improvement (e.g., reduced endobronchitis, perifocal infiltration and lung tissue destruction).
•A 1980 study used DMSO to treat children with pulmonary tuberculosis.
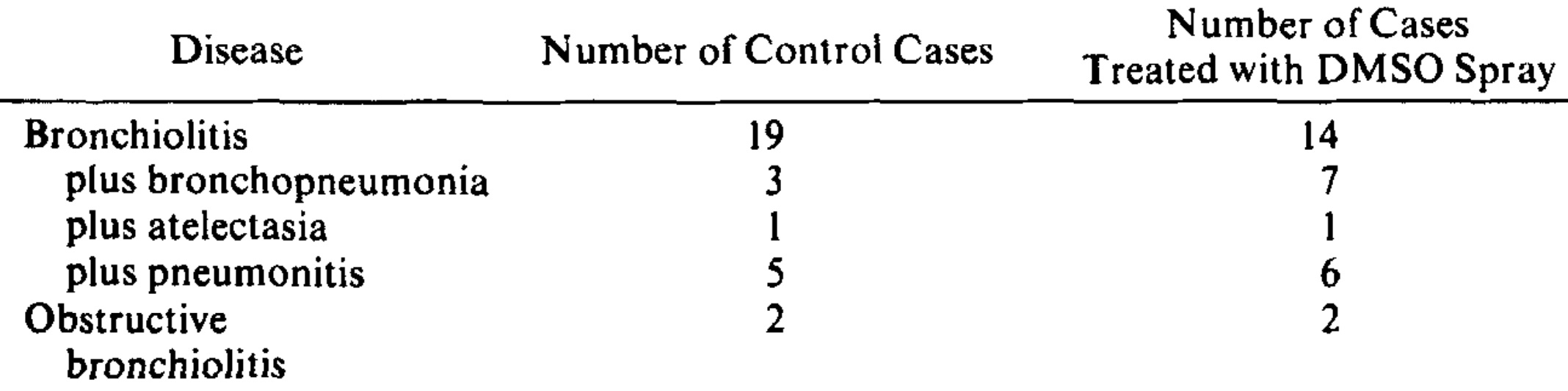
•A 1991 study found nebulized DMSO mixed with rifampin over 1-2 months was an effective treatment for 148 pulmonary tuberculosis and 18 obstructive bronchitis patients (e.g., it healed the destructive cavities caused by tuberculosis), that it could be used alone or to enhance the efficacy of conventional therapies and that DMSO significantly reduced the chronic liver toxicity of rifampin.
Additionally, one complication of the (live) tuberculosis vaccine is that it can cause recipients to form tuberculosis like abscesses (especially if the vaccine comes from a hot lot). A 1994 study of 287 children with either abscesses or regionally inflamed lymph nodes following tuberculosis vaccination who receiving isoniazid (a common antibiotic for tuberculosis) found that locally administering a rifampin DMSO mixture halved their recovery time, reduced the number of isoniazid injections and eliminated the need for other antibiotic therapies.
Bacterial Toxins
One of the primary reasons bacterial infections sicken and kill is because of the toxins they release. DMSO in turn, has been repeatedly shown to mitigate this. For example:
•DMSO has been shown to protect the duodenum from H. pylori induced chronic ulcers.
•In rats, DMSO was shown to create a dose dependent reduction in the fluid secretion and mucosal permeability triggered by C. difficile’s toxin (with its maximum inhibition occurring at a 1% concentration). Given how common C. difficile colitis is and how low of a DMSO concentration was needed to create this effect, this application of DMSO has a great deal of promise.
•The shigella bacteria’s toxin causes severe diarrhea and bloody stools (and sometimes severe illness) by destroying the cells that line the colon. DMSO was shown to prevent cellular uptake of the toxin and partially reduce its cellular toxicity.
•Endotoxaemia occurs in response to bacterial lipopolysaccharide (LPS) entering the bloodstream and is one of the most severe and ubiquitous disease processes in horses. A 2008 study of 18 horses found DMSO reduced the fevers that followed artificially induced endotoxemia. This is highly relevant to humans as LPS is highly inflammatory and can create a variety of severe disease states (e.g., sepsis). Unlike many agents, DMSO can protect cells from the damage this toxin causes.
Note: one of the most important characteristics the early adopters of ultraviolet blood irradiation recognized about it was that UVBI could effectively neutralize toxins in the bloodstream (a property which saved a significant number of lives).
Severe Infections
In addition to tuberculosis, DMSO has shown promise in addressing a variety of other life-threatening infections and severe internal infections which often require prolonged hospitalizations. This, in turn, has led to DMSO authors (who’ve seen many remarkable cases of DMSO being used in this manner) stating that DMSO should be the standard of care for severe infections, particularly those not responding to antibiotic therapy.
Sepsis
•In patients who survive heart attacks (and are brought back to life) they frequently have a variety of complications. In a 1982 study of 42 severely ill patients who had septic complications of post-resuscitation disease, IV DMSO was an effective therapy, even in cases where sepsis came from antibiotic resistant bacteria.
•A 1984 Russian study reported that DMSO was quite useful for critically ill patients with a variety of septic infections and that DMSO accelerated their recovery.
Note: one author cited a case of a septic patient with a severe bladder infection who did not respond to antibiotics but recovered once he began taking one teaspoon of DMSO three times a day.
Lung Infections
•A 1962 article and a 1974 article discussed using DMSO to treat suppurative lung diseases (e.g., chronic infections with pus in the lungs), while a 1981 study also used DMSO to treat bronchopulmonary infections.
•A 1975 study used a DMSO spray containing y-ketophenylbutazone (an anti-inflammatory NSAID), moroxydine (an antiviral) hydrocortisone, lidocaine, n-propylcarbinol, and 1-butanol (which has antibacterial properties) that roughly 2mL of was sprayed it into the mouth and throat each day. It was given to 30 fairly-ill infants (most of whom were 1-6 months old) with respiratory diseases (concurrently receiving ampicillin) until they recovered, which was typically in 1-2 days and never more than 4.
There was a significant improvement in the DMSO group (e.g., the rapid breathing and respiratory distress improved within 30 minutes and became practically normal within 24 hours, thick obstructive secretions fluidified so the infant could expel them, steam tents were no longer needed for the infant and their general condition significantly improved). Likewise, their time to recovery was much faster than the controls.
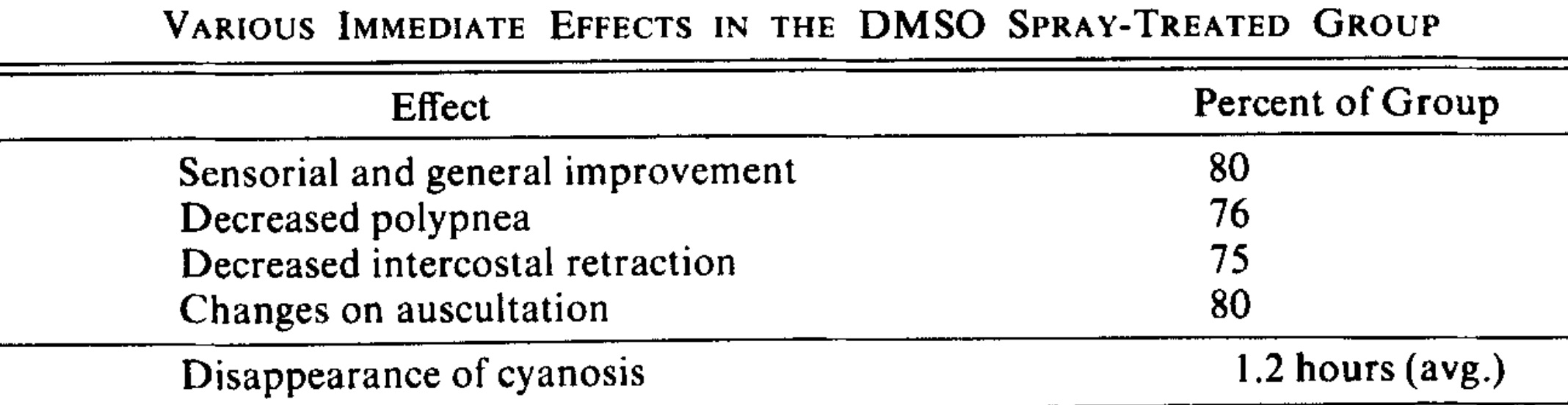
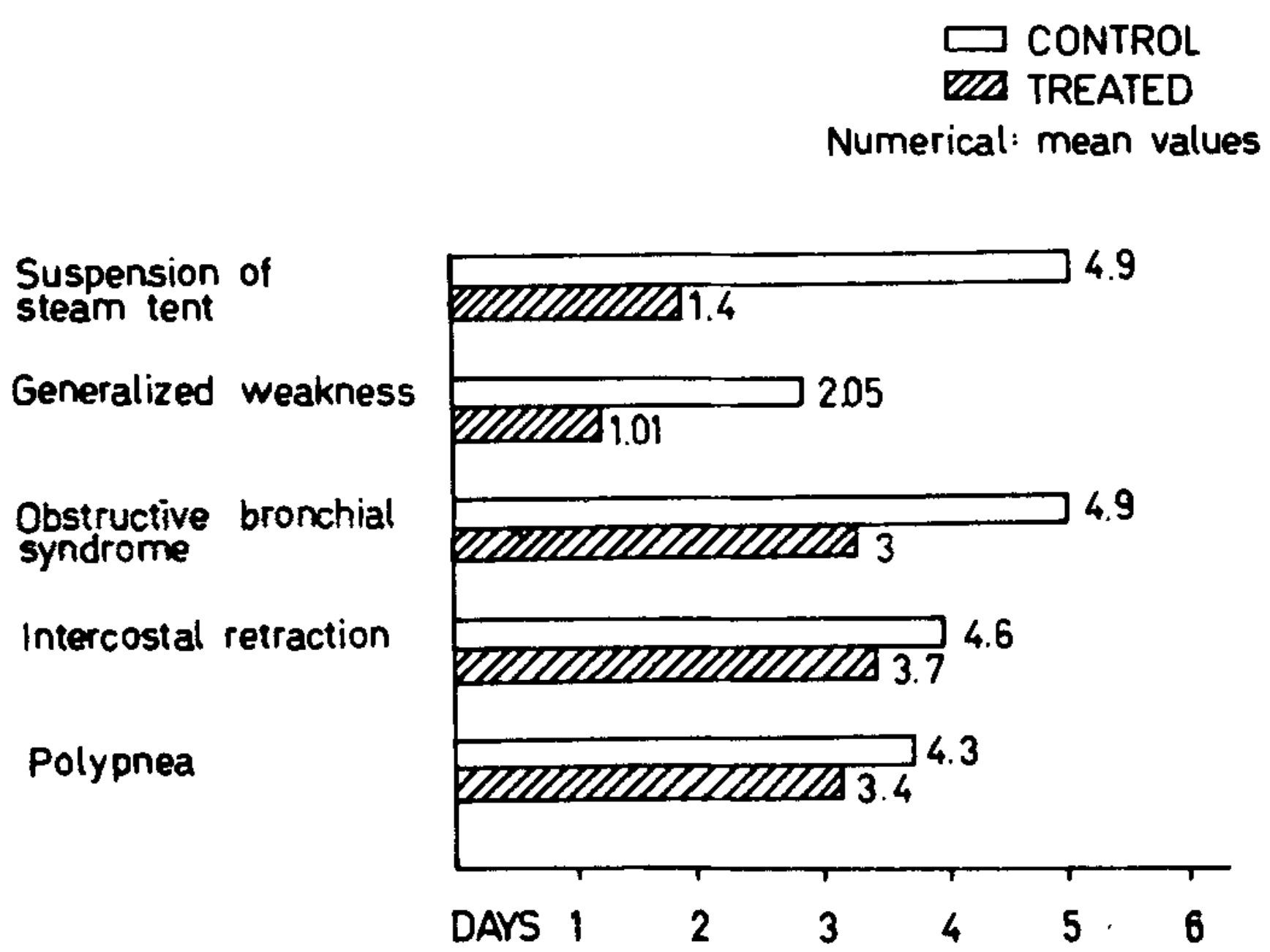
The dramatic improvements led to the authors feeling this should be the standard of care for the neonatal intensive care unit.
•A 1978 study used DMSO to treat pleural empyemas (pockets of pus accumulated in the space between the lungs and chest wall).
•A Libyan hospital, in 2020, reported that in the last 10 years, 20% DMSO and ceftriaxone were administered to 31 out of 39 lung abscesses, all of which had a complete recovery and no recurrence over the 6 to 12 months they were followed. In 16 cases, DMSO was given through a chest tube (being used to drain an empyema communicating the abscesses), in two cases it was administered directly into the abscess (via a chest tube), and in 13 cases, it was done through an endotracheal cannula (which resulted in a shorter hospital stay than chest tube administration). Additionally, in 4 of these cases, either decortication or a lobectomy (lung surgery) were also done.
Note: DMSO has also been repeatedly shown to effectively treat Acute Respiratory Distress Syndrome, a challenging lung condition that frequently follows severe infections and often requires ventilation.
•A 2023 clinical trial gave an oral DMSO spray containing zinc iodide, ginger extract, propolis extract and xylitol to patients with mild or moderate COVID-19. Compared to placebo, this treatment caused significant improvements in clinical symptoms, recovery time, and viral clearance.
Abdominal Infections
•A 1974 study used DMSO and antibiotics to treat peritonitis.
•A 1975 study used DMSO and antibiotics to treat abscesses in the abdominal cavity.
•A 1978 study used DMSO in the treatment of purulent peritonitis. Its author then conducted a 1981 study that found injecting DMSO mixed with kanamycin into the peritoneum caused it to concentrate in the peritoneum (e.g., increasing its concentration 3-8 times, and delaying its diffusion into the rest of the body so that it was retained 10-13 hours longer there), particularly in animals with peritonitis (inflammation of the abdominal lining). Given what I know about DMSO, I find this effect surprising. Still, it makes quite valuable for the treatment of peritonitis (a dangerous infection that, with hospital care, kills 13.16% for patients under 50 years and 33.33% of patients over 50 years).
Note: the above author also evaluated DMSO’s effect on the absorption of penicillin from the abdominal cavity and the specific DMSO sensitivity of the bacteria causing peritonitis.
Additionally, cutting off the blood supply to the small intestine will rapidly cause the tissue there to die and often rupture (leading to fatal peritonitis). In rats, giving IV DMSO to rats after 30-60 minutes of the intestinal blood supply being cut off, resulted in 28 out of 29 not developing gangrene, and within 24 hours, there was no evidence of ischemic damage to the intestines.
Meningitis
•A 1978 study found DMSO was an effective treatment for meningococcal infections.
•A 1987 study used DMSO combined with a nuclease to treat meningitis or meningoencephalitis caused by an acute viral respiratory infection.
Osteomyelitis
For a variety of reasons, infections of the bones can be quite challenging to treat and often become chronic. Fortunately, DMSO addresses many of those reasons, and over the years, a lot of compelling data has emerged for this application:
•A 1976 study of 132 children with acute osteomyelitis found mixing 33% DMSO with antibiotics was a highly effective therapeutic method.
•A 1980 study gave 129 newborns with epiphysial and meta-epiphysial osteomyelitis DMSO and hyperbaric oxygen therapy (HBOT), which improved their general condition, normalized serum laboratory values, reduced bone destruction, and accelerated bone regeneration. Identical results were achieved in a 1978 study of acute and chronic osteomyelitis, a 1979 study of 43 children with chronic osteomyelitis, and a 1981 study of 54 children with acute septic osteomyelitis (where reduced tissue edema was also seen).
•A 1986 study reported that DMSO (in conjunction with antibiotics) markedly improved chronic osteomyelitis due to an improved white blood cell response to the infection.
Surgery
For example, a surgeon colleague recently shared this story with me:
I had a horribly contaminated foot wound on myself down to muscle from a rusty lid of my sewer system ~5cm long. I washed it out, sewed it up, and used the DMSO along the wound edge. It took care of the pain and the wound has healed at least twice as fast as I would’ve expected. It’s been ‘fun’ to experience.
This in turn, touches upon three of the major issues encountered in surgery:
•Surgical wounds (or burns) become infected before they seal and heal.
•Infections deep within the body need to be cut open so the infection can be drained or removed (or have antibiotics directly applied to it).
•Infected tissues must be removed (e.g., amputated) because the infection within them can’t be reached or addressed.
Fortunately, DMSO is uniquely suited to address each of these (e.g., in this article, I discussed how many studies and reader testimonials show DMSO is a remarkable therapy for burns and wound healing, and here I reviewed the wealth of evidence that DMSO is a highly effective therapy for surgical scar healing).
Likewise, as I’ve shown, DMSO makes reaching a deep infection within the body possible without surgery. Numerous studies, in turn, demonstrate that DMSO can prevent and treat those infections. For example:
•A 1978 surgical study used DMSO in combination with antibiotics to treat inflammatory infiltrates.
•A 1984 study used DMSO to treat surgical wound infections.
• An 1985 study found that injecting DMSO after severe mechanical trauma reduces the risks of a subsequent infection, while a 1984 study found that DMSO plus antibiotics prevent open wounds in the hands from developing purulent infections.
•A 1990 study of 33 patients with phlegmons (inflamed areas under the skin) throughout the body found that a dressing with DMSO and silver nitrate, when compared to those receiving standard treatments, reduced the time required to begin a surgical repair by 2-2.5 times.
•Authors of a 1998 Russian paper stated that they routinely apply DMSO to surgical wounds as it accelerates healing and provides general infection control. This is congruent with the studies mentioned earlier in this article that show DMSO improves the healing of surgical wounds.
Likewise, there are numerous cases of DMSO being able to prevent an invasive surgery or amputation, such as a 1969 case report of a patient with a chronic Scedosporium apiospermum infection (a challenging fungus that did not respond to antifungals of the time and often requires amputation) complicated by bacterial osteomyelitis declined a foot amputation and was offered an experimental DMSO treatment (where the antifungals were dissolved in 60% DMSO). The patient fully recovered with no side effects, but had a recurrence 4 months later (at which point an amputation was done).
In turn, one author shared numerous cases of severe infections that required surgery but instead were treated with DMSO such as:
•An 8 year old girl and recent immigrant who vommitted daily from what was discovered to be internal bleeding and an intestinal blockage due to a severe fungal infection. After anti-fungal medications were tried without success, surgery was planned to remove the colonized intestines. As a last resort, she drank DMSO with diluted aloe vera, and three days later the vomiting disappeared (so she stopped). After it came back a week later, she then resumed treatment for 2 weeks and had no further recurrences.
•A patient who had an infection under the scalp who was told it would require a partial surgical removal of part of the scalp the expose the infected area and remove it, but the patient was able to completely eliminate the infection by applying DMSO to the scalp.
•A 43 year old man who had a crushing injury to his foot that would not heal and became infected. As the infection spread (as it did not respond to antibiotics) and an amputation was considered, IV DMSO and antibiotics were tried, leading to an immediate improvement and then a full recovery of the affected food.
•A 36 year old man who developed chronic osteomyelitis from stepping on a nail which did not heal and eventually led to an amputation being considered, but rapidly healed with DMSO plus antibiotics.
Note: that author also recounted how veterans used a DMSO lotion to treat jungle rot, a challenging polymicrobial ulcer that persisted for years and did not respond to conventional treatments (which led one doctor to believe it was the best treatment for the condition).
Other Bacterial Infections
DMSO has also helped with a variety of other infections (and as I’ve discussed throughout this series, the inflammatory complications of many infections (such as sterility). These include:
Skin Infections:
Note: many other studies also show DMSO’s value in treating skin infections (e.g., it’s extremely useful for a wide variety of chronic ulcers, as they often become infected due to their poor supply).
•A 1967 study gave 23 leprosy patients with tuberculoid markings who had been on dapsone for 6 months to 5 years were given either dapsone, isoniazid, or paraaminosalicylic acid mixed in 70% DMSO. In almost all patients, a rapid, marked and relatively equal improvement occurred, suggesting the improvement was due to DMSO rather than the antibiotic.
•A 1988 study used DMSO and methyluracil to treat erysipelas (a form of cellulitis), and likewise a 1981 article used DMSO to treat this condition.
•A 1980 study discussed DMSO’s use in treating suppurative wounds (wounds discharging pus) and a 1987 study discussed its use for treating suppurative-inflammatory diseases of the skin and subcutaneous tissue. Likewise, a 1962 study used DMSO, papaya enzyme and nitrofurazone to treat suppurative wounds.
Orchitis and Epididymitis
In 1986, a Russian physician reported that ochiepididymitis (inflammation of the testicles and where sperm are stored), a condition which can cause sterility (and follows certain infections), had an excellent response if DMSO was used as an adjunctive therapy.
Veterinary Infections
Note: there are a large number of veterinary infections which has been treated with DMSO, so many studies are not included in this section (as I did not want to make the article too long).
•A 1967 study treated 9 cats with feline panleukopenia, a virus which has a high mortality rate (e.g., over 90% in kittens) and hence is one of the primary cat vaccines. Those cats were treated with 4ml injections of 90% DMSO alongside vitamins, antibiotics and IV fluids. There was a rapid improvement in the cats, and two-thirds survived (60% of those less than six months old and 75% of those over 6 months). In contrast, after 12 subsequent cats were treated with only the standard of care, all died.
Note: according to this author, in September 1992, at the Pharmacological and Biological Therapies panel of the newly created National Center For Complementary and Alternative Medicine, it was reported that DMSO had shown promise for treating human HIV.
•A 1971 study injected either the Sindbis or Calovo virus into mice, and after 10 minutes injected either 40% DMSO or normal saline into their abdomen. DMSO (if a virus had also been injected) was found to increase the anti-viral interferon released by the mice by 2-16 times, and to significantly reduce their susceptibility to the virus.
•A 1985 study found DMSO mixed with antibiotics was an effective treatment for poultry affected by colibacillosis (an E. coli infection).
•A 2002 study of Rhodococcus equi (isolated from pulmonary infections in young horses) found DMSO increased its sensitivity to kanamycin, amikacin, and streptomycin) and chloramphenicol. However, no benefit was seen for a few other antibiotics (e.g., penicillin).
•A 2004 study found that DMSO roughly halved the amount of antibiotic (gentamicin, ciprofloxacin, or norfloxacin) that was required to treat bovine mastitis from pseudomonas aeruginosa and dramatically decreased the amounts required for antibiotic resistant strains.
Note: many other studies (reviewed here) such as a 1967, another 1967, a 1972, a 1974, and a 1992 one all found bovine mastitis was significantly improved by the combination of DMSO and an antibiotic, including in resistant strains.
•A 2006 case report discussed using IV DMSO mixed with acyclovir to treat a horse with myeloencephalopathy (dangerous brain and spinal cord inflammation) from equine herpesvirus-1.
Fungal Infections
DMSO has some antifungal properties. For example:
•At low concentrations (1%) DMSO alone showed no inhibitory activity against the common skin fungi, while some (but not all) evidence existed that 10% and 60-70% DMSO demonstrated fungicidal activity.
•A 2013 study used DMSO and antifungal agents on six different Candida species. It found 0.5-1% DMSO had an antifungal effect, but the inhibitory effect (with or without concurrent antifungals) varied significantly.
•A 2016 study found DMSO mixed with a variety of different plant extract was a highly effective at inhibiting the growth of candida infections isolated from patients with mouth cancers (whereas it was resistant to many antifungals).
Likewise, DMSO can effectively bring antifungals to many parts of the body. DMSO for instance was shown to significantly increase the amount of ketoconazole that entered the brain, which is useful in fungal infections of the central nervous system, as there are fairly few antifungals which can pass through the blood brain barrier (and likewise it can be used to bring other drugs such as cancer therapies or antibiotics to the brain). Additionally, when tested with other substances that it could bring into the brain, DMSO was not observed to alter the cells lining the blood brain barrier or the brain tissue.
Note: there is some evidence suggesting DMSO is unable to bring molecules larger than 70,000 Da through the blood brain barrier.
Because of this, DMSO’s primary commerical use has been to bring antifungal medications into infections, and in doing so, has frequently produced remarkable results in both animals and humans (e.g., consider the previously mentioned foot that was saved from amputation).
•A 1965 study found DMSO’s MIC for micosporum (the fungus that causes ringworm) was 30%, while 50% was not sufficient to eliminate T. mentagrophytes (the fungus that causes athlete’s foot). When 90% was applied to the space between the toes twice a day for two weeks in to 8 athlete’s foot patients with a verified fungal infection, it improved the symptoms of the infection, but only eliminated the infection in 2 of the 8. They then mixed 90% DMSO with 2% thiabendazole (an antiparasitic with antifungal activity) and applied it in the same manner once a day for 14 days to 16 patients, all had an excellent response, and the fungus was eliminated in 13 of the 13 patients.
Note: many since then have stated DMSO is an excellent treatment for athlete’s foot.
•Griseofulvin is an anti-fungal that is primarily taken orally because it has poor absorption through the skin.
A 1971 study found DMSO mixed with griseofulvin transported active griseofulvin through the unbroken skin of guinea pigs (which could be recovered from inside the skin and used as an antifungal in cultures). This topical mixture appeared to treat trichophyton mentagrophytes (ringworm) infections, but it was hard to be certain given the condition's tendency to spontaneously recover. Additionally, they found at high concentrations, DMSO inhibited fungal growth.
Following this, 11 cats infected with Microsporum canis (microsporum is a fungus that causes ringworm in pets and humans), often having quite severe infections were given either nothing, topical griseofulvin, topical DMSO, oral griseofulvin, or the DMSO griseofulvin DMSO combination. The first three did nothing, griseofulvin cured the cats in 21-42 days (typically around 30), while the topical DMSO griseofulvin combination fully treated the cats in 5-10 days (typically under a week). The primary issue the investigators ran into was the mixture would harden after every 3-4 days (requiring it to be remixed) which they believed was due to the binders present in commercial preparations.
Note: a 1974 study also used a 5% griseofulvin DMSO mixture to treat a microsporum (ringworm) infection in the glabrous skin (e.g., the hands and feet).
•A 1977 study found DMSO (in combination with lidase) was a highly effective treatment for actinomycosis of the face and neck.
•A 1991 guinea pig study found that applying ultrasound to topical amphotericin B (a powerful antifungal) increased its penetration into the skin, but a larger effect was seen when DMSO was applied to the skin prior to amphotericin B being applied (without ultrasound).
•A 1997 study gave 30% topical DMSO ointment mixed with 1% itraconazole (an anti-fungal) to 9 horses with fungal infections of their corneas (one of whom had 2 affected eyes) every 4 hours, with 8 of the 10 eyes recovering, with treatment lasting between 16 to 53 days (on average 34.6). These results suggested this is a promising treatment for that condition.
Parasites
There is also some data DMSO can treat parasites (e.g., 3% DMSO has been shown to significantly inhibit the growth of Trypanosoma cruzi (which causes Chagas disease). However, its primary value is bringing an anti-parasitic medication to the region of infection (as parasites can often burrow quite deep into the tissues).
For example, two different 1966 studies (this study and this 25 person RCT) found that DMSO plus an anti-parasitic (e.g., 2% topical thiabendazole in 90% DMSO) was an effective treatment for hookworm infections in the skin. DMSO can also be combined with anti-parasitic medications to reach challenging parasitic infections deep within the body. For example, a 1984 case report discussed DMSO treating a complex amoeba infection of the liver.
Note: in the 25 person RCT, DMSO alone provided no benefit.
Cancer and Autoimminity
One of DMSO’s widely recognized properties is that it causes cancerous cells to revert to normal. In researching that, I came across a fascinating study that tested cancer patients for pleomorphic bacteria (something many previous pioneers of successful but suppressed alternative cancer therapies like Rife and Naessens also believed caused many cancers). While difficult to culture, pleomorphic bacteria were eventually isolated from the blood of some of them, in the blood of some of those who had been around those who had recently died from cancer for a prolonged period:
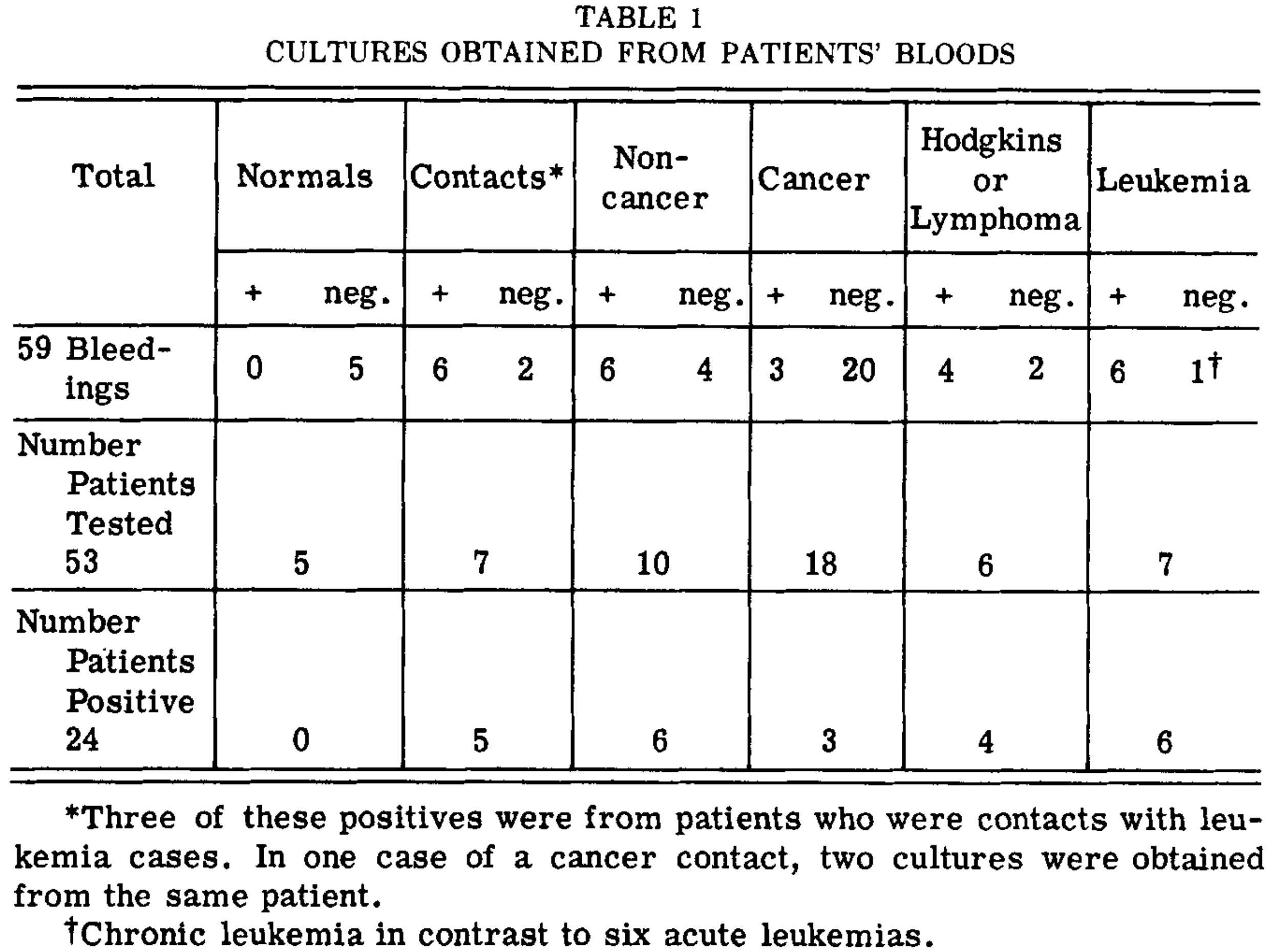
Likewise, 17 tumors were directly sampled, of which 16 yielded cultural specimens, with the negative coming from a granulomatous nodule. Additionally, one tumor had to be sampled twice as the initial specimen did not produce the bacteria. Finally, in some cases, the organisms were found directly within sampled cells.
Note: the morphology of the bacteria is extensively described in the paper, but essentially matches what many other pleomorphic researchers have found over the years.
They tested three different agents on the bacteria, ethambutol (an antibiotic), lysozyme (an enzyme present in many mucosal secretions that protects the body from invading organisms), and DMSO. They found lysozyme did a bit, but DMSO did much more.
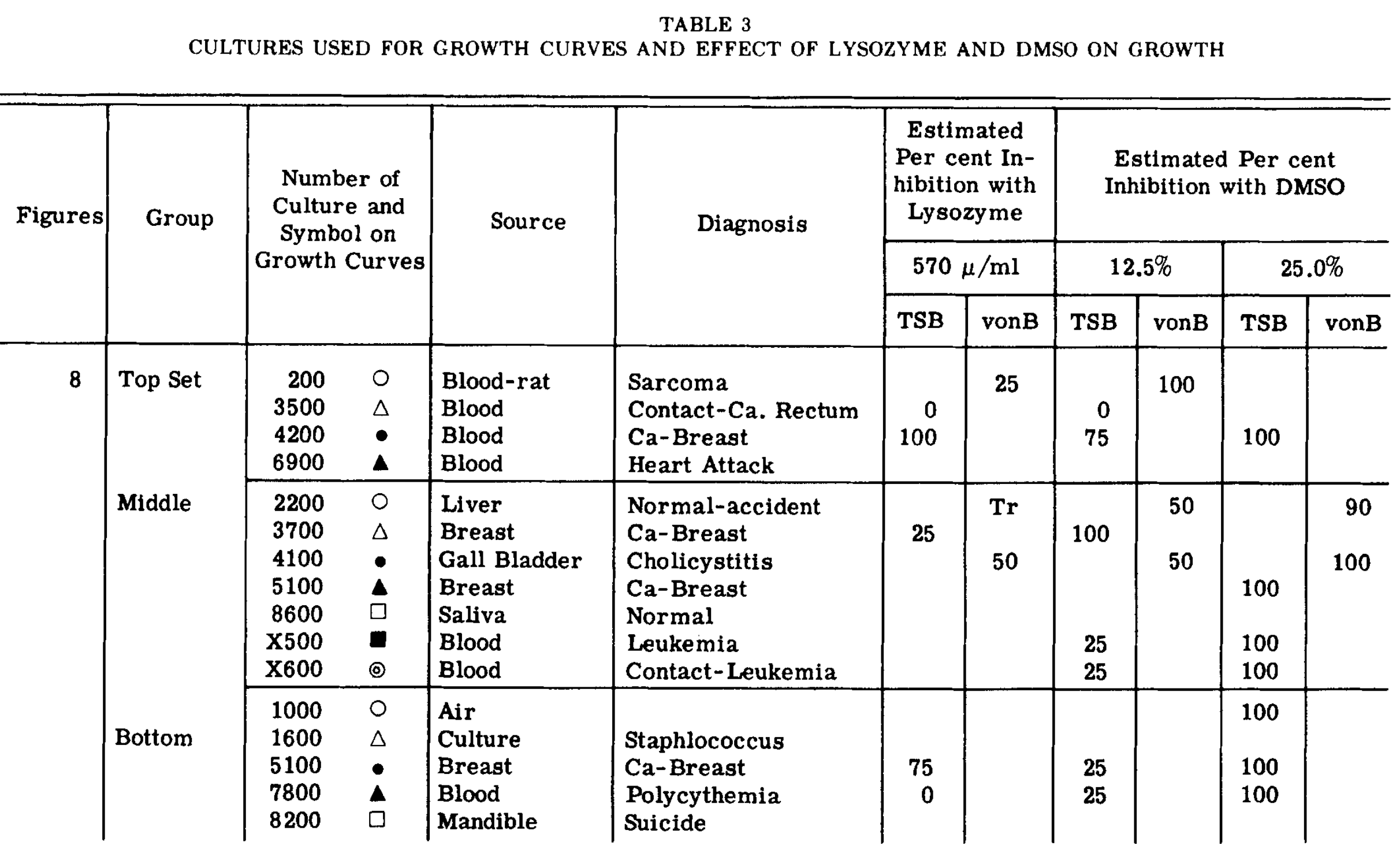
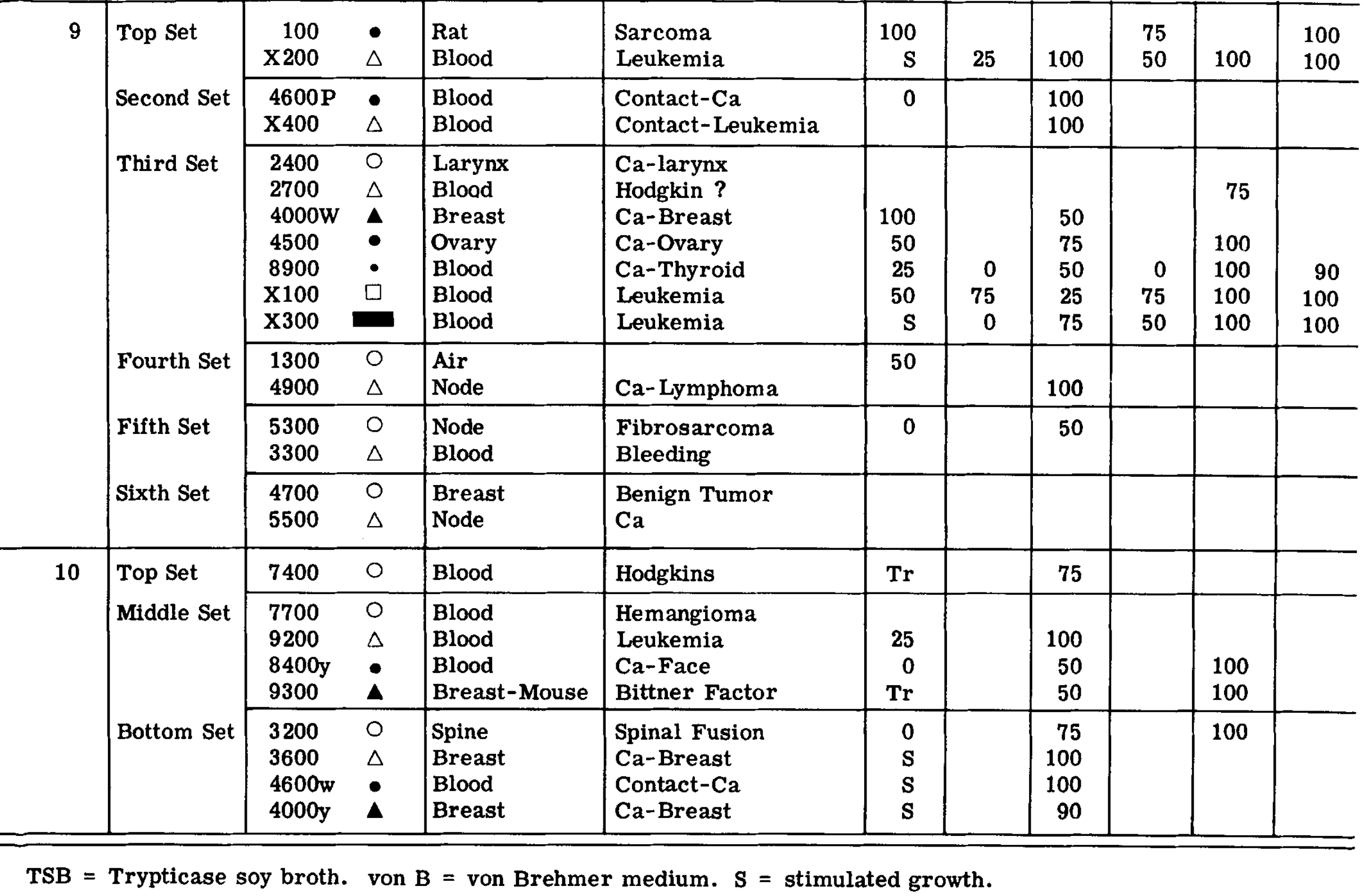
They also provided a series of growth curves that were illustrative of the effects of DMSO (one of which I annotated so you can identify what each symbol represents).
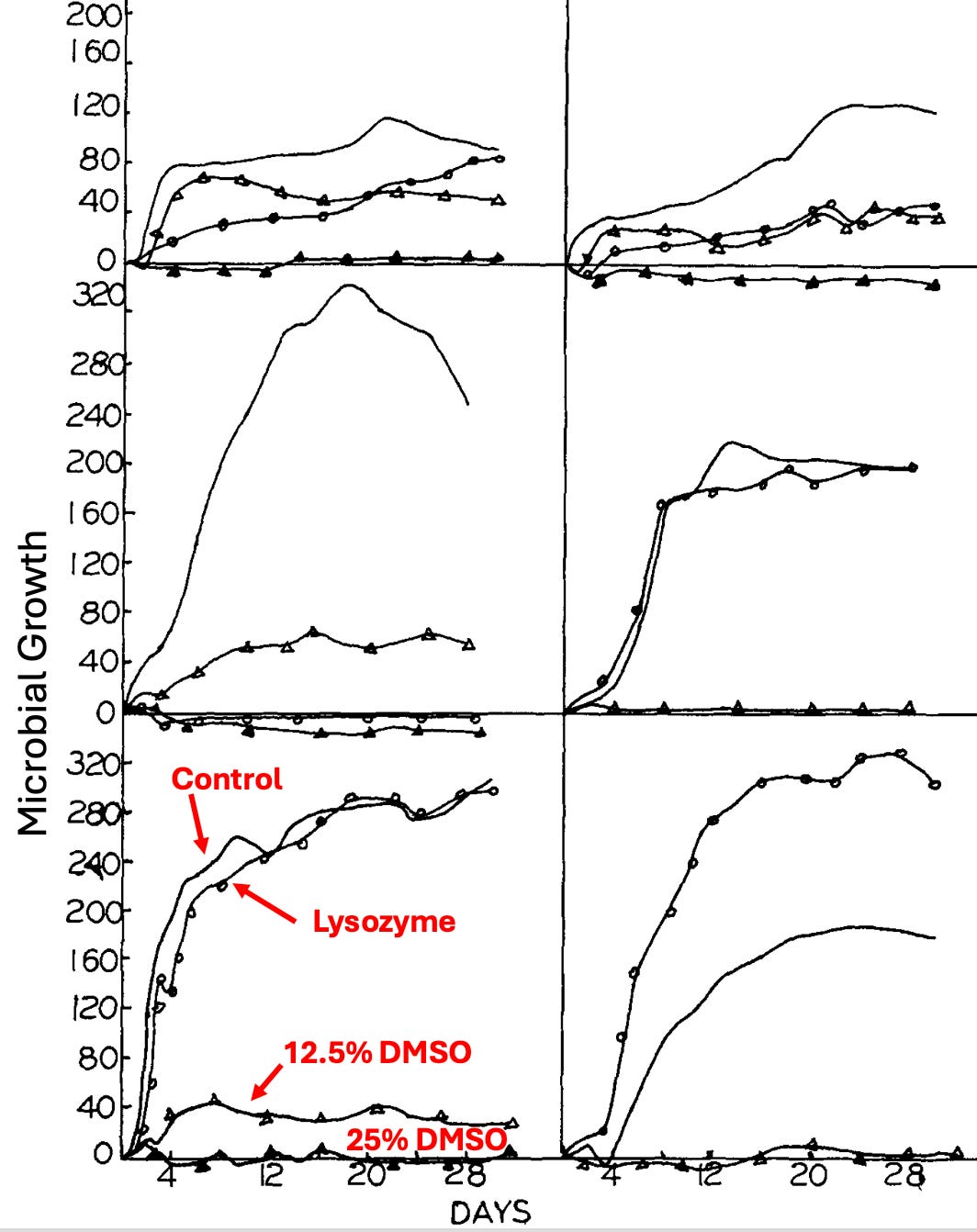
Note: when DMSO was added to fresh leukemic blood samples, it, completely inhibited the dancing motion of particles free in the blood or attached to the periphery of the crenated red blood cells (another common pleomorphic observation), but did not damage the red blood cells at all.
The pleomorphic model of bacteria (discussed further here) essentially states that bacteria can significantly change their morphology (to the point they are almost unrecognizable from their original form), that these changes are often done in response to their environment, and that some forms are relatively harmless to the body, while others cause disease. In turn, since things that kill bacteria often transform them into ones that are more pathogenic, a longtime belief within certain schools of natural medicine is that the goal should be to change the terrain of the body to encourage a benign morphology of bacteria rather than trying to kill them all off.
Note: some of these schools also believe this applies to viruses and fungi, and that, in some cases, they can transform from one type to another (e.g., a bacteria becoming fungal).
A large group of modern researchers studied this subject for decades (e.g., hundreds of research studies they conducted are summarized in this wonderful textbook by Lida Mattman). Five of their key observations were:
•Antibiotics will often fail to kill every bacteria present and then trigger those that survive to enter a primitive survival state known as a “cell wall deficient” (CWD) form resembling a mycoplasma. This process in turn, was most commonly triggered by antibiotics that attack bacterial cell walls (which characterizes many commonly used antibiotics).
•CWD bacteria are very hard to detect (most standard microbial methods will determine that no organisms are there when CWDs are present).
•When conditions are more optimal for survival, CWD organisms can revert to the active form and cause an infection that had been eliminated with antibiotics to suddenly and inexplicably recur (which, for example, we frequently see with urinary tract infections).
•Once present, CWD bacteria will often enter cells and cause chronic inflammation because the immune system will attack cells with the CWD bacteria.
•Many different unexplained autoimmune disorders (e.g., sarcoidosis) have characteristic CWD bacteria present that can be repeatedly identified from their inflamed tissue (the textbook cites an exhaustive amount of data substantiating this).
•While standard antibiotics are ineffective in treating CWD infections, non-standard ones (e.g., erythromycin or minocycline) often are, but the sensitivity to those antibiotics is highly variable depending on the causative organism.
In practice, we find 10-15% of chronic illnesses (including blood clots and cancers) have a pleomorphic etiology, but rather than try to eliminate those organisms with antibiotics (which always have side effects), we instead give signaling products derived from healthy bacteria that cause the pathologic bacteria to transform into a non-harmful form, which in those applicable cases, frequently yields remarkable results (e.g., this approach is very useful for lupus and many cancers). Likewise, I believe this model explains a longstanding belief within natural medicine that giving antibiotics for an acute infection often transforms it into a chronic illness down the road.
Note: ultraviolet blood irradiation is also quite effective at eliminating these organisms and the diseases they cause. For example, a case report discussed a cohort of 5 family members who had a variety of chronic diseases (e.g., Crohn's disease, asthma, complex regional pain syndrome, hypothyroidism, type 1 diabetes mellitus, and lymphangiomatosis) and found that 4 had a MAP (mycobacterium paratuberculosis) infection. Two patients received antibiotics and UVBI, and then experienced a resolution of their autoimmune symptoms.
As I discussed recently, DMSO is well-known for being able to treat a wide variety of autoimmune disorders. In that article, I highlighted my suspicion that this cancer may partially explain that. This is due to the fact many that rheumatologic drugs also function as antibiotics, antibiotics suited to eliminating CWD bacteria also function as rheumatologic drugs (which is also essentially the case for ultraviolet blood irradiation), and that many autoimmune conditions, with the appropriate techniques, have had CWD bacteria isolated from them. In turn, I suspect DMSO’s increased toxicity to smaller microorganisms (possibly due to their lack of a cell wall) may make it uniquely suited to eliminate these microbes (while simultaneously not harming the body).
Lastly, Individuals with chronic fatigue syndrome often find relief from DMSO, which some have attributed to its antiviral properties (e.g., towards Epstein Barr). This for example, is a letter Stanley. Jacob received from a patient:
I am the victim of a rare chronic systemic virus infection, which is not recognized by a majority of the medical profession. In 1965, 1 had an acute attack of encephalitis, hepatitis, and asthmatic bronchitis so severe that mental and speech coherence were impaired and I scarcely hoped to live through the night.
The internist who had accepted me three months earlier gave me prednisone, which resulted in immediate improvement. But before the course was completed, serious symptoms of encephalitis recurred. I felt I had nothing to lose, as the next attack would almost certainly be fatal.
I tried DMSO strictly on my own responsibility. Results were truly dramatic. All symptoms diminished, and after an absence of six weeks I returned to work. Laboratory tests showed equally dramatic chemical improvement in liver and white cell count
I attribute all of my success to DMSO for not having to go through with the amputation of my right leg. I was told by several professional men I would not be able to stand the pain otherwise, and they were right. The pain was so excruciating, so severe that I bounced my head on the wall. I had to crawl instead of walking, and I took 1 5 to 20 painkiller pills a day.
Note: Readers have also reported to me (e.g., here, here, and here) that DMSO helped their chronic fatigue.
Treating Infectious Diseases With DMSO
In my writing this article, it is my sincere hope that it:
•Will inspire physicians to begin combining DMSO for challenging to-treat infections (as it opens up a new door to medicine and provides a way for doctors within a fairly conventional paradigm to treat many illnesses they struggle with).
•Provide you with the tools you can use to help your own health to deal with these challenging infections.
Fortunately, due to the multifaceted and systemic benefits of DMSO, many who used the guidance previously have already reported that DMSO also helped with a challenging infection they had. As such, in the final part of this article I will cover:
•General instructions for using DMSO (e.g., doses, sources, and updates) and disease specific recommendations.
•Non-pharmaceutical alternatives to antibiotics that can be mixed with DMSO to eliminate infections.
•Some of our other preferred approaches for treating the diseases discussed in this article (e.g., shingles, candida, or upper respiratory tract infections).
•Thoughts on some of the popular alternative antimicrobials (e.g., chlorine dioxide and many others few know about).
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.