

Constitutional Archetypes in Medicine
A discussion on the challenges of algorithmic vs. personalized medicine

One of the greatest challenges any large medical system faces is where to prioritize between personalized and collective medicine. For a large medical system to function, it needs to have standardized procedures everyone correctly follows—which takes a lot of work to facilitate throughout the medical system, but at the same time, no medical intervention is 100% appropriate for everyone, so any collective approach will inevitably fail to serve many of those who need care.
Although I very much follow the personalized approach in my own practice, I do not believe that either side of the equation is entirely correct. For example, there are a lot of challenging things standard medicine handles extremely well and we rarely think about because we take it for granted those things will dealt with correctly. In many cases, the primary reason they are handled so well is because a lot of work (e.g., years of trial and error) went into creating an effective approach and making it become the national standard. Likewise, there are numerous poor medical practices that persisted for decades and then gradually were reformed through the medical system recognizing those issues and then forcing every physician invested in the old (harmful) method to change what they were doing.
Conversely, because our system is structured to favor the collective, in order to make it be able to improve and reliably have everyone in it perform as expect, certain biases need to exist. They include:
•Everyone should strive to practice the “best” form of medicine.
•The best form of medicine is that validated by large randomized clinical trials.
•A physician’s personal judgement should be superseded by the existing clinical evidence.
•When conflicting clinical evidence exists, the evidence endorsed by trusted authorities is correct.
•If a patient cannot be helped with the existing approach, rather than the physician trying a new non-standard approach, the patient should be referred to a specialist (who is sadly often a psychiatrist).
•Protecting the medical system is important so if at all possible things that cast doubt on it (e.g., a pharmaceutical injury) should be dismissed.
As the last few years have shown the world, these biases can create a lot of problem. For example, because the system is so large (and hence has a great deal of inertia) it is very difficult to get anything to become standard of care unless a lot of money is spent to make that happen. This results in expensive and not necessarily effective therapies (e.g., remdesivir) disproportionately become the standard of care rather than effective low-cost ones no one can profit off of—especially once a lot of money is at stake and corruption inevitably enters the equation.
Although money and corruption are a huge issue, I believe the bigger problem is the widespread belief that following the “best available evidence” is the best form. Specifically, rigidly adhering to this belief becomes a huge issue if the best available evidence does not yield acceptable results for many patients.
For instance, sepsis is one of the most common causes of death for hospitalized patients, and for this reason, numerous policies and guidelines have been created which aim to improve a septic patient’s likelihood of survival. Nonetheless, hospitalized patients with sepsis still have a 24-35% chance of dying and one out of three hospital deaths occurs in a septic patient.
This is noteworthy because if IV vitamin C is given within their first 6 hours at the hospital (along with thiamine and hydrocortisone), the risk of death drops to almost zero. The ICU doctors I know who use IV vitamin C have all seen this difference and think it is unconscionable it is not the standard of care—especially since it is affordable and there are no dangers associated with it. Nonetheless, that’s the way things are because there is conflicting evidence existing for the merits of this approach and the trusted authorities support the evidence arguing against its usage.
Note: there are other approaches I believe could also dramatically reduce the mortality from sepsis (e.g., ultraviolet blood irradiation). I am focusing on IV vitamin C here because there is by far the most evidence for that approach.
I have watched the IV vitamin C debate play out numerous times (e.g., when it is requested for septic hospitalized patients) and I am always struck by the fact doctors are unwilling to consider trying it out (because there is not evidence for it) even though they know the patient is otherwise likely to die. This in turn was why I was less than shocked when during COVID-19, doctors around the United States were unwilling to try anything not within the COVID treatment guidelines for patients they knew would otherwise die.
To illustrate, as detailed in The War on Ivermectin, there were 80 lawsuits where families with a relative being subjected to the COVID hospital protocols, and was expected to die, had lawyer Ralph Lorigo sue the hospital for ivermectin to be administered to their relative. Of those 80 lawsuits, in 40 the judge sided with the family, and in 40 with the hospital. Of the 40 cases where ivermectin was given, 38 of the 40 patients survived. Of the 40 cases where the hospitals were allowed to withhold ivermectin, 2 of the 40 patients survived.
In turn, I regularly see blatant examples of this behavior. For example consider this response by an ICU doctor to a recent article I wrote that Pierre Kory shared on Twitter:
The problem with this doctor’s logic is that:
1. The current treatment of burns still leaves much to ask for as the time spent in the burn unit is a prolonged and agonizing process for the burn victim and frequently they are left with permanent disfigurations that impair their quality of life.
2. Numerous approaches have been developed over the years which frequently were able to rescue the damaged tissue, significantly improved survival of burn victims (which is less of an issue now since that has instead been solved through improved supportive care), shortened their time to recovery and significantly decreased their pain (independent of pain killers).
3. He is not aware of any of that research because it is not in the guidelines—which I would argue is not a valid excuse.
These types of doctors are typically very good at treating life-threatening conditions medicine has already solved (e.g., diabetic ketoacidosis). Yet they struggle with conditions where the existing guidelines do not provide a reliable solution and in those circumstances, will never consider non-standard approaches such as ivermectin for COVID (which is why the previously described lawsuits were necessary).
As a result, over the years (but especially during COVID) I’ve heard of numerous cases where a patient was expected to die and someone went behind the hospital’s back to covertly administer a therapy which then saved the patient’s life. Even though hospital doctors essentially have the legal cover to do this thanks to Trump’s 2018 Right To Try Act, at this point in time, I only know of one hospital in the United States where the physicians are willing to try non-standard therapies for patients they know need them. From a patient perspective this is appalling, but from the perspective of a system seeking to promote the universal adoption of standardized treatment protocols (which it aims to ensure are correctly administered), it is to some extent necessary.
Note: after I posted this article, one reader (a lawyer and doctor) shared a comment I believe adds an important context to this section.

Large Double Blind Trials
At this point in time, we hold the belief that for a clinical trial to be valid, it must have a large number of people enrolled in it, and be double blinded. I would argue the following is true about those trials:

Note: my own belief is that large magnitudes of effect do not require large trials to be detected (which has been repeatedly shown by small studies observing those effects that are eventually confirmed by large blinded trials and then become the standard of care). Since a therapy at least in theory should have a large magnitude of effect, this calls into question the assumed need for prohibitively expense trials in order to adopt a new therapy.
The above also helps to explain why a ton of money is frequently spent on those trials, yet they often fail to detect clinically significant adverse events (e.g., consider the countless severe injuries that whistleblowers from the COVID-19 vaccine trials revealed were covered up by the vaccine manufacturers). Likewise, financial conflicts of interest help to explain why more and more pharmaceuticals are pushed onto patients despite them not appearing to provide any significant benefit to the majority of those receiving them.
The corruption within the trials is easier to understand (and entirely predictable since their cost virtually guarantees the sponsor will want a positive outcome which protects their investment). However, I believe the fact that they are a weighted average that sees each patient through a collectivist lens rather than as an individual is ultimately much more harmful. The collectivist lens makes it possible to ensure the overall greatest benefit (e.g., by having the therapy with a 30% success rate rather than the 25% success rate be the standard of care), but it fails to do anything for those who do not benefit from it (which often comprises the majority of patients).
Unfortunately, there is rarely one correct therapy for every patient. For instance, although there are certain things that are more likely to be helpful for COVID vaccine injuries (e.g., improving zeta potential or a systemic regenerative therapy), when working with a vaccine injured patient, I frequently need to use a different approach from what I’ve done before to improve their symptoms). This reality is fundamentally incompatible with a standardized model which provides the “best” treatment algorithm for every patient.
One of the most important challenges with evidence based medicine hence becomes “how do I know if the results of this trials are applicable to the patient in front of me?” Unfortunately, while some leaders in the field recognize this issue, the majority of physicians in practice do not seriously consider it.
An excellent example is how to dose pharmaceuticals. Many of my colleagues who get the best results with drugs typically use nonstandard doses (normally lower ones) they calibrate to each patient. Because they do this, they are able to get many of the benefits of the drug without much of the side effects. However, the majority of doctors use the standard dose pharmacies provide the medication in (reflexively assuming it must be correct), thereby failing to recognize that the dose is a weighted average rather than specific to what each person needs. Furthermore, in many cases, those doses are chosen for the sake of making profit rather than serving patients.
For example, as detailed in the memoir of a Pfizer sales rep, when viagra came out, the FDA approved three doses of the medication:
•25mg—for the elderly (the most likely to use the drug) and those with kidney problems.
•50mg—the normal starting dose
•100mg—for people who did not respond to the starting dose
Since Viagra was a new medication, Pfizer was worried too many early overdoses (something their trials had detected was a real risk from the drug) would spoil the market. So, to preempt this, Pfizer broke with the standard industry practice of charging more for a higher dose and made the price for a 50mg tablet and 100mg tablet be the same so that their sales representatives, seeking to meet their monthly quota, would not try to push the higher dose to doctors and cause too many overdoses from the 100mg formulation.
However, this “backfired” as patients quickly realized they could buy the 100mg pill and then cut it in half to save money. Pfizer panicked (as they assumed their initial design made the pill uncuttable) and instructed their reps to instead tell physicians the 100mg dose was optimal. Later, after better solutions were found to prevent patients getting two Viagras for the price of one, Pfizer again reverted to promoting the 50mg dose.
Conventional Archtypes
Numerous factors are recognized to affect how drugs will interact with the body. These include:
•Age—as you become older, your body becomes less able to tolerate toxic pharmaceuticals. For example, the kidneys and liver are responsible for clearing drugs from your body, and since their function declines with age, the elderly often cannot tolerate the same dose of a drug that a younger person can. Likewise, as you age, your arteries become less able to reflexively bring blood to your head when the blood pressure drops there, and as a result, if we medicate the elderly down to a blood pressure younger adults can easily tolerate, it far too frequently results in them becoming light headed and passing out (which is a huge problem because of the severe harm falls often cause to the elderly).
Conversely, premature infants are less able to tolerate vaccinations than normal weight infants, and as a result, neurological disorders and sudden infant death syndrome following vaccination is much more common in those children. Nonetheless, because vaccines are assumed to be a 100% safe and effective, ways to prevent toxic doses (e.g., by vaccinating later in life or spacing out vaccinations) are never considered within the conventional medical system.
•Gender and Race. Significant differences exist in how different ages and genders respond to many medications. Unfortunately, in the same way that drugs frequently given to the elderly are rarely tested on older patients in clinical trials (since to make a drug look “safe” it has to be tested on those least likely to be injured by it—which is typically young healthy adults) it is rare drug trials will assess for gender specific responses to a drug and rarer still that racial differences will be evaluated. Furthermore, in the name of DEI, there has recently been a push in the medical field to remove many of the metabolic differences that had been observed between different races (and affected their appropriate medical management).
Note: one reason many suspected SARS-CoV-2 was a race-specific bioweapon is because a lot of research has been done on racial differences in the ACE2 receptor (since many common pharmaceutical drugs target it) and because it was observed that the spike protein’s ACE2 affinity significantly varied by race—something which in theory was possible to design ahead of time due to the preexisting ACE2 research.
In addition to demographic factors (e.g., age, race, sex) affecting one’s response to a pharmaceutical, genetic variations can as well. For example, the P450 enzymes play a pivotal role in liver detoxification, and as a result, P450 function directly affects how long a drug will stay in the system and what the resulting appropriate dosage is for it. On one hand this is considered in medicine since certain drugs are known to increase or decrease (more common) P450 function, although typically, the main reason we hear about this is because grapefruit juice also does that (to a moderate degree), so patients are often told not to drink it in conjunction with a variety of medications.
Note: during my training while at a rotation in a hospital where I didn’t know anyone or have access to a kitchen, I decided to go on an all fruit diet for a month instead of eating from their cafeteria. Since I ate grapefruits I brought with me each day at lunchtime, I received a lot of concerned comments from physicians and medical residents about how doing that could be dangerous—something I never heard them say about any the pharmaceuticals so many people there were on.
More importantly, significant genetic variations exist in P450 function that are virtually never considered. One of the more tragic examples can be seen with SSRI antidepressants. A long standing problem with those drugs is that a certain portion of people who take them become violently psychotic and then either kill themselves or others (e.g., in a school shooting). Many of the stories are quite horrifying and subsequent lawsuits those killings inspired showed these side effects were observed throughout the clinical trials and then covered up.
Forensic investigations in turn have been conducted to determine what caused the individuals to turn psychotic. One common thread was the individual having a genetically reduced P450 function, which in turn caused the individual to develop dangerously high levels of the SSRI in their bloodstream. For example, in one study evaluating 10 patients suspected to have this issue (due to them becoming violent after starting an SSRI), all ten were found to have a genetically altered P450 function, and all ten become normal once their SSRI was terminated.
This is important because very few physicians who prescribe SSRIs are even aware of the P450 issue, so it is something never screened for when the SSRIs are prescribed. Likewise once an individual starts developing early psychotic symptoms, it is rare for the physician to attribute that to the drug (rather they often assume it arises from insufficient dosing and hence give the patient more of the SSRI).
Similarly, because no one wants to acknowledge that vaccines could cause autism, a lot of research has been conducted to find the genetic cause of autism (which is nonsensical because a gene can’t suddenly appear in a massive number of people—something that would be necessary for a genetic cause to explain the sudden explosion of autism).
As a result, despite all the desperate searching, no “autism gene” has been found. However, a large number of genes have been linked to autism and many of them either reduce detoxification of the body or increase the sensitivity of the body to developing an abnormal metabolic state in response to a stressor (e.g., a hyper-inflammatory one). Likewise, consider the story of the McDowell triplets, all of whom suddenly became autistic on the same day with a few hours of their vaccination. To anyone looking at the situation objectively, all of this research suggests some children are more susceptible to vaccine injuries than others and hence should be dosed differently—but instead this is never even a consideration within the standardized medical system.
Integrative Archetypes
Within the integrative field (partly due to the fact a higher level of service needs to be provided in order for patients to be willing to directly pay for medical care), there is a greater recognition that genetic predispositions require differing approaches for treating a patient. As a result, many different protocols have been developed such as genetic testing or blood work being done to identify the presence of disruptive SNPs which are then treated with a supplement regimen that mitigates the metabolic defect created by the SNP, and some patients benefit greatly from this approach (discussed further in this book).
One of my favorite examples of functional medicine’s personalized model of care came from William Walsh, PhD. Walsh spent 20 years building a database of 2,800 depressed individuals (which had over 300,000 analyses of blood and urine) and identified five common patterns that were seen. Most of those patterns in turn were the result of genetic predispositions (e.g., deficient or excessive methylation) that could be detected with relatively affordable tests and if treated directly (e.g., by giving methylation supporting supplements) would resolve the patient’s depression.
Furthermore, some of these metabolic types would improve if SSRI antidepressants were given to the patient, some would experience no improvement from an SSRI, and some (the overmethylators) would instead begin to turn psychotic if administered SSRIs. Sadly, while depression is one of the most common reasons why patients see a doctor, very few doctors (including psychiatrists) are even aware of this concept—which again highlights the medcine’s inability to recognize what individuals (rather than the collective) need.
Most importantly however, people in the integrative field tend to notice many of their patients are “sensitive” patients who do not respond well to traditional medical care.
Traditional Archetypes
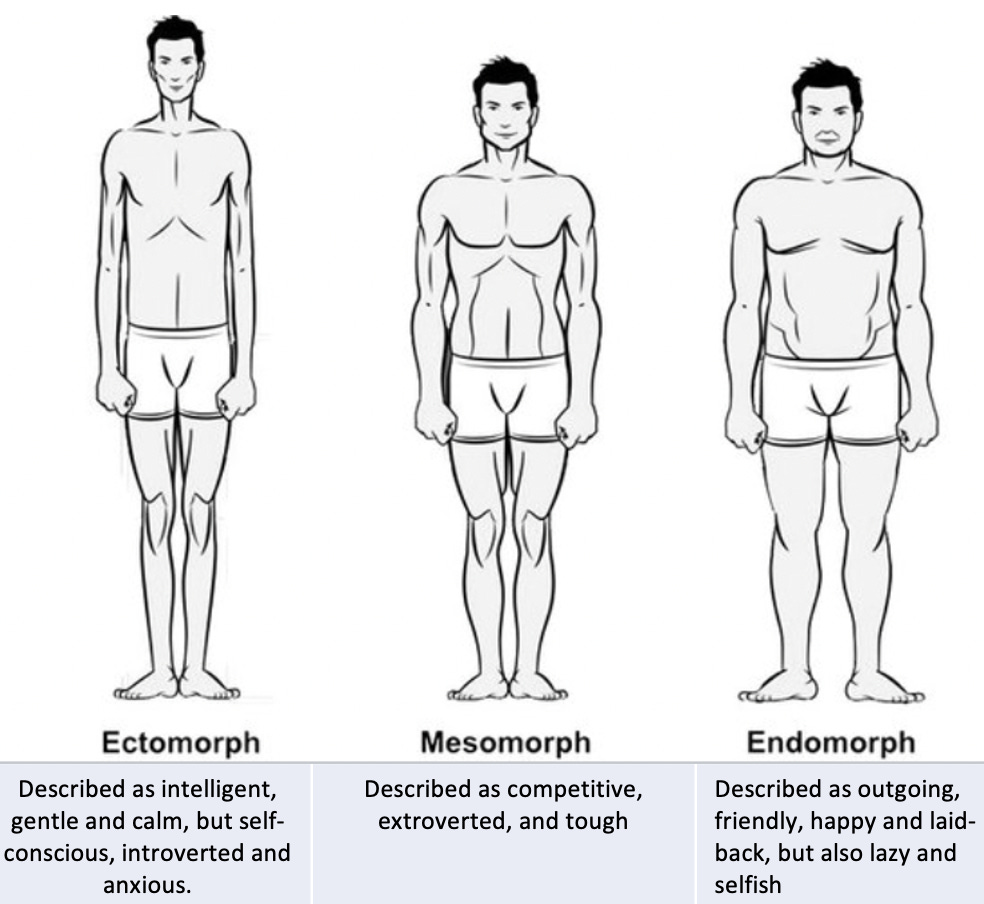
Within the modern system, I only know of one periodically utilized method for classifying individuals to a specific archetype, the somatotype theory. It is based off attempting to pair personality traits with specific body shapes which were then classified by linking them to the three germ layers the human embryo develops from.
Note: what I find most intriguing about this theory is that I have observed a few instances of individuals having the body type and personality of one somatoform and then later change to the body type and personality of another somatoform.
In contrast to the modern standardized medical system, most traditional medical systems believe that much of human health is defined by their constitutional archetype. In general, the belief was that some type of constitutional “energy” imbued the person and guided the development of their body mind and spirit. As a result, their training always focuses on learning to identify these archetypes and then using a different approach for each patient depending upon what their archetype is.
Over the years, I’ve looked at more of these systems than I can count, and I’ve felt they have many overlaps and varying degrees of validity. For instance, astrology is probably the archetypal system the greatest number of you are familiar with and it has long bothered me how accurately my three astrological signs (sun, moon, and rising) define my personality, as that uncanny accuracy argues to some extent against my own free will. Likewise, while I am by no means perfect, I can now guess an individual’s astrological sign far more frequently than would be attributed to chance (1 out of 12 times). At this point, I am still unsure over how I feel about astrology, but I’ve always found it compelling since (as highlighted by Graham Hancock) many ancient societies had a remarkable strong emphasis on understanding the exact movements of the constellations.
Note: one of the lesser known facts about astrology is that there is also a system many swear by (provided there is one day of wiggle room) which assigns a specific personality to each day of the year.
Of all the archetypal systems out there, there are two I find to be particularly useful.
The Three Gunas
Hinduism is one world’s oldest religions and is practiced throughout India. As a result, much of India’s cultural heritage, such as the Ayurvedic medical system originated from Hinduism. Typically, when constitutions are looked at through the Ayurveda’s lens, individuals are constitutionally classified as belonging to either the Vatta, Pitta or Kapha dosha. A variety of Ayurvedic treatments in turn exist for each dosha and are directed at either providing things which support each person’s dosha, or address an imbalance between the doshas.
While the doshas are fairly well known (due to the spread of Ayurveda into Western culture) another system also exists which is much less known here. Guna when translated means something akin to a “quality, peculiarity, attribute, or property.” Three Gunas are recognized to exist, and it is thought in Hinduism that they have always been and continue to be present in all things and beings in the world—although their proportion varies in each place. In turn, the proportion of and interplay between these Gunas defines the character and nature of whatever they imbue.
The three Gunas are:
Sattva, which has qualities including “goodness, calmness, harmonious.”
Rajas, which has qualities including “passion, activity, and movement.”
Tamas, which has many qualities including “ignorance, inertia, laziness.”
Sattva in many ways mirrors Vatta, and to a lesser extent the ectomorph type. Rajas in turn pairs with Pitta and mesomorphs while Tamas pairs with Kapha and endomorphs.
The reason I place a heavy emphasis on the three Gunas is because patients will typically have one of the three Gunas predominate them, and the appropriate way to care for them is completely different from someone embodying another Guna.
Sattvic patients tend to have a more ephemeral (less solid) body type and personality and are much more sensitive to their environment and surroundings. Tamasic patients are the opposite, and tend to have a much denser and thick body body type and are much less sensitive to the things around hem. Rajasics in turn are the most active of the three and lie in the middle of the spectrum between Sattva and Tamas.
Note: In a recent article, I discussed the curious phenomenon of memories, skills, emotional patterns and preferences transferring from an organ donor to the recipient—something most commonly observed with heart transplants. One observation made by the researcher who collected numerous highly compelling reports of this occurring was that only a minority of transplant recipients experienced this personality transference, but within that minority, eighteen traits were commonly observed. Interestingly, most of those traits (e.g., an ectomorph body type) were identical to those I typically associate with Sattvic individuals.
This system is important because Sattvic patients tend to be immensely responsive to gentle therapies (e.g., energetic therapies like acupuncture) and react badly to harsh forceful interventions (e.g., having their joints popped, receiving pharmaceuticals or having surgeries). Tamas types are the exact opposite and respond well to forceful interventions while gentle and more natural or energetic ones typically do nothing for them.
There are many consequences of this theory and I would argue the most important one is that it helps guide which type of therapy to use and know ahead of time who will be the most likely to be harmed by it. Throughout my life, I have known Sattvic patients who have been severely injured (and often permanently disabled) by the medical system. I have always felt this is an immense shame because the sensitivity of the Sattvics often makes them able to perceive what is wrong in the world around them and be driven to fix it, but instead of being able to do anything they are simply trapped by their illness and unable to do any of that critically important work.
In turn, many of the ideas I’ve put forward are strongly influenced by the Sattvics. For example consider the cell danger response (CDR), which I believe is one of the key issues that defines both long-covid and spike protein vaccine injuries (and frequently must be treated to resolve the injury). It was originally developed to answer a simple question—why are some patients (particularly those who eventually seek out integrative medicine practitioners) so sensitive?
For context, these patients have many different hypersensitivities like mast cell degranulation disorder (something also frequently seen following COVID vaccine injuries). Likewise, it is often quite difficult to treat these patients as a tiny amount of a relatively safe therapy would often trigger a systemic decompensation that took them weeks to recover from—something many physicians treating spike protein injured have likewise encountered.
Note: there has also been a longstanding observation within the integrative medical field that hypermobile patients are much more “sensitive” and likely to be injured by pharmaceuticals (e.g., the HPV vaccine). I have noticed those patients tend to have a Sattvic constitution.
I find that outside of the integrative field, Sattvics are relatively misunderstood by the medical field, and as a result, their sensitivities are often interpreted to be psychiatric in nature. Further compounding the issue, since there are also many Tamasic patients (who respond quite well to conventional care), mainstream doctors tend to disproportionately remember those positive responses and assume they generalize to their entire patient population.
So when the opposite of what the physician intends ultimately happens from their treatment plan, they tend to view it as being fault of the patient rather than consider that they might be working with a different constitutional archetype which intrinsically requires a different treatment approach. Likewise, I tend to notice that healers (both doctors and non-doctors) tend to gradually accumulate a practice matching the Guna the physician is unconsciously biased towards treating.
The Five Elements
Many different societies have concluded that primordial energies matching the metaphorical elements give birth to physical matter and that if the elements which compose something can be identified, many of its traits can be predicted from that elemental composition. Typically, four element or five element systems were adopted—with the (less common) five element systems adding in an extra element to account for mind being one of fundamental qualities which allows manifestation.
The four elements are typically water, fire, earth and air. In astrology for example, of the twelve signs (one being for each month), three are assigned to each element.
The most well known five element system comes from China’s culture and is used throughout Chinese medicine. Within this system, many different things (e.g., organs of the body) are assigned to each system and many treatment approaches exist which like those for the doshas, essentially seek to either provide therapies specific to the patient’s constitutional archetype or identify and resolve imbalances between those archetypes (the elements) within a patient.
Having reviewed numerous archetypal systems, I believe that overall, the Chinese five elements is the most accurate one I’ve come across. In turn I can often discern which elements predominate an individual I meet and I find frequently find the system to be immensely useful.

Note: although the above diagram of the generating and controlling cycle is typically used to describe how the five elements affect the physiology of the body (for instance I discussed some important but relatively unknown examples of it in this article), I have found it to also be extremely useful for understanding many other things like human relationships.
Archetypes and Human Interaction
The entire five element theory is quite detailed, and since it has been extensively written about by the Chinese Medicine field and is relatively easy to find online, I would instead like to focus on a few of its non-medical correlates. For example, many gifted healers and teachers I have encountered predominantly utilize one of the five elements (the one matching their innate constitution) to practice their craft and have unique styles which embody the characteristics of their element. I share this because a great deal of what I’ve learned in life came from observing those individuals and trying to recreate the subtle qualities they brought forward in my own work.
Frequently, in life, we encounter things that hold profound importance to each human being yet lie outside the existing bounds of science (e.g., the dying process) and thus remain a constant source of both fascination and frustration. One area I feel this is particularly true in are human interactions and human relationships.
Over the years, I have come to believe that any pair of individuals have an intrinsic degree of compatibility, and that this intrinsic compatibility rather than any preconceived notions is the primary determinant of how their short-term or long-term interaction will proceed. Since that intrinsic compatibility is largely a product of the constitutional archetypes (e.g., the “energies”) which compose each individual, it becomes extremely difficult to accurately model the interaction by solely describing it through an intellectual lens like psychology.
Unfortunately, that is exactly what our society has always done (e.g., its fascinating to see how the social constructs of beauty have changes over the decades and centuries), and since the algorithms of Big Tech entered the picture, the process has only accelerated. For example, patients regularly share their regrettable experiences with online dating, and the consistent pattern I’ve noticed is that almost all of the qualities which the online platforms select for are mental ideas that have almost no correlation with the essence of who someone is of if there will be any intrinsic compatibility between two individuals.
Note: to date, the most reliable (but by no means perfect) quality I have come across that can be conveyed online and accurately determines overall compatibility between two individuals is both of them being unvaccinated.
Likewise, I believe that much in the same way personality transplants can occur following organ transplants (which suggests that aspects of our consciousness do not originate in the brain) I believe much of our personality and preferences (e.g., what type of people we seek out) directly originate from the energetic archetypes we are composed of.
In the final part of this article I will discuss some of the specific patterns I have observed regarding how those archetypes influence human interactions and how I believe they go a long way towards answering some of the longstanding questions in this realm (e.g., with human relationships). Since this can be a touchy subject for some but is also something I feel is very helpful for many (e.g., as I see many people have tumultuous personal lives as a result of them forcing relationships to happen when the archetypal compatibility simply is not there), I went back and forth on covering it at all and decided its best to share with a smaller audience.
Keep reading with a 7-day free trial
Subscribe to The Forgotten Side of Medicine to keep reading this post and get 7 days of free access to the full post archives.