

Dissecting the New York Times' Plea for Vaccine Amnesty
Reviewing a remarkably disingenuous "apology" and what actually caused the vaccine disaster

Story at a Glance:
•Repeatedly forcing the public (e.g., through mandates) to use unsafe and ineffective therapies (that injured millions) has created a public relations disaster for the establishment.
• Various attempts have been made to do the impossible—restore the public’s trust in our medical institutions without any of them admitting fault.
•Here, I review each of the previous attempts and how they were used to create the recent infamous article by the NYT—which while monumental for bringing attention to the COVID vaccine-injured, also repeats a variety of strategic and very harmful lies to protect the vaccine industry.
•One of the mysteries of the COVID-19 response is what could have possibly justified breaking the public’s trust in the medical institutions our society revolves around. Here I will review the most compelling explanations we’ve come across after three years of investigating this commonly asked question.
For decades, I’ve noticed propaganda campaigns in the media will subtly signal what is in the works and it’s been a longstanding challenge for me to see if I can use those signals to accurately predict the future (e.g., this is how I predicted the course of the pandemic at the end of 2019).
In organic chemistry, one of the common subjects students are tested on is chemical synthesis. In synthesis problems, students are given a set of chemical reactions that can be performed, and are then expected to deduce how a combination of those reactions can be sequentially performed to transform a starting chemical to the desired final product.
The reason it’s essentially possible to “predict” the future by studying a public relations (propaganda) campaign is that like the synthesis problems, the PR field has a fairly limited number of tools to accomplish its agenda, and as a result, if you see one step being enacted, it often cleanly fits into a 10-step campaign you’ve seen conducted before (e.g., if it matches the 4th step of the previous campaign, you can reasonably infer the 10th step will likely to come to pass in the future).
As a result, I tend to view many media campaigns as “synthesis” problems. I consider their sponsors' likely goals, the sequential steps that would need to be taken to enact those goals, and then see if what I’m currently observing fits into one of those sequences.
In turn, I’ve been amazed at how frequently this process has allowed me to know what’s in the pipeline, and over the years, I’ve reached a few key conclusions:
1. Synthesis problems are something college students typically struggle with (while not that complicated, they differ from the typical “first-order” thinking students are typically tested on, where they are just expected to memorize things and then regurgitate them). I believe this same blind spot is what prevents people from recognizing that when the same propaganda “synthesis” campaigns are conducted in the media again and again.
2. While propaganda is incredibly effective and appears monolithic (e.g., consider the complete insanity it made people unshakably believe throughout COVID-19), the majority of people who orchestrate it typically aren’t that intelligent or creative. Instead, they tend to use the same proven steps again and again, which while not optimal, are effective enough to accomplish their goals because they always have the weight of the mass media behind them.
Note: one of the best illustrations of this was Trump’s interactions with the media, as he regularly gave the response which effectively countered the current PR campaign against him. Yet rather than adapt and effectively respond to Trump’s response, the entire media would double-down on its initial message, frequently leading to their PR campaign boosting rather than undermining Trump’s popularity. Yet, despite this approach clearly not working, the media kept on doing it, which I took as a sign their adaptability within their campaigns was actually quite limited.
3. One of the biggest “red flags” for me is seeing a propaganda campaign unfold that is structured in a significantly different way from the baseline I’ve come to expect from watching previous iterations of those campaigns.
For example, I am used to the media whipping up hysteria about an inconsequential infectious disease (e.g., bird flu) every few years. The key thing which told me COVID was going to turn into a global disaster was the fact during the first few months (November 2019-March 2020) the media instead downplayed it as much as possible (e.g., the “it’s just a flu bro” meme was everywhere and anyone who raised concerns about it was accused of being racist towards Chinese people). Given that the entire biosecurity apparatus has been begging for something like COVID-19 for decades to justify their existence (and funding), the fact that they were downplaying it signaled that something much more nefarious was in the works.
Note: years ago, I learned that Corporate America would often commission “Tiger Teams” composed of talented employees to solve a problem (e.g., how to monopolize a sales market), and like tigers tearing apart a piece of meat, relentlessly attack the problem until a solution was found. Since these “solutions” often required complex multi-year campaigns, it was easy for me to wrap my head around the idea that PR firms would conduct similar endeavors.
The COVID Vaccine Campaign
When I observed the campaign used to sell the COVID vaccines, a few things jumped out at me:
•A lot of work went into setting up the campaign (e.g., the lockdowns, the messaging around the lockdowns, an immense effort to discredit any off-patent therapy that could treat COVID-19, and historically unprecedented online censorship to monopolize the narrative).
Note: the key thing all of the approaches we took to “addressing” COVID-19 had in common was that they were useless, and in many cases made things much worse.
•Before the vaccines came out, we repeatedly heard messaging stating that if you felt awful, that meant “it was working.” This for context was not something I’d heard from any other vaccine.
•The campaign was done in sequential stages where once a “softer” approach (e.g., gift cards) had maxed out how many sales it could get, a “harder” one was immediately implemented (e.g., pseudo-mandates like being unable to go to concerts without being vaccinated).
•Give or take, every stop that could be pulled out was used to sell the vaccines. Before long, this included ridiculous things like Krispy Kreme giving everyone who was vaccinated a free donut each day for the rest of the year, and CNN not only covered it but also covered it again when this was changed to two donuts rather than one. Not long after, it pivoted to draconian mandates that permanently broke many people’s trust in the medical system.

Note: I compiled some of the most ridiculous vaccine promotions here (e.g., lotteries, drugs, alcohol, and complementary brothel visits).
From all of this, I inferred that a decision had been made to do whatever was needed to vaccinate as many people as possible as quickly as possible (as best as I can guess, due to Biden’s repeated messaging on it, the goal was 70% of Americans 6 months into the campaign). Additionally, it appeared the people who chose to push the vaccines were fully aware of how unsafe and ineffective they were,
I hence concluded that the people pushing the vaccines knew they had a limited window to get everyone vaccinated and were willing to do whatever was necessary to vaccinate the world before that window closed—even if it was immensely costly for them in the long term.
Note: as best as I can gather, the “window” was either due to people inevitably becoming aware of the adverse effects of the vaccines (particularly the medium and long-term ones), people realizing the vaccine didn’t work, or COVID-19 becoming extinct (something which happened in many of the African countries which didn’t vaccinate).
mRNA Blowback
Given all of this, it was virtually certain that there would be a lot of blowback from the vaccination campaign. For instance, a large number of Americans no longer trust vaccination (which has long been a bedrock the American medical system has relied upon), a large number of Americans no longer trust the health authorities (also a bedrock the entire system has relied upon), and there are a large number of vaccine-injured individuals (along with their family members) who are enraged at the politicians who pushed the vaccines on them.
Given the toxicity and inefficacy of the vaccines, it was essentially a forgone conclusion that an excessively aggressive campaign to deploy them upon America would inevitably lead to the consequences listed above. Because of that, something would have to be done to regain the public’s trust in the medical establishment and I was quite curious to see how accurate my prediction for how it would unfold would end up being.
For example, early in the COVID vaccination roll-out, it became clear to me the goal was not to vaccinate the world, but rather to get as many people to receive the mRNA technology as possible. Because of this, I predicted that as it was necessary, the non-mRNA vaccines would be thrown under the bus, and likewise, no criticisms of the mRNA vaccines would be allowed until their sales had dried up and there was no value to continuing the immense effort to prop-up the myth of their “safety and efficacy.”
Note: “Safe and Effective” is a meaningless (but persuasive) mass-marketing term that has been in use prior to most of us being born (e.g., in a recent article, I cited an example of John’s Hopkins professor calling out the medical profession’s abuse of it during the 1955 Polio debacle)
This in turn may explain why:
•Despite the world being locked down until a COVID-19 vaccine was found, almost no attention was paid to China deploying one in July of 2020 and another in August of 2020 (whereas the mRNA vaccines came out in December 2020). In turn, the WHO did not acknowledge China’s vaccines until May and June of 2021 (at which point the mRNA vaccines had already saturated the market) and most people in the United States still don’t know about it (since it was never licensed here). Despite that, China’s (affordable) vaccines are by far the most used COVID vaccine in the world, and are now also the most effective (as the COVID virus rapidly mutated resistance to the single antigen-based mRNA formulations—something the live attenuated ones were much more susceptible to).
•The FDA temporarily suspended the (non-mRNA) J&J vaccine in April of 2021 after 6 people (out of the 7 million vaccinated) developed a rare cerebral blood clot, and then lifted it ten days later with a press release which stated:
Agencies Underscore Confidence in Vaccine’s Safety and Effectiveness Following Data Assessment; Available Data Suggest Potential Blood Clots Are Very Rare Events
Note: blood clots, strokes, and heart attacks were common side effects of the mRNA vaccines (e.g., many of us knew multiple people this happened to and hence they were often referred to as “the clot shot”). My belief at the time was that the FDA making a big deal about how they were conducting a token investigation of a “rare side effect” was primarily done to create the perception no more serious condition could exist. In turn, I lost count of how many doctors I spoke to who insisted the mRNA vaccines could not be dangerous as the FDA was willing to act on a 1/1,000,000 safety signal for the J&J vaccine. Because of this, I believe J&J was thrown under the bus to protect the mRNA vaccines. This sadly was only one of many audacious PR moves done to protect the mRNA vaccines (e.g., the Nobel Prize was recently awarded to two people who were falsely credited with inventing the mRNA vaccines).
•The J&J vaccine was pulled from the market in June of 2023.
•The AstraZeneca vaccine was recently pulled from the market (with the media continually mentioning “AstraZeneca previously admitted in court documents that the vaccine can cause rare side-effects such as blood clots and low blood platelet counts.”).
Likewise, now that no one wants the mRNA vaccines (e.g., Moderna’s sales fell 91% this year) we are now starting to see periodic acknowledgments in the media that there are “rare” risks of COVID vaccination.
Note: one of the frequent questions we receive is how much should one be worried about the J&J and AstraZeneca vaccines. I ultimately don’t know, because while I saw far fewer J&J injuries, far fewer people received the J&J vaccine (and in contrast, almost no one I knew received the AstraZeneca one). However, we noticed long term complications from the J&J vaccine were much rarer, which we believe was due to it (like AstraZeneca) utilizing a virus that was designed to (in theory) be unable to replicate in the body and hence is eventually cleared (whereas the artificial vaccine mRNA can persist for a much longer period).
COVID Amnesty
The medical industry had a huge PR problem, and I was quite curious to see how they would address it. Since a common approach in PR is to test messages with focus groups (to see how the public will respond to them once they are blasted on every media platform), I was hence on the alert for “test runs” of their ultimate strategy.
On October 31, 2022, a semi-mainstream platform (the Atlantic) published a plea for COVID Amnesty “written” by a semi-mainstream journalist (Emily Oster, a professor who had a semi-large Substack following on “data-driven parenting” before she left this platform to protest its other authors). In it, Oster stated while she made a variety of horrible decisions during COVID (e.g., promoting school lockdowns or training her four-year-old children to scream at unmasked hikers to stay away from them) those decisions were “not her fault” because there was no way to know those decisions were wrong and she simply made the best guess she could in the face of “tremendous uncertainty” (whereas she attributed the correct decisions we made to “luck”).
For a variety of reasons, this response rubbed a lot of people the wrong way (e.g., contrary to Oster’s claims, at the time there was an abundance of data showing the COVID policies were wrong) and it prompted an uproar online which eventually prompted one person (I cannot disclose the name of) to have this flown over Oster’s house:

However, I believe the primary reason it upset so many people was because it constituted a “disingenuous apology.” Almost everyone has had a time when someone “needed” to apologize to them, but didn’t want to admit they did anything wrong, and hence tried to find some way to twist their words to accomplish this goal (e.g., “I’m really sorry about how that made you feel” places the blame on the victim’s reaction to the aggression rather than the aggression itself).
Note: since PR is often tasked with getting a client out of trouble for a past misdeed, you will frequently observe elaborate attempts to sculpt their language and reframe the situation so that they can get out of trouble without admitting fault.
When I dissected Oster’s plea for amnesty, I hence emphasized that it was a classic example of a disingenuous apology (e.g., she always used inclusive language implying both sides were at fault). In turn, I argued Oster was effectively trying to have her cake and eat it too, as she wanted to be forgiven and have the public regain their trust in the other vaccines (without even allowing a discussion of why that trust was lost), but simultaneously was unwilling to admit fault her part (and hence bear the burden of that admission) or touch on any of real issues at play.
For instance, the only “mistake” of the vaccines Osteer touched upon was people erroneously believing J&J’s vaccine was superior to the mRNA ones, whereas in her words “the mRNA vaccines have won out.” Likewise, she never discussed the disastrous hospital protocols or the suppression of early COVID-19 treatments which were the primary thing responsible for America’s high COVID death rate.
Note: one of the most famous examples of a duplicitous vaccinologist who tries to have his cake and eat it is Peter Hotez. For example, he received a massive grant to create a SARS vaccine for a lab leak (which funded the Wuhan bioweapons research) and he repeatedly denounced anyone who suggested COVID-19 came from a lab. Likewise, he continually laments the “dangerous” politicization of science and horrible attacks against scientists like himself, but continually uses “science” to politically target conservatives in much more damaging ways.
Since Oster’s insincere pleas landed on deaf ears, we witnessed a series of more candid apologies published in semi-mainstream publications (e.g., Newsweek) which again tried to regain public trust with more candid admissions (which still danced around the vaccine issue). Since I felt these represented important historical records and I wanted to track how the messaging evolved, I in turn discussed the second plea and the third one, and then patiently waited for the real one about the vaccines to come out.
I waited patiently, and last week, the New York Times at last published the first “mainstream” plea for amnesty about the vaccines. It was seen by many, and as expected, built upon the previous messaging that had been sculpted to redeem the medical system’s reputation while admitting the absolute minimal amount of guilt necessary to accomplish that objective. I will now attempt to dissect the new disingenuous plea for amnesty.
The New York Times
Before we go any further, I'd like to focus on its title, which sadly synopsizes the entire NYT article:

Note: thousands is a very clever word to use here, since if 999,900 people were permanently disabled by the vaccine, it would still be “true” but it implies a far smaller number.
When the word “believe” is used, it can have a few different meanings. For example it could be used:
•When you think something is true but don’t have the ability to back it up (e.g., I frequently use “believe” here because I think it is important to note the claims I am making that I cannot provide strong evidence for).
•To characterize something someone thinks is true an irrational belief that only exists in their head (e.g., a common way medicine gaslights patients ds by arguing the symptoms they experienced from a pharmaceutical injury are actually just “in their head”).
•When you want to acknowledge someone’s feelings to make it seem like you are doing something but divorce the discussion from any factual or substantiative grounding (something which sadly is quite common in the modern left).
In turn, I would argue the NYT was not using “believe” in the way I believe is appropriate to do and instead doing the latter two. Thus, like all good propagandists, they are attempting to find a way to twist the situation so that they can have their cake and eat it. Similarly, if you consider the other underlined phrase, it’s clear someone spent a lot of time trying to figure out how to write something that sounded like an acceptable admission and apology to those injured by the vaccines but simultaneously suggested that those injuries aren’t really a thing and there is nothing to be concerned about with the vaccine.
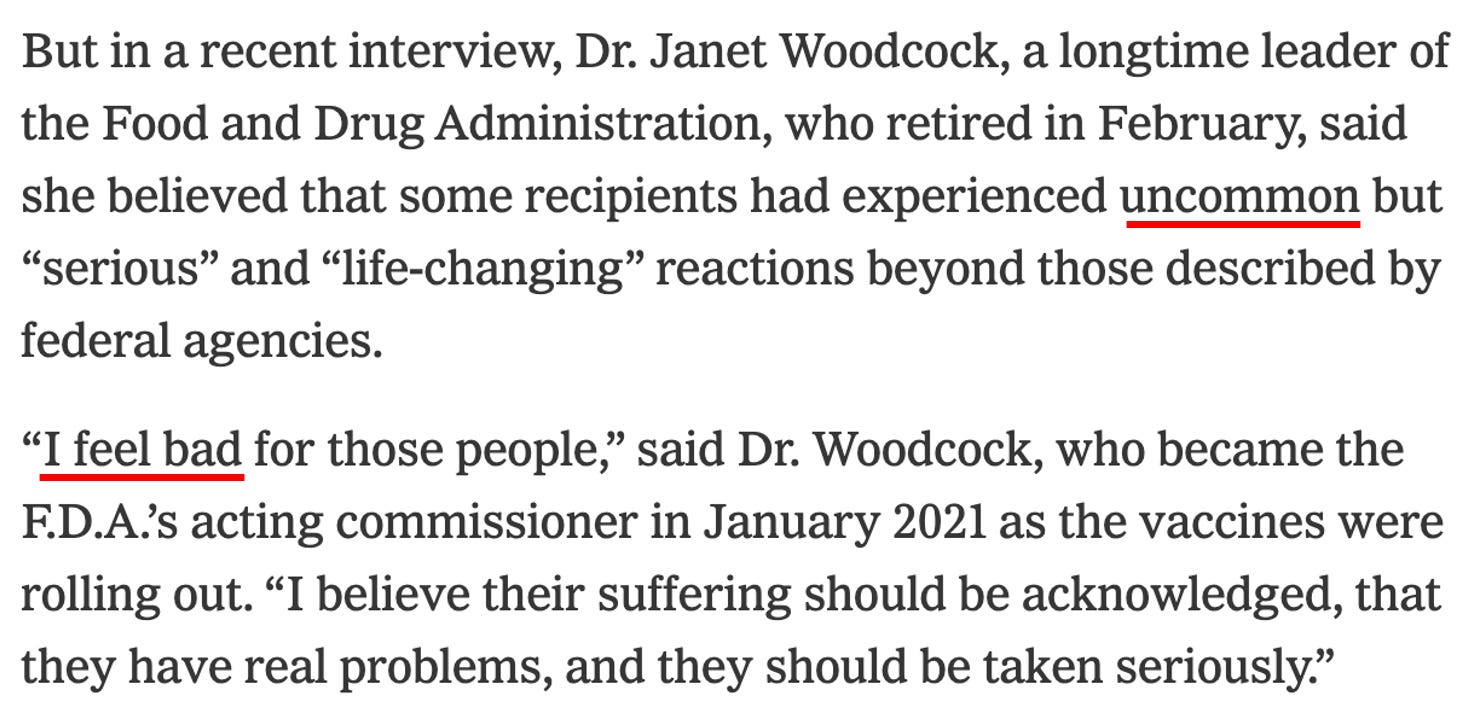
For example, after opening on the tragic story of a neuroscientist who like many other Americans was disabled by the vaccine, the NYT produces evidence that suggests (but does not state) the problem was due to production issues rather than the vaccine itself.

Similarly, here, if one reads this passage without thinking too deeply into it (which likely describes a typical NYT reader), it translates to saying a few regrettable things happened, but they aren’t a big deal because of how much the vaccines benefited humanity. Beyond this being false (they were actually one of the most catastrophic medical products in history), it’s also saying anyone who was injured was an acceptable sacrifice for the greater good.

This statement implies the majority of the thousands COVID vaccine injuries are much less severe than Dr. Zimmerman’s, when in reality, I and my colleagues know many people who would give anything to trade their current (much worse) injury for what Zimmerman is going through (e.g., assisted suicide, homelessness and failed marriages are common topics in their support groups).
To illustrate, this is one of countless (brief) videos I’ve seen circulating online, which was posted by a vaccine-injured nurse I periodically correspond with who essentially had her life taken away by the vaccines and has worked tirelessly to advocate for the people in her situation (e.g., on Twitter).
Note: it’s really hard for me to put into words how bad I feel for these people, which is why I try to repeatedly bring attention to their situation in this publication.
Note: most of the vaccine injured have over $3,600 of medical expenses each month.
This passage (without explicitly stating it), attempts to equate the 13,000 compensation claims to the number of people who believe they were injured. This ignores three key facts:
•The compensation program was not advertised and many people hence did not know about it.
•Many people did not know they had a year to apply to the program and hence missed their window to.
•Many people I talked to did not bother filing a compensation claim with the program because they knew it was an arduous waste of time (i.e., the 12 that have been “paid out” only were paid after Republicans in Congress formally complained about it). To illustrate how extreme this is, even participants in the clinical trials for the COVID vaccines who were clearly injured by the vaccines were not allowed to get compensation (or often to even associate their injury with the vaccine). As a result, private non-profits with very limited funding (e.g., REACT-19) have actually “paid out” more to vaccine victims than our entire Federal compensation system.
Note: one of the key things the pandemic profiteers (e.g., Bill Gates) pushed for was to have all liability protections removed for “emergency” vaccines so they could do things like this. In turn, the WHO’s disastrous pandemic treaty (which we are doing everything we can to stop) stipulates signatory nations must provide that same liability exemption which have devastated those injured by the COVID-19 vaccines.
I always take note of when a gaslighter uses the word “gaslighting.”
It’s worth noting that beyond numerous adverse event systems giving red flags, Steve Kirsch has spent almost three years formally sending data demonstrating serious safety issues to the Department of Health and Human Services. Likewise, he has proven they’ve ignored major safety signals (e.g., that the vaccines were killing people) ever since the vaccines hit the market, has publicized those submissions to his large audience, and has paid for a billboard in front of the CDC in order to force the Federal Agencies to respond to the data (which they have still refused to do).
The context this passage omits to mention was that the initial wave of vaccine injured (e.g., those injured in the 2020 clinical trials) repeatedly requested for Woodcock to look into their injuries, and while Woodcock initially told them she cared and the FDA needed to investigate their data, once the injuries started piling up and the government realized this was not a rare problem they could manage, they switched to ghosting those injured by the vaccines.

Woodcock’s “apology” again avoids admitting culpability, despite the Wall Street Journal article showing that she was directly responsible for much of what happened.
Note: this is somewhat analogous to how Obama, the first African American president, presided over one of the most damaging and unjustified wars in Africa’s recent history, and when asked, stated it was “the worst mistake of his presidency” but nonetheless did nothing to fix the situation and was never held responsible for what happened (with Libya remaining a disaster over a decade since his invasion).

Here, the NYT tries to justify their complete failure here under the logic that the “most intense safety monitoring in US history” somehow could not detect injuries that were so obvious and apparent much of the general public was able to. Furthermore, all of these excuses are complete hogwash. For example:
•A safety monitoring system (V-Safe) was specifically made to be able to appropriately evaluate these events (which the government then covered up once, as court ordered disclosures showed, V-Safe proved the vaccines were dangerous).
• Many hospital systems have electronic medical records that track vaccination and health outcomes and are hence easily queryable databases. Remarkably, independent researchers are never allowed access to those databases, regardless of how much they try.
•The criteria VAERS had which was specifically made for detecting signals was met for 780 conditions—but somehow this also was not available to those officials.
•Some of the key symptoms linked to the vaccines (e.g., myocarditis) have been so extensively researched the general public knows to associate them with the vaccines—yet Federal officials somehow don’t know to look for them as well.
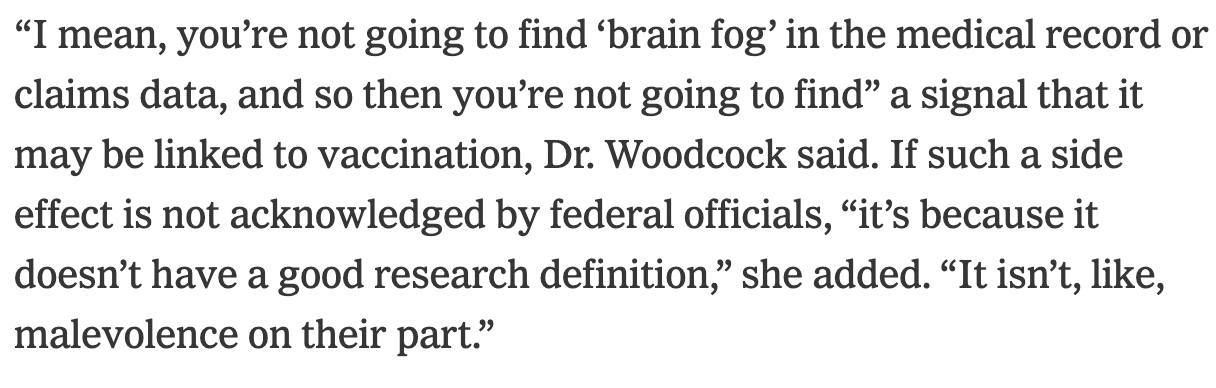
Note: Brain fog is one of the most common symptoms of a COVID vaccine injury.
The first excuse here is similar to the fact there is a massive backlog of reports being processed by VAERS (which the CDC is legally required to process) because the CDC has refused to hire anyone to process them.
The second excuse touches upon a similar problem with the normal vaccine injury compensation program (which covers everything besides the COVID vaccines). The court is quite fair in approving a “covered” injury, but since the Secretary of the HSS has the discretion to determine what a “covered injury” is and the “uncovered injuries” are almost impossible to get compensation for most—a lot of vaccine injuries never are allowed onto the list of eligible conditions.
The final excuse on the surface sounds “reasonable” to the right audience, but if you think about it for a moment, it directly admits the injured people are being sacrificed to protect the public image of the vaccines. Remarkably, I have read the exact same thing said countless times in the past (e.g., the 1967 text written by a prominent bacteriologist I previously covered repeatedly emphasized that the medical profession covered up vaccine injuries to avoid giving ammunition to the antivaxxers).


Note: as I show throughout this article, one of the most common scripts used to defend the vaccination program has been that the injuries are rare (e.g., one in a million). The best estimate I have seen of the vaccine injury rate is 18% of recipients experiencing mild to moderate injuries, 0.9% experience significant injuries (e.g., disabilities)—which of course does not include the many who have died (which many estimate at around 1 in 1000).
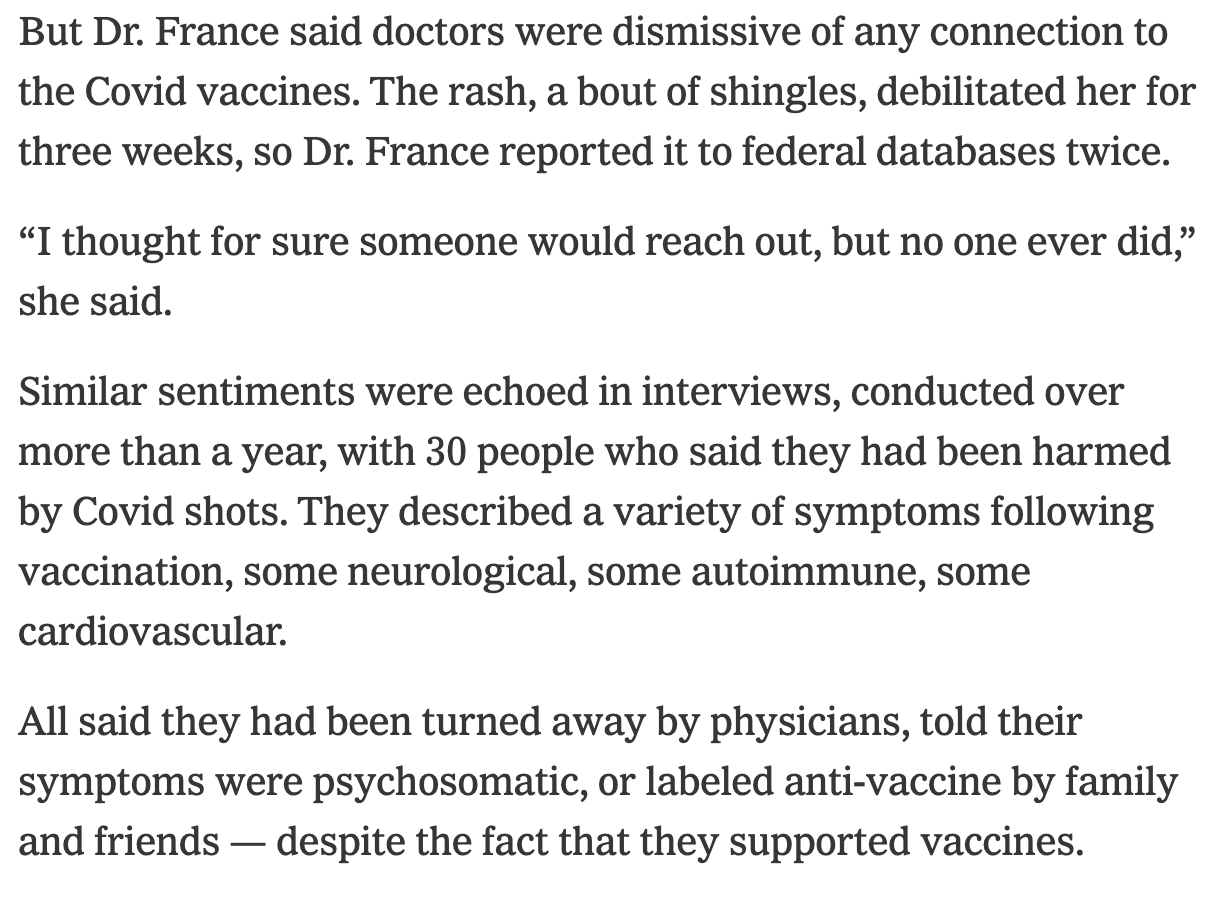
I have heard more examples than I can count of every single thing mentioned above, so I have to give the NYT credit for disclosing it. However, I believe that is also a reflection of how just common these issues actually are (and hence that the government is being forced to make some type of acknowledgment of them).
However, it’s quite extraordinary to me that they were only able to find 30 of these “rare” cases to interview over more than a year (as I could have found 30 people I knew who were vaccine injured and throughly interviewed all of them within a week). I am hence curious how this compares to your own experiences:
I also need to credit the NYT for mentioning this. However, it also touches upon one of the biggest mistakes with the COVID-19 vaccine rollout (which will be discussed later in this article).

This passage illustrates another common way vaccine injuries are gaslighted and neglects to mention that:
•Tinnitus and palpitations are two of the most common side effects of the COVID vaccine.
•Many of the symptoms of the vaccine and COVID overlap because both are caused by the spike protein (which the mRNA vaccine perpetually mass produces in your body and hence causes a more severe manifestation of).
Note: in the original trial for the Pfizer vaccine, Augusto, one of the participants nearly died from a complication to the vaccine. The trial site director (who was also the lead author of Pfizer’s pivotal NEJM vaccine paper) opted to document this as COVID despite Augusto having a negative COVID test.

This is a great example of a nice-sounding but meaningless statement, because no one ever does investigate them.
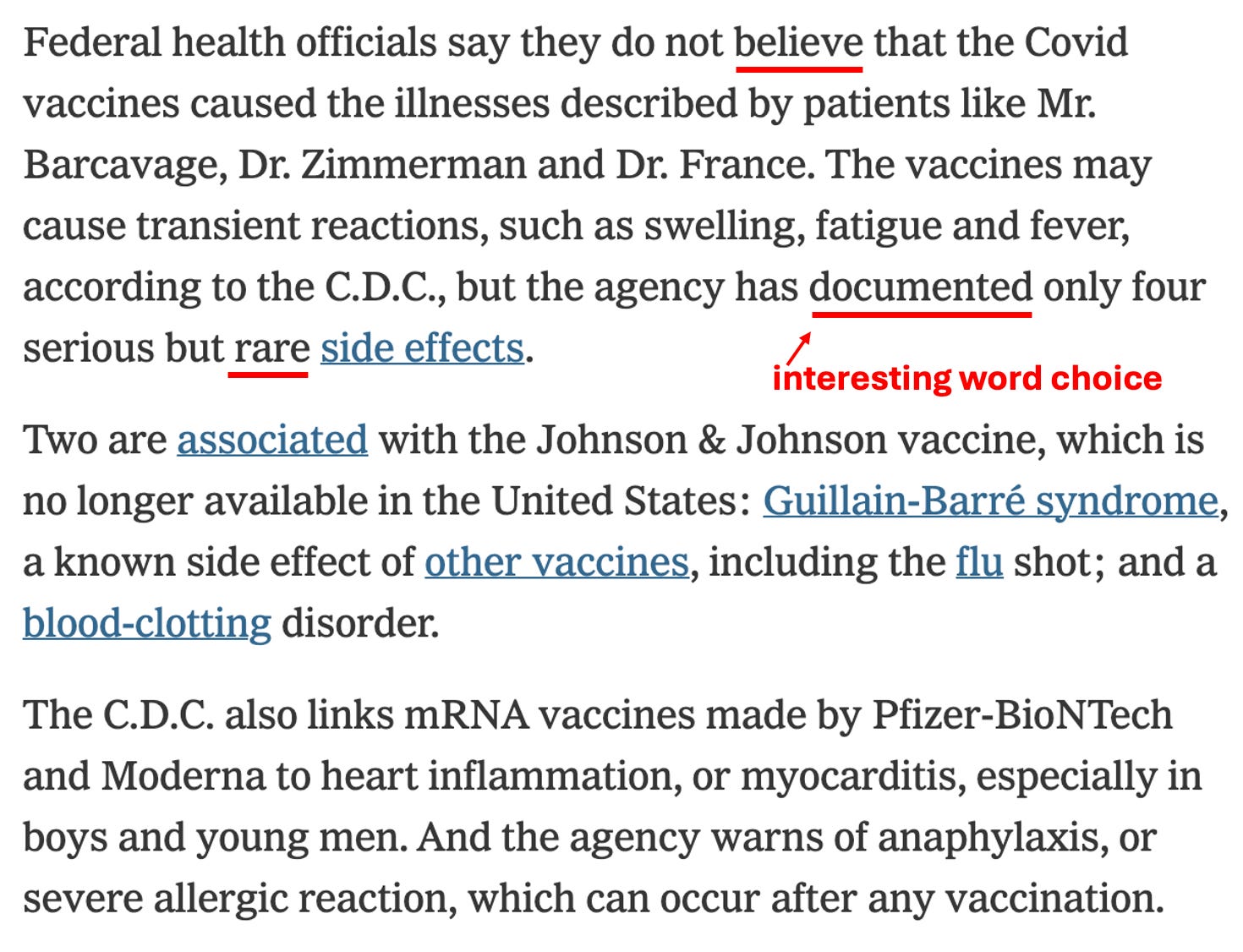
Here “believe” is used to suggest the lie but avoid committing to it. Similarly, “documented” has a very ambiguous meaning which again protects them from committing to a lie but implies they have no record of those injuries happening.
Additionally, it should be noted that the myocarditis link was only acknowledged because of a great deal of pressure on the FDA and CDC. Conversely, since the J&J vaccine has been taken off the market, there is more willingness to criticize it.As mentioned above, Steve Kirsch has conclusively demonstrated the CDC is not effectively monitoring VAERS for safety signals and is intentionally ignoring hundreds of them.
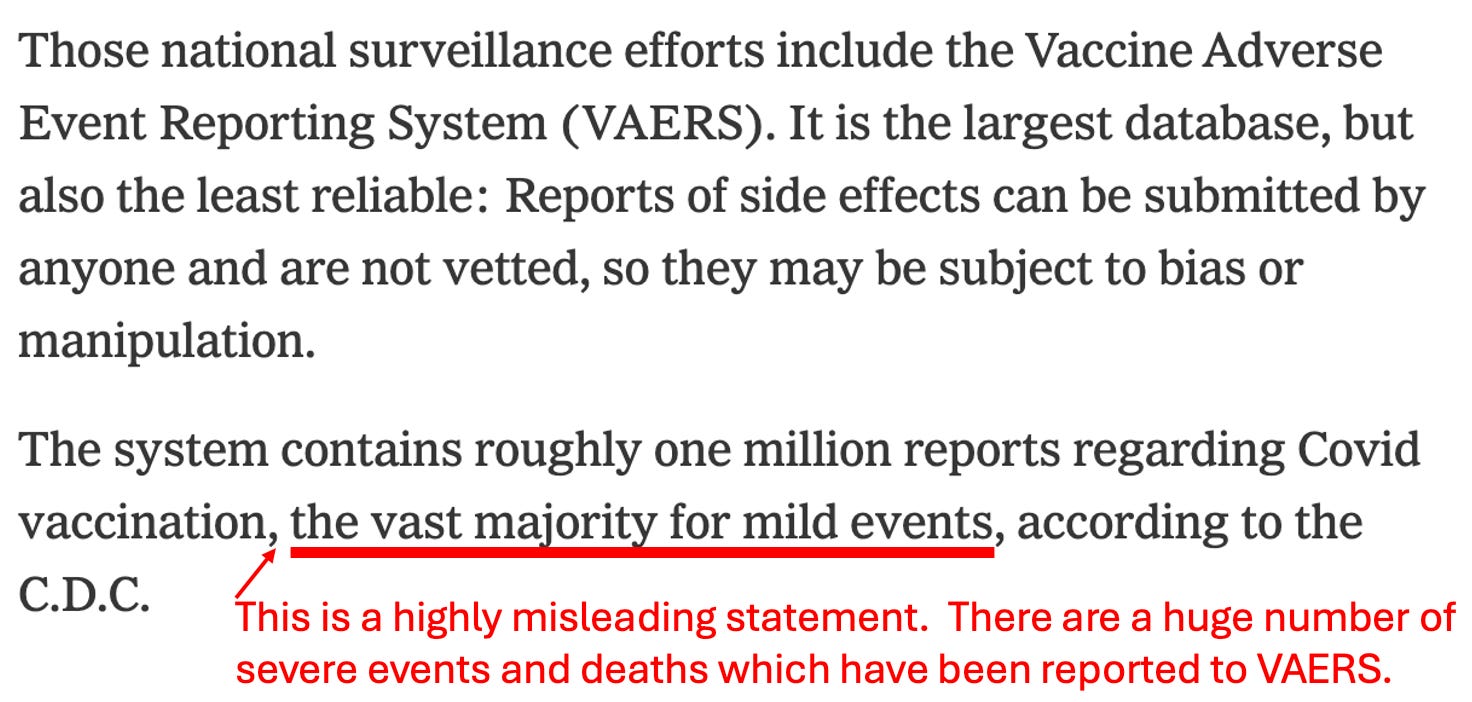
Something many people don’t know about VAERS is that it was specifically made because vaccine-injured parents found everyone refused to record the vaccine injuries they reported, and then used the lack of any reports to claim there was “no evidence the injury they experienced was real.” Once the government was forced to create it because of the 1986 Vaccine Injury Act, they have done everything they can to disparage it and understaff it so it cannot process most of the injuries it receives.
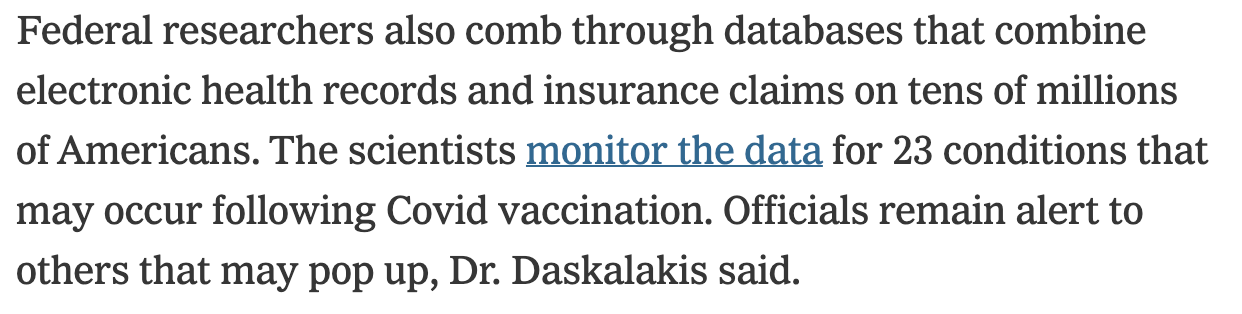
As I showed above, earlier in the article, the NYT claimed our Federal officials were unable to analyze vaccine injury claims because did not have access to databases like these.

It might be “harder,” but it’s still very easy to see them.

Saying the data is “unclear” is a very common strategy industry uses to bury inconvenient data.
Mark’s language is almost identical to that of the FDA’s former commissioner Dr. Woodcock. Remarkably, like her, Marks was also in frequent contact with those first injured by the COVID-19 vaccines.

It’s nice the NYT admitted this, but the focus should be on the fact officials actively sought out the data, not the data they already had access to (as the USA has willfully ignored theirs).

This is a misleading statement because almost all cases of shingles do not require hospitalization and the ones that do are really bad (e.g., that’s what killed Senator Dianne Feinstein). More importantly, it omits mentioning that if the rare cases are increased, there is a much larger increase in the common but extremely unpleasant cases (e.g., typical shingles).
Note: the link between COVID vaccination and shingles was discussed in more detail here.
This section strikes an interesting balance between acknowledging and denying tinnitus (one of the most commonly reported side effects of the vaccine). In addition to some missing data, the key point it neglects to mention is that all tinnitus is not the same (e.g., many cases are quite minor) whereas the COVID vaccine also produces severe side forms of it.
This passage again takes the tactic of greatly understating the magnitude of the problem.

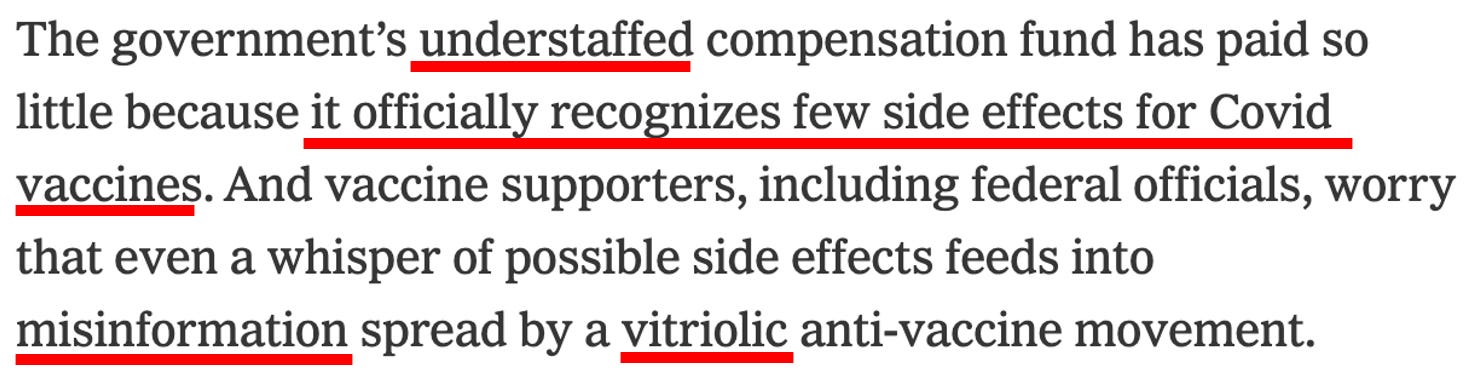
DARVO is an acronym for Deny, Attack, Reverse Victim, and Offender and encapsulates a common tactic abusers (and abusive institutions) use to control people. In this case, it is being argued that all of this is the “antivaxxer’s” fault because we are being mean to the honest scientists trying to share information about the safety issues with the vaccines but not making it safe for them to do so.

This raises a good point, but simultaneously neglects a much larger one. When a relative effect is small, you can only know for certain if it is real with detailed research. However, when the effect’s size is large, you don’t need sophisticated data to establish its existence. In the case of vaccines, the injuries are so frequent this type of research (which the government will never produce) is not needed to determine causality.
Note: the rest of the NYT article discusses the challenges individuals injured by the COVID vaccines face being compensated by the government’s program and attributes this to the COVID vaccines not having a tax on them like the normal vaccines to fund a compensation program. This is somewhat deceptive as it implies the normal compensation program works for individuals with vaccine injuries (it typically doesn’t) and that the primary issue is a lack of funding for the compensation program (whereas the actual issue is the legal immunity that makes it impossible to sue the vaccine manufacturers regardless of how egregious their conduct is).

The final line of the NYT article hints at a pivot many are expecting from the medical industry—once the vaccines can no longer be sold, the focus will shift to selling lucrative treatments for vaccine injuries.
Chris Cuomo
Brothers Chris and Andrew Cuomo (both children of a previous New York governor) previously were prominent members of the Democratic establishment, and due to their aggressive and belligerent personalities, became icons of the Left during the Trump presidency (e.g., NY governor Andrew Cuomo was frequently hailed as the leader of the resistance against Trump, while Chris attacked anyone who deviated from the COVID orthodoxy). I, in turn, have major disagreements with what both of them did during COVID as I believe it played a key role in the deaths of many Americans (e.g., by denying them access to safe and effective treatments for COVID-19). Likewise, New York had one the highest number of COVID-19 deaths in the United States, something which I believe was in part due to policies from the governor’s office.
After Biden became president, they were both discarded by the Democratic Party, with Andrew being pushed to resign from his position as governor and Chris having to leave his position at CNN because of the role he had played in helping to cover up Andrew’s sexual misconduct while governor.
Note: while I do not support Andrew’s alleged conduct (nor do I hold any positive feelings towards him), the point here is that this type of behavior is typically covered up (I have heard many stories of worse things being swept under the rug from people in the government), which in turn suggests that the Democratic party stopped protecting Andrew the moment the establishment no longer needed him.
Chris Cuomo in turn left CNN and was hired by a smaller mainstream news outlet (Newsnation) where he has become less partisan and begun to explore topics that would never be covered on CNN.
Recently, a great deal of attention was brought to the fact that Chris:
•Admitted that he was vaccine-injured.
•Hosted another vaccine-injured person on his show and discussed the struggles they both faced.
•Stated that he was taking ivermectin for his vaccine injury and that we had been lied to about it.
•Stated that he was given the wrong information about all of this from the authorities he assumed he could trust and that we need to know why this happened.
This provoked a very negative reaction because Chris (in his previous role) was one of the most vocal advocates against those who did not want to vaccinate:
In my eyes (keeping in mind that I do not know him nor anyone who does), Chris’s about-face is likely a product of him being discarded by the Democrat party, him being left on his own to struggle with his vaccine injury, and possibly, his network being open to covering the issue as they have a greater need for traffic than the larger networks like CNN. In turn, I believe that Chris’s willingness to admit what happened highlights the precarious position the medical establishment is in and that the best thing we can do at this point is to encourage people like Chris to come forward (as many of them are suffering in silence because they do not want to risk the political ostracism they will face from the left if they admit they were vaccine injured).
Note: I frequently hear people say that being a liberal and admitting you were vaccine injured is very similar to the reality gay men who wished to come out of the closet faced in the 1980s (due to social repercussions they faced for doing so). Stories like Cuomo’s I believe indicate that we are transitioning from coming out of the “vaccine closet” being dangerous to simply being risque and avant-garde but not actually a threat to one’s livelihood.
Cuomo has continued to push the envelope on this subject, and recently he had the former director of the CDC on air, who admitted Federal Officials silenced other government scientists who warned about the dangers of the COVID vaccines and thta “some” people were injured by them:
The Limits of Propaganda
I believe a few things were done with the COVID vaccines which has placed the medical system’s propaganda in a very challenging position. As I alluded to earlier, three are particularly pertinent now:
1. Propaganda can sweep “rare” side effects under the rug so most people ignore and forget about them (which happens a lot and is something I hence try to expose here). However, once too many people have those injuries, it can’t and this is the situation the medical industry is in now because the COVID vaccines had one of the highest injury rates of any pharmaceutical in history.
2. To market the vaccine, the most over-the-top propaganda campaign imaginable was utilized. The risk of this approach was that if it became widely known that the vaccine was fairly unsafe and ineffective, it would destroy the public’s trust in the medical system, especially since the widespread mandates and censorship were predicated upon the vaccine being “safe and effective.” This touches upon a broader point which is that one of the few things that can break the hold propaganda has over someone is if they are directly harmed by the lie (e.g., having to suffer from a vaccine injury will red-pill a lot of people).
3. To market the vaccine, healthcare workers (who are highly compliant with vaccination drives) were utilized to create the “social proof” that the public could trust the vaccines were safe and effective (as Americans are conditioned from a young age to always “trust their doctor”). While this initially worked (and many doctors zealously promoted the vaccines), as time went on more and more of them got injured. Typically, doctors (including well-intentioned doctors) are willing to gaslight patients who are injured by their drugs because one’s distance from the patient makes it very easy to buy into a rationalization that negates the validity of that injury. However, once the doctor is directly harmed by the medication, it becomes impossible for them to ignore what’s happening and they become able to see it in their patients. Because of this, more and more doctors are realizing exactly what happened and they are frequently discussing it behind closed doors, and more importantly, with their patients.
In turn, presently numerous polls show that roughly:
•Half of Americans believe the COVID vaccines are not safe.
•Half of Americans believe the vaccines are causing a significant number of “unexplained” deaths.
•A quarter of Americans believe someone they knew personally died from the vaccine.
•34% do not believe the vaccines are effective.
•7% experienced a severe side effect from the vaccine, and 34% experienced a minor side effect.
These numbers are extraordinary and dramatically higher than what I’ve seen stated for any other dangerous pharmaceutical (including the previous disasters where the American government rushed an unsafe vaccine to market and the mainstream media was willing to do its job and expose what happened).
As far as I can tell, there is no solution to this problem which would allow the medical industry to have its cake and eat it too as we are well past the point where a half-baked apology will “solve” the current predicament. Rather, I would argue that all the NYT article accomplishes is temporarily delaying the problem, as it will make many of the left-wing voters who were injured by the vaccine feel better because “someone cares about their suffering” but simultaneously, to do so, it further opens up the discussion our healthcare authorities do not anyone want to have.
Why Was This Done?
One of the most common questions we receive is “Why was this done?” This, in turn, is a very difficult question because most answers can’t explain why the medical industry would be willing to cause such profound damage to the public’s trust in them (which a lot of money has been spent over decades to create). Likewise, most of the potential answers to this question are impossible to prove, so if any of the leaders in this movement share them, it directly undermines their credibility as it shifts us from the realm of solid science to speculative conspiracies.
However, we are just as curious about this as you are, and in private, I’ve repeatedly heard this question be raised. Likewise, since I started this publication, I’ve had a variety of interesting people (e.g., a pharmaceutical executive from a major vaccine manufacturer) reach out to me to share their perspectives on what happened.
With that disclaimer in mind (that many of these are theories rather than facts), I will share the most compelling explanations I’ve come across for what happened over the last few years.
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.