

Another COVID-19 "Conspiracy Theory" Comes True!
Yearly ineffective and unsafe COVID-19 vaccines epitomize the pharmaceutical business model.

By this point, most of you have probably heard the news:

Note: The full information for the public meeting tomorrow which is scheduled to evaluate this proposal (1/26/2023) can be found here.
Given that existing evidence now shows that:
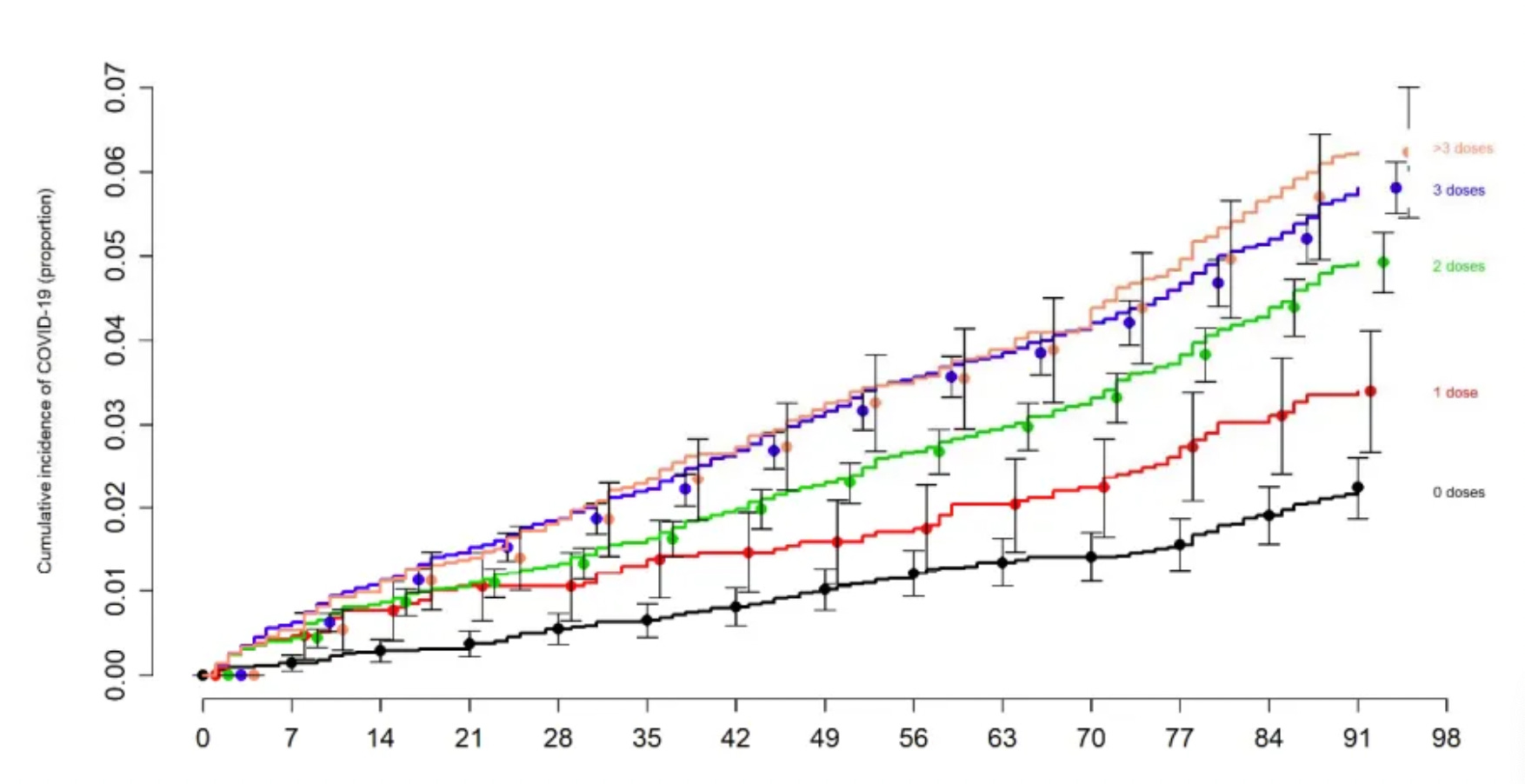
•More COVID-19 vaccines over time result in reduced immunity to COVID-19 for the individual (best shown below by the Cleveland Clinic’s study of 51011 people):
•Severe injuries are very common following a COVID-19 vaccination and increase in frequency with each successive vaccination.
•A large portion of the public essentially agrees with the previous statements and most importantly believes that the vaccines are killing people.
It is completely inexcusable that the FDA has moved towards instituting annual COVID-19 vaccinations (which, following their authorization, will be made mandatory by many institutions and employers). When a similarly unjustifiable decision happened last year after the CDC decided to add the COVID-19 vaccines to childhood immunization schedules, I wrote a lengthy piece on the systemic (and documented) corruption within the agency.
Since the reprehensible corruption within the federal agencies which are overseeing the vaccines has already been a frequent topic of discussion here, I felt that a different lens would be more appropriate for considering today’s events—what is financing that corruption? Many of the concepts in this article build upon the ideas put forward in this previous article:
Recently Project Veritas got a bombshell interview where an alleged chief scientific officer actually admitted Pfizer is conducting gain of function research on COVID-19 to aid in their development of vaccines for future variants. This is clearly outrageous so this video will likely be seen by many.
However, there is another important point also raised by this video as the Pfizer scientist discusses both the systemic corruption within the revolving doors of the healthcare system and describes the business model Pfizer is following for COVID-19. These provide important context for the arguments that will be laid out in this article.
The Vaccine Playbook
As I observed the pandemic unfold, I correctly predicted that we would go through the following stages:
1) Every authority would deny that COVID-19 was a problem until it had hit a critical mass and could no longer be stopped (note: I am still not sure if this deceit was motivated by a desire to spread the pandemic or done to stockpile the resources necessary to combat it as Event 201, the exercise that “simulated” the pandemic a month before it started, advocated for doing the latter, but I only observed the former transpire).
2) Once that critical point was reached, the media would reverse course and attempt to create the largest possible hysteria about COVID-19.
3) A few ineffective (but proprietary) drugs to treat it would be put on the market, while at the same time, numerous effective (but not proprietary) treatments for it would be banned.
4) The inability to treat the disease would be used to justify a variety of (ineffective) mitigating measures that would create a massive disruption to everyone’s lives and businesses.
5) This contrived “emergency” (e.g., the lockdowns) would be used to open up the mRNA market since mRNA gene therapies represented a trillion-dollar market for the pharmaceutical industry (which is now desperate for new proprietary drugs).
6) Because there have been major issues with mRNA technology that had prevented its use on humans, the emergency would be used to override that obstacle. This, in turn, meant that the companies would be allowed to cut a lot of corners on testing vaccine safety before administering them to test subjects and then the general population.
7) An extremely aggressive marketing campaign would be used to promote the vaccines to the public (it ended up being arguably the most over-the-top propaganda campaign in history), and the vaccine roll-out would be structured in a sequential way to maximize sales (which also required aggressive censorship of anyone or anything questioning vaccine safety).
The essential formula would be:
•Pressure as many people as possible to vaccinate with one sales push.
•Wait for that market to saturate.
•Once it had, do a more extreme sales push that used the previous vaccine uptake to justify it being done.
•Repeat ad-infinitum, until annual COVID-19 vaccines become normalized (note: even here I was too näive as the FDA is suggesting biannual vaccines for “high-risk” groups like children, the elderly, and the immune-compromised [keep in mind that these vaccines commonly create immune suppressions]).
If we look at the roll-out itself, it essentially followed the predicted pattern.
•First, everything possible was done to market the vaccines as a modern-day miracle.
•Second, a scarcity model was used to sell the vaccines so that people would jump on getting them at the first opportunity (people always want what they can’t have).
•Third, the initial cohort that got them were healthcare workers because it was known that they would be the most likely to comply with experimental vaccination (as they had already been trained to comply with their annual required flu shots), and their recommendations would garner the most trust in the public. The elderly (who were vaccinated next) fulfilled a similar role because a rationale could be made to vaccinate them before younger adults were “eligible” and if they were injured or died, it would be easy to sweep what happened under the rug (e.g., consider what happened in the nursing homes and how many vaccine deaths were simply attributed to old age).
•Fourth, once the initial irrational exuberance behind the vaccines ran out (e.g., due to the vaccine injuries and failures of the vaccines to prevent COVID-19), and people stopped wanting to vaccinate, an incentive model would be introduced where people were bribed to vaccinate. I tried to list some of the examples here. The bribes included direct payments, lotteries, all sorts of junk food, marijuana, alcohol, and even prostitutes.
•Fifth, once the bribes stopped working, soft mandates would be instituted. These essentially said if you want your freedom back (e.g., to travel or to go to restaurants and concerts), you had to vaccinate.
•Sixth, once the soft mandates stopped working, hard mandates would be instituted. These would be initially tried upon vulnerable populations (e.g., the military or nursing homes residents) who could not refuse the order, and then leveraged against groups that the government had some degree of control over (e.g., federal employees or anyone working for a facility receiving Medicare payments—which applies to most healthcare workers). Finally, corporate America would be gently encouraged to mandate vaccines for the entire workforce, and then firmly made to do so through (illegal) government mandates.
•Seventh, once the hard mandates also hit the saturation point for vaccine sales, the most questionable market--children who have no risk of dying from COVID-19--would be opened up and built upon the existing sales apparatus that had been created for pressuring vaccines onto children.
•Eighth, once all existing markets for the COVID-19 vaccines had been saturated, everyone would pivot to selling boosters so that the previously established market could be reused. I suspect that this was planned for from the start, as the mRNA spike protein vaccine platform (consisting of a single antigen in a rapidly mutating portion of the virus) was virtually guaranteed to rapidly trigger the evolution of COVID-19 variants that the vaccine no longer worked on.
•Ninth, as those boosters failed (due to them not addressing the underlying problems with the vaccine-promoting mutations), more boosters would be pushed on the population.
•Finally, once the population had become accustomed to an endless barrage of COVID-19 vaccines marketed on false premises, this would pivot to annual COVID-19 vaccines, which like annual influenza vaccines, do not work, but are just taken on faith to work. Simultaneously, the “incredible success” of the mRNA vaccines would be used to declare that the (extremely dangerous) mRNA technology is safe and does not require significant scrutiny before being used in other products (e.g. the recent bivalent booster that was only tested on 8 mice before being approved for humans).
Being aware of this process was also why I encouraged everyone I spoke to who was conflicted about vaccinating to do whatever they could to avoid vaccinating and to NOT do so by forging a vaccination record (which was an easy option for many in the healthcare field). I felt that since escalating the process of mandating the vaccines was contingent upon how many people were vaccinated, you had a civic duty not to contribute to that (almost certainly inflated) figure.
Similarly, I knew that because there would eventually be indefinite boosters (which each would have increasing toxicity compared to those preceding it), as a long term strategy it was absolutely critical to not put yourself in a position where they could be mandated on you. This most commonly came up with religious exemptions (which were much more likely to be accepted than medical exemptions since almost nothing is recognized as a valid reason for a medical exemption to vaccination) as if you ever had a vaccination, you effectively waived your right to religiously object to them.
Reviewing the Predictions
As the above examples show (assuming I did indeed predict all of the following would happen), I was fairly accurate. I feel that this is important to share because the same pre-existing factors which allowed me to make those predictions still exist now, and will continue to shape the course of the future.
At the same time, I need to acknowledge the biggest mistake I made. I failed to recognize just how dangerous the spike-protein-producing vaccines would be, and I still deeply regret this error (as my prior research endeavors on treatments for COVID-19 had provided plenty of indications for the toxicity of the spike protein). At the time of the initial healthcare worker roll-out (and one took on a real professional risk for questioning the vaccines), I expected a situation similar to the recent human papillomavirus (HPV) vaccine disaster (discussed here) and I essentially told many people:
The rate of adverse reactions to these vaccines in the trials was very high, you are actually more likely to feel awful if you vaccinate than if you catch COVID-19, and while COVID-19 can be treated, I am not sure if COVID-19 vaccine injuries can be. Additionally, there are many significant long-term safety issues with this novel technology no one has tested for and it is very likely as these come to light you, will regret not having waited to vaccinate.
In hindsight, I would have said something very different, and many of my friends and patients who got vaccinated likewise wish I had been more forceful on this issue. I feel that the fundamental mistake I made was that once I realized that these vaccines were not a good idea, I left it at that and moved on to something else (you can’t study everything). Instead, I should have thought through what the implications were of vaccinating the entire population and done the additional digging necessary to fully answer that question sooner rather than later.
Once the initial vaccines for healthcare workers were given at my facility, I heard a few very strange stories of sudden unexpected cardiac arrests occurring in my healthcare organization but failed to pick up on the signal. Not long after the vaccines were given to the general population, I began to have friends and patients reaching out to me with accounts of the sudden deaths of a relative or friend immediately following COVID-19 vaccination, and I finally realized what was happening. Since I knew that no one was going to listen to me, I decided to do the best I could and document all of these cases so that I could present the evidence to people who were insisting it was not really happening.
Over the course of a year, I ended up learning of 45 cases within my personal circle of someone either dying or developing a condition that would likely prove fatal (e.g., a sudden unexpected cancer), and many more not quite as severe complications from vaccination. Although a few of the things I came across were very weird (e.g., a colleague knew someone who developed auto-brewery syndrome immediately after vaccination), most of what I saw matched exactly what I saw reported for the vaccines across the internet.
After a year, I stopped recording these vaccine injury cases because I no longer had the time to (e.g., this Substack takes up a lot of personal time). Since then, I’ve noticed that the rate that I encounter these histories of these events has continued to increase (e.g., two weekends ago I heard about 8 cases of sudden deaths or soon-to-be fatal cancer following vaccination; this week I came across 3 significant strokes immediately following vaccination, one of which was almost fatal). Similarly, many more people I speak to are now aware of this problem, and recent polling shows that the public feels the same way (e.g., 28% know someone whom they believe may have died from a vaccine and 49% think the vaccines are causing a large wave of unexplained deaths).
Where did the predictions come from?
In December 2019, I started seeing reports on anonymous message boards about COVID-19 in China and realized that it looked like a potential global catastrophe (I have never felt this way about another emerging disease). The thing that specifically informed me of the potential issue we were facing was the media’s choice to deny that any issue existed (“it’s just a flu bro”). This was a signal because the media always overhypes relatively minor viral outbreaks, so I could only infer that if they were doing the opposite, it meant that this was going to become a disaster. Not long after, I came across the Event 201 documents which both confirmed this analysis, and more eerily, accurately predicted what I would soon see transpire in January, February and March.
At the very end of 2019, I was able to see all the pieces falling into place and had a vision of what would transpire over the next few years. My life since that time has essentially been the surreal process of watching that nightmare become reality. However, as stated before, the one error in my initial analysis was under-predicting how dangerous the vaccine would be and I believe that danger is now evident enough to the public that it may be possible to derail the initial trajectory that was planned for every human on the planet.
For the rest of the article, I wish to discuss the pieces that fell into place and how we got to where we are now.
Pharmaceutical Economics
One of the key themes I’ve tried to illustrate in this substack is that the medical industry always follows the same playbook. The goal is to create products that large numbers of people will take on an ongoing basis, and have large enough margins on the product to cover the costs of pushing them on the public (e.g., developing the pharmaceutical, bribing regulators to approve it, marketing it, bribing doctors to push it, bribing healthcare facilities to push it, bribing regulators to protect it and paying for legal expenses for complications from the product which the regulators can’t cover for).
Because so much money is made from pharmaceutical sales, a well-oiled machine has been developed that everyone uses repeatedly to get products to the market. There are two rarely appreciated consequences of this paradigm:
•First, when trying to understand the life cycle of a pharmaceutical product, it must be seen through a lens that considers its profitability and scalability, not its safety and efficacy.
•Second, the entire process does not incentivize the production of safe and effective products. On the contrary, it arguably disincentives them.
Ineffective Pharmaceuticals
Let’s first look at the efficacy of half of this equation:
Consider the life cycle of two drugs, one of which effectively treats a condition and one which may provide a bit of improvement, if administered indefinitely. In the case of the former, it will rapidly destroy its market (since everyone is cured) and a lot of parties will get very mad with the drug manufacturer (e.g., competing companies selling a drug for the condition and specialists who have a significant number of patients with the condition their healthcare facility depends on the repeat visits of). Conversely, if the drug only provides a partial improvement, it has a good chance of fitting into the self-serving drug sales machine (especially since it does not upset any vested interests) and becoming a great commercial success.
Because we operate in a pay-to-play system, it is nearly impossible to bring a drug to market unless it can be expected to recoup the cost it takes to do that. For example, if a drug is known to be safe, effective, and able to meet an unmet medical need but not have any scalability (as it treats the issue and does not require recurring administration) no one will fund the (fairly large) costs needed to get the drug to market. Many of us learned this first-hand during COVID-19 when we attempted to get approval for off-patent medications for treating COVID-19 (e.g., Steve Kirsch funded research that proved fluvoxamine was effective for treating COVID-19, but nonetheless could not get an emergency use authorization (EUA), and I encountered similar headaches with the FDA on the team I led—although we did not make is as far down the road as Steve’s team).
One of the clearest proofs of this dilemma can be found here:
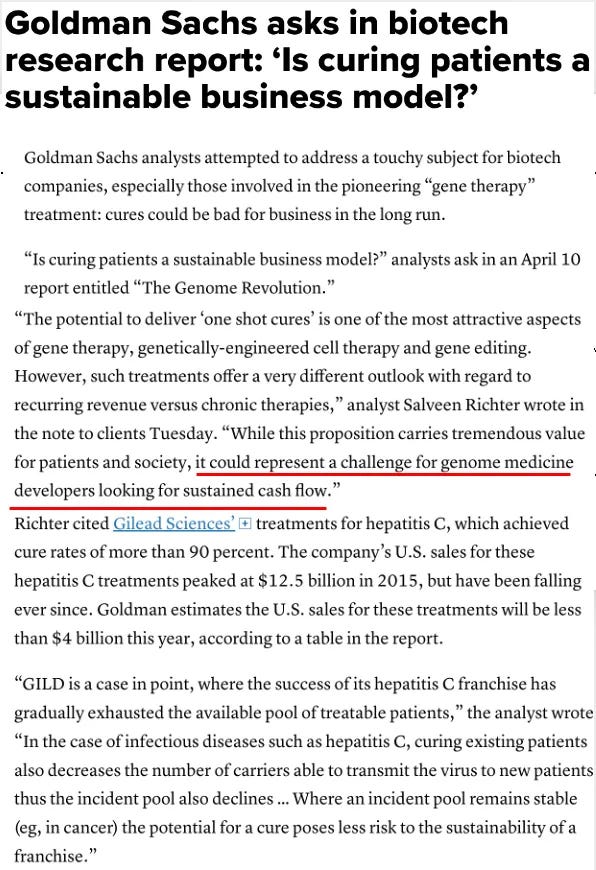
When this report was published, it understandably provoked a great deal of outrage. I, however, felt that they deserved a nod for being honest since they admitted an unspoken truth that exists throughout the pharmaceutical industry

For those wishing to know more about the subject, the saga of Ivacaftor, a life-changing drug for some patients with cystic fibrosis, also illustrates an interesting aspect of the dynamic. This is because the drug could only be brought to the market with 100 million dollars of funding from the nonprofit Cystic Fibrosis Foundation, but once it was approved, the manufacturer who had begged for that funding so it could be moved through the development process nonetheless shot its price through the roof so that many who needed it simply could not get it.
Similarly, one of the unspoken dogmas in medicine is that most viral infections cannot be treated, and thus can only be addressed by prophylactic vaccination. I believe this dogma exists because most of the reliable treatments for viral infections (e.g., the oxidative therapies that successfully treated viral pneumonias such as the 1918 influenza and COVID-19 along with other scourges such as Ebola, AIDS, and Polio) are fairly universal rather than being specific to individual viruses.
Because of this, any of these drugs entering mainstream medical practice would threaten an enormous market, and thus, despite decades of need for therapies like them, they have never had mainstream adoption. Instead, they are only used by independent holistic practitioners, and occasionally in other countries that are not as economically incentivized to have expensive and ineffective therapies dominate medical care.
Knowing this dogma played a key role in how I was able to predict the course of COVID-19. Opening the market for mRNA therapies and permanently establishing another annually required vaccination for all Americans could provide so much future income to the medical industry so it was a foregone conclusion that anything which threatened this outcome would be targeted by every one of our institutions.
Keep in mind that this is also exactly what has happened in the past. For example, when the original AIDS outbreak occurred, Anthony Fauci blocked numerous effective (non-proprietary) treatments from entering the market, despite vocal protests from the gay community.

This was done so that a lucrative but extremely dangerous (and arguably ineffective medication), AZT, could enter the market. Friends of mine who lived through this all told me that AZT made AIDS much worse (AZT’s successor, remdesivir, likewise was pushed by Fauci for COVID-19, and had the same poor results), and that it was ultimately the ones who independently pursued unorthodox therapies who survived the early days of AIDS.
This account has been confirmed by many outside commentators, and since Fauci played a key role in orchestrating both that debacle and the COVID-19 mess, he was also a focus of Robert F. Kennedy’s exposé on the damage Fauci has done to America. Fauci’s past (unpunished) behavior allowed me and many others to predict exactly what would transpire during COVID-19. Similarly, members of the Front Line COVID-19 Critical Care Alliance (FLCCC) have noted that a 2013 movie about AIDS patients trying to get a protocol differing from the one Fauci pushed on America perfectly matches what happened with COVID-19 decades later.
The terribly sad thing about all of this is that much in the same way that AZT made AIDS much more deadly, it had been predicted by many that COVID-19 (like many previous pandemics) would have three waves, and then disappear on its own. However, before that could happen, the vaccines were introduced and instead of the pandemic ending naturally, it has become a permanent fixture of our lives.
I (and others) were worried that the vaccine would trigger the evolution of variants, and would also prevent recipients from being able to develop broad and long-lasting immunity to COVID-19. This has come to pass. The best proof of this is the fact that despite our best efforts, Africa refused to vaccinate, and unlike the rest of the world, COVID-19 has virtually disappeared for them.

If we step back for a moment and think about it, going from “95% effective with two doses” to “1-2 vaccines a year for life will be mandated to reduce your chance of dying from COVID-19” is a pretty remarkable goalpost shift (and all of us who claimed it would happen were simply dismissed as paranoid conspiracy theorists). Unfortunately, since actual efficacy is not a requirement for approval, the industry can frequently get away with doing things like this.
Dangerous Pharmaceuticals
Ten years ago, I read an interesting book about how the visual media industry (and Big Tech) came together to be the behemoth they are now. One of the most interesting points I learned from the book is that there is very little incentive to produce creative and innovative best-sellers in Hollywood. Due to how much money it costs to produce a movie, a relatively safe formula has been settled upon that guarantees that investors will get their money back on a film they finance. Since that revenue stream is almost always guaranteed by fitting within the industry’s box (a lot of money is made from selling things besides the film itself such as merchandise and subsequent video replays) there is no incentive to produce a groundbreaking movie because going outside the standard movie formula entails too much risk. Somewhat analogously, when I wrote this article, I went to check how many Fast & Furious sequels have been made, and apparently, they are now working on the eleventh.
This situation is essentially analogous to what was outlined in the previous section. Such a robust sales apparatus exists for selling most medications, that provided it can be argued they do something (which is much easier to do if they conform to the existing expectations of how pharmaceuticals should work), they will normally make money for the manufacturer. This is also why the majority of drugs (e.g. 75% in 2004 according to the FDA) that enter the market are “Me-too” drugs, which are essentially knock-offs of drugs already in use that are slightly changed so they can be patented and sold to the American public.
Whenever I examine the data behind pharmaceutical drugs, I frequently find that much of the (often minuscule) benefit ascribed to them is an artifact of how their research trials are conducted, rather than an effect of the drug itself. For example, in a recent article on the fraud within the COVID-19 trials, I discussed the many signs that Pfizer’s clinical trial data suggested there was no benefit to taking the “95% effective” vaccines (Arkmedic likewise did an excellent breakdown here).
To some extent, this should make sense since the elaborate business apparatus we have (it costs a lot of money to conduct preclinical drug studies and clinical trials) requires a consistent output of profitable products making it to market regardless of their actual efficacy.
Since you can't fight everything, I have chosen not to get too upset by widely used pharmaceuticals that are ineffective. My focus instead is directed at the pharmaceuticals which I know injure patients, and I have made peace with useless ones that don’t harm anyone. Unfortunately, in the same manner, that ineffective pharmaceuticals can be made to look effective, the adverse effects of harmful drugs can be concealed by unscrupulous pharmaceutical companies.
For example, in a recent article, I discussed how numerous participants have come forward from the spike protein vaccine trials, all stating that they had horrible injuries. These adverse events should have been documented to avoid them in the future. However, rather than these adverse events entering the official report (remember this was a trial for a product that was going to be forced upon the entire world), the participants were gaslighted by the supervising doctors, and their life-altering injuries were fraudulently documented as something fairly benign. I sadly suspected that this would happen since I had seen similar things happen before (e.g., with the fairly recent HPV vaccine trials).
Although the FDA has demonstrated for decades that it is fairly corrupt (as best as I can tell this really began during the Bush and Reagan years on account of how they handled aspartame and Prozac—each of those scandals is astounding), I am nonetheless astounded by how the FDA and the CDC have handled the vaccines. Every possible warning sign is flashing red, top vaccine officials from the agency have resigned suddenly, and for the first time in my lifetime the general public is actually distrustful or angry at these agencies (e.g., the majority of Americans want the CDC investigated), and yet all these bureaucrats are doing is covering up what is happening and doubling down on the vaccines.
Tiger Teams
When I was much younger, I was exposed to public relations, the invisible industry that reliably allows corporate and governmental clients to pay to instill their beliefs into the population. As I have grown older, I have come to appreciate just how many of our cultural axioms (unquestioned beliefs) are the result of someone paying a PR firm to instill that belief, sometimes subliminally, into the public.
Note: ironically one of the severely vaccine-injured individuals in my circle worked on Moderna’s initial PR campaign and at the time fully believed they were doing a public service by manipulating the public into vaccinating.
In many cases, this manipulation is relatively straightforward to do (PR is remarkably effective). However, in other cases, so much is being asked for that goes so far against the existing values of the general public, that a much more elaborate and cut-throat campaign must be engineered to create that cultural shift (so this is only done when there is a huge reward for doing so). Although we just concluded the year of the tiger, I would nonetheless like to quote a previous article that described where the entire COVID-19 debacle came from:
When I was younger, a friend who was a corporate executive told me about “tiger teams,” an approach that industry would utilize to solve a complex problem facing them or to develop a plan for achieving a long-term strategic goal. After he vividly described the tenacity with which they attacked their problem, I realized that large corporations could be expected to conduct highly strategic and Machiavellian plans over long timelines that would be difficult for anyone but the most talented observer to spot.
Since that time, I’ve also come to appreciate how most businessmen and their industries will default to reusing tools that have previously proven successful for addressing each new problem that emerges. As a result, once you learn what each of the tools are, it becomes possible to predict each of the sequential steps a tiger team will choose to accomplish its goals.
Since I have held a long-term interest in the politics of vaccination, I have been able to witness the sequential steps that played out first in California and then throughout the nation. What I still find remarkable about these events was how each one directly enabled the subsequent event, and that in many cases, what happened subsequently had previously been promised to never come to pass.
When you look at the chronology I detailed at the start of today’s article and the more extensive chronology presented within the previous article, it should be clear that this was all methodologically planned out from the start. Huge players like Bill Gates invested a lot of money to set the stage for this to happen, years before COVID-19 emerged, and once the pandemic occurred they made a lot of money off those investments (Gates also bought out many of the media outlets that then suppressed competition to his investments throughout the pandemic).
Normalizing Sickness
Although many medical practices provide a clear benefit, once you begin to examine the routine procedures we perform and the pharmaceuticals everyone prescribes, you often discover there is no real justification for them. Instead, like annual flu shots, they are all just assumed to be something everyone must do that should not be questioned and very few can draw a connection between each one and the widespread harm it has created.
One of the most common questions I receive from readers is my position on circumcisions. Since it relates to the subject at hand, I will discuss it here (note: henceforth I am only referring to male circumcisions; female “circumcisions” are completely unjustifiable genital mutilation that should not be labeled as anything else).
Although I, like many, have strong feelings on this issue, I have tried to give a fair hearing to both sides of the debate, and this is how I believe they break down:
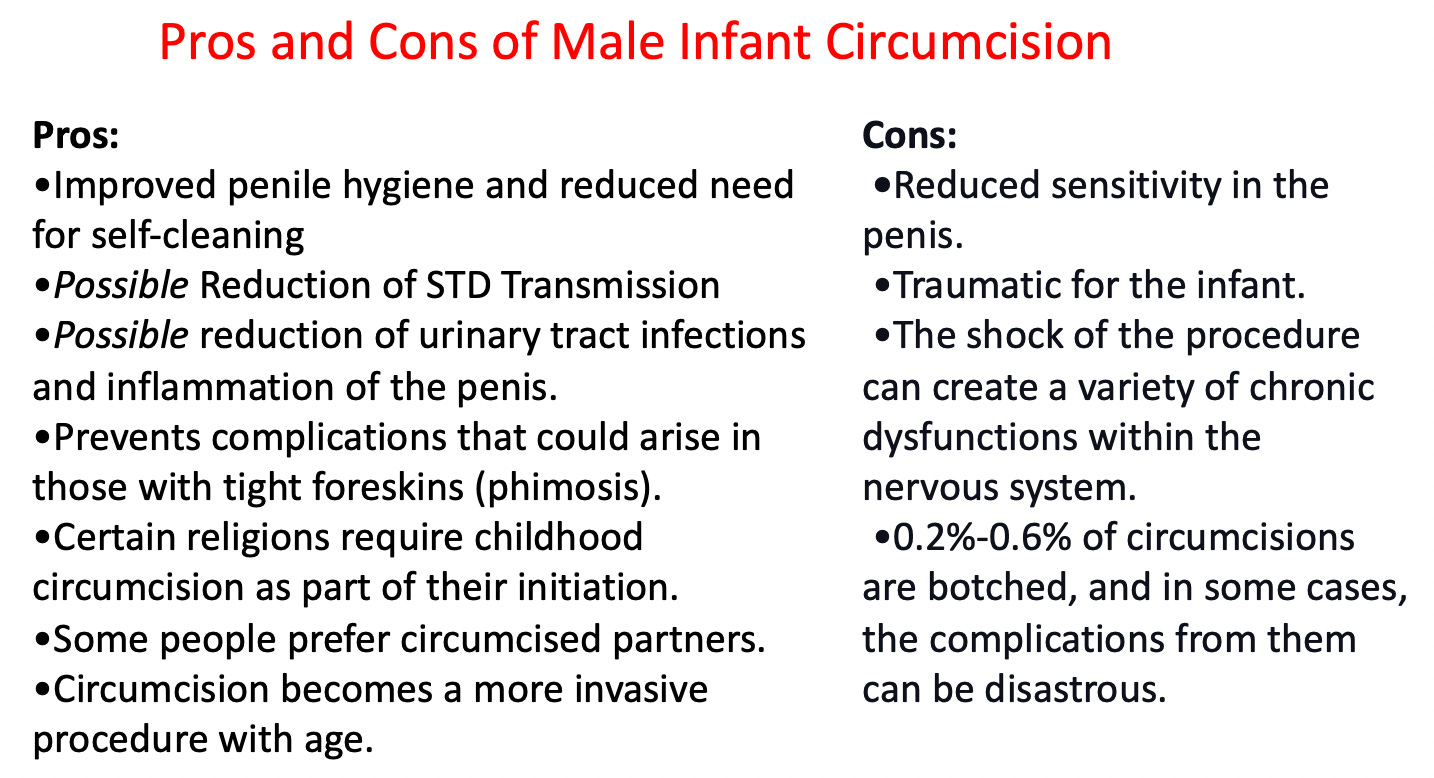
Note: this article provides a good example of the evidence for and the arguments in favor of infant circumcision from a supporter of the practice. It should be recognized that many of those arguments are much more applicable to individuals who live in areas (e.g., Africa) without a developed infrastructure and a climate that is much more conducive to large numbers of dangerous infectious diseases.
My opposition to circumcision is rooted in both ethical and medical grounds and at this point, I view the practice primarily as a traumatic religious ritual, which like infant vaccinations, habituates into becoming a lifelong adherent of Western medicine. Additionally, I periodically encounter patients who have issues tied to their childhood circumcision (some of which they share with me, others which I discover while investigating their current issue), so there is no doubt in my mind circumcisions are not a benign procedure.
Due to my opposition to these practices, I found a way to avoid ever performing either on a child during my medical training (although I have done similar procedures). However, I have seen many done, and over and over I have observed infants or children recoil in fear from the forced procedure and receive traumatic injuries when it happened. What has always puzzled me is that while some physicians I have spoken to have shared my observations, most completely lack the ability to recognize any of this is happening.
As best as I can remember, I have never met a man who regretted not being circumcised as a child. Conversely, I have met more than I can count who sincerely regretted what was done to them. Similarly, beyond observing many infants or children who I felt were refusing to consent to a forced vaccination or circumcision, I have also met a few older children (now capable of speech) who remembered the trauma they experienced when that initiation was done to them.
For this reason, although many (such as the author of the above article) argue otherwise, I do not believe you can ethically justify infant circumcision or vaccination. Until they can understand what is being done to them and either consent or refuse to consent to it, as far as I am concerned, it should not be done.
In a previous series written after Roe v. Wade was overturned, I explored the subject of medical ethics, a critical, but frequently neglected aspect of our profession. One of the areas I focused upon was a major challenge within medical ethics—how inconsistent the principles behind it are, as you will frequently see a principle followed in one case and then tossed aside for another. However, if you instead reframe it as a question of what choice results in a profitable medical procedure, everything becomes much more consistent, as that almost always arrives at the “ethical” procedure.
In the case of circumcisions, I believe their primary reason for being performed is because they are a source of guaranteed income for the doctor (and the facility they work for). The thing I find particularly interesting on this subject is that for most of the doctors I’ve asked who routinely perform these procedures, they are largely unaware of the pros and cons of the procedures. Instead, they just view circumcisions as something you do and rarely even think to question them.
Similarly, with annual flu shots, most healthcare workers just take or administer them and have minimal knowledge of the risks or benefits of the practice. Instead, they either mindlessly comply with the practice and don’t give it much thought either way, or they assume it is critical to prevent severe outcomes from influenza, never really research the subject and make excuses each year that the influenza vaccine inevitably fails because the wrong strain for it was chosen.
Many businesses succeed based on if they can create an unquestioned ritual in the general population that involves using their product. The way Febreeze (something I greatly dislike being around) was marketed is a great example. Similarly, so many pharmaceuticals are parts of checklists everyone uses to practice medicine, and relatively few providers actually will think through if a generally accepted medication makes sense to prescribe each time their checklist tells them to.
Because there are so many things you have to learn to be a doctor, the shortcut most doctors use to navigate the incredibly large body of medical knowledge is to trust in something if everyone does it. Time and time again, you will witness an aggressive campaign to instill a new (and questionable) product into the medical marketplace many doctors of the era oppose, but if you fast forward in time, that product becomes the gold standard few even think to question.
One of the most important articles I’ve written here summarized how the medical system handles the sudden explosion of new diseases due to the introduction of an environmental hazard (e.g., a pharmaceutical, medical device, or pesticide) that no one wants to challenge as doing so would threaten the vested financial interest creating that hazard:
In general, the medical profession will deny the disease even exists and aggressively gaslight those who are suffering from it. Then, as everyone becomes aware the disease exists, the medical industry will come up with a variety of excuses to divert everyone from the actual cause. Eventually, one of three things happens:
•There is no longer a need to protect the hazard causing the disease, the cause will be admitted and the cause will be pulled from the market. This, for example, is what happened with lead no longer being added to gasoline once a safer replacement to it was finally found. Sadly, this outcome is fairly rare as it typically requires a viable replacement to be discovered.
•Activists are able to bring attention to the actual cause and it is pulled from the market. Sadly, this outcome is also fairly rare.
•The disease becomes normalized and people stop remembering that it used to not exist. At this point, it becomes a mysterious “syndrome” (e.g. Sudden Adult Death Syndrome or Sudden Infant Death Syndrome).
Long before COVID-19, I had read of (and often spoken to physicians who directly witnessed) previous instances of massive declines in the vitality of the human species (e.g., what resulted from the early smallpox vaccine campaigns or Fauci’s 1986 law that pushed a plethora of unsafe vaccines on our children). Because of this, within a month of the vaccines hitting the market, I was able to recognize that I was bearing witness to a titanic shift in the health of our species.
Although annual flu shots are a real issue (they periodically cause significant issues, and there is no evidence the decades of use decrease the incidence, transmission, or severity of the flu—to the contrary, they appear to worsen many of these), their harms pale in comparison to what indefinite COVID-19 vaccines could do.
My greatest fear is that these indefinite mandatory mRNA vaccinations and new illnesses will become the new normal. I have absolutely no doubt that allowing this will be immensely detrimental to our species and a large part of why I’ve spent so much of my life over the last 3+ years on this issue is because I believe that future is not set in stone.
Conclusion
One of the major questions with which everyone has had to struggle is why the product that was finally chosen to be mandated upon the entire population was so dangerous (nothing like this has happened since the smallpox vaccines). On the surface it doesn’t make any sense; if there was one single time you did not want to push an extremely dangerous product onto the market, it would be when there was the greatest risk of losing the popular trust that was built up over decades.
At this point, I have come across three explanations for how this could occur (note: a combination of these could also be true):
1) The adverse events were actually desired. The only two potential outcomes I have found to explain this are either population reduction or breaking the public’s trust in their national governments.
Although both of these seem speculative and conspiratorial, there is some evidence for one as there is a longstanding fixation by the Western rulership to appropriately cull their populations, and a variety of immoral sterilization programs have been previously conducted (both of which I did my best to document here). Additionally, numerous vaccines have been evaluated for their capacity to sterilize recipients and the most successful candidate was repeatedly forced upon women of childbearing age in the third world (which I documented here).
2) The adverse events were viewed as an acceptable trade-off for the intended goal. This could be a direct financial reward (e.g., getting a blockbuster product or opening the mRNA market), an indirect financial reward (e.g., having a vaccine that failed so that updated boosters would always be needed), or something completely different like making a tool kit be available to change the genetics of the human species.
3) They royally screwed up, and the vaccines were much more dangerous than was anticipated.
A decent case can be made for any of these options (especially since many outside scientists who did not even have access to Pfizer’s or Moderna’s data recognized the spike protein vaccine design was both unsafe and likely to quickly stop working, whereas many better options were glossed over). Similarly, a large increase in deaths and a decrease in live births have occurred since the vaccines rolled out, which argues for a depopulation narrative. However, even when considering those arguments, at this point, I believe the most probable explanation was a monumental screw-up.
I would argue this is actually an extremely fortuitous outcome since it has created a window to derail the train of ever-growing corruption with which the industry has entrapped our society. Our societal relationship with pharmaceuticals has gotten much worse as the decades have gone by, but the rate by which it has happened has been just slow enough that public protests against the ever-encroaching industry are small enough to suppress.
Because this shift now is so extreme, it has motivated people to act who, in the past, would have typically sat on the fence. For example, based on our presently accepted standards, imagine how many feel who know people around them who died suddenly after the vaccine and are worried that the same will happen to them or their loved ones.
The only time I can think of where something like this happened was during the early smallpox vaccination campaigns. That is because these vaccines did not work, often caused smallpox outbreaks or seriously injured patients, and required progressively more draconian mandates to be implemented, which were eventually met with some of the largest protests of the era.
When this happened, the protesters were successful, and the mandates were scrapped. Unlike that bygone era (where it took decades to end the smallpox mandates), today, due to the internet facilitating rapid communication around the world, those same changes can occur in a much faster fashion, and the traditional forms of propaganda that have been used to direct our society for over a century are now powerless to stop competing narratives.
Many attempts have been made to stop this from happening (e.g., Peter Hotez spent 2019 going on a media tour to lay the stage for the deadly censorship we saw throughout the pandemic and he is still aggressively promoting it). However, because of the times we live in, the censors have ultimately failed, and these two unprecedented events (a serious reason to distrust the government and losing the ability to censor the population) have converged to create a political movement that has a good shot at overturning a lot of the terrible things that have happened over the last few years.
One way or another, a lot of large changes are going to happen this year. Many are now willing to pay for a better form of medicine (e.g., one that does not involve annual COVID-19 boosters) and to publicly share their distrust of the mainstream narrative with others (along with institutions like the FDA). These are very powerful social forces, and it is my sincere hope that each of you can help us work towards making those changes that transpire this year be positive ones and not a future like this:

In summary, I hope this article has made the case that the vaccine industry is relentless and unless we put our feet down, this will continue to escalate (remember that COVID-19 vaccine efficacy declines after a few months, so they may ultimately pushed for even more than annual COVID-19 vaccines).
Lastly let me know if you want me to write more about the corruption in the FDA and the revolving doors between our healthcare regulators and the pharmaceutical industry alluded to by Pfizer’s scientists. In the meantime this is one excellent example of the problem.

Thank you so much for your support and sharing this article with those who could benefit from it.
The first lie that must be dispensed with is that there ever was a pandemic.
Repeating that lie covers up the criminal acts that occurred in hospitals and nursing homes which were the justification for the phony pandemic and falsely catapulted the Big Lie that there was some dangerous "novel virus" that threatened people- there wasn't.
There was no "pandemic."
It’s imperative that everyone stop ceding ground to these fascists by reifying the Big Lie that "Covid" is a unique disease and that it is responsible for a global pandemic.
"Covid" the disease is pure fiction. All the rest of it (biolabs / batsoup / bioweapons / lableaks) is political theatre and bread and circuses. They gamed the system to code for "covid deaths."
This has never had anything to with what is nothing more than a computer-generated genome falsely attributed to a novel pathogen. It is a global conspiracy by the worlds transnational ruling class which was planned out and war-gamed at the WEF, the central bankers summit in Jackson Hole, and at Event 201.
Once you get people to assent to a world that makes no sense you can get them to do anything. That's precisely what the Covid Cult is: it competes with the real world. Strategy of tension, mass mind manipulation, a psychological operation, the general population hypnotised right in front of your eyes.
99% of people falsely certified as having ‘died from covid’ actually died from their preexisting conditions being exacerbated by mass medical malpractice and ‘public health’ despotism, the other 1% simply died of old age.
Translation: No one has "died from Covid" as “Covid” is nothing more than a fraudulent PCR result plus a nebulous clinical re-branding of cold, “flu” and many other disease conditions
This is all just so insane.