

A Massive Spike in Disability is Most Likely Due to a Wave of Vaccine Injuries

This article has been revised and updated here:
Early in my medical practice, I elected to work with individuals seeking disability because there was a shortage of doctors in my area willing to do these exams (they do not pay well and we had a physician shortage to begin with). My personal reason for involvement was that due to this shortage, many individuals who desperately needed disability were facing significant delays moving through the process, which often rippled out into causing significant problems in their lives and those around them.
While a few people I saw were suffering from self-created problems and some were either faking their condition or exaggerating their disability for money (which is the typical lens disability claimants are seen through), I found the majority had been through significant hardship that resulted in a life impairing disability (some of their experiences were pretty horrific). I took this as a sign a lot of vetting was done by the state before they were sent to me.
In many of these cases, I felt if the individual had been my patient, they would not have arrived at the place they needed to seek disability. Many of them either had iatrogenic complications from the poorer quality of medical care that individuals in state insurance programs like Medicaid have access to, and had problems that would relatively fixable within a more integrative model of medical care if they had had access to one.
A frequent topic of discussion with my colleagues was whether granting someone disability was ultimately a harmful thing to do since it removes their motivation to address their illness. This is important because in almost all cases, being disabled and receiving disability is a far worse life than not being disabled and having employment. I always kept this in mind when I evaluated these claimants, and ultimately recommended disability for many of them.
I found the majority of claimants I saw did not want to be disabled, had tried over and over to get better, hated going through the process and were only doing this because they had no other choice left. It also made me particularly sad that many of them said I was one of the first doctors they met who treated them as a human being, something I once again view as a consequence of my working in a socioeconomically impoverished rural area where these patients only had access to the inferior quality of medical care afforded by state medical insurance.
From this job, I came to view the disability process as the last stop on the train for individuals who had been failed by the system. Due to the legal requirements of providing an impartial medical evaluation, I was not allowed to provide any type of medical advice to these individuals and I eventually quit the job because it just made me depressed and there was nothing I could do to help the people I saw.
Today I learned Ed Dowd (the Blackrock executive who broke the story of the spike in life insurance claims following the vaccine rollout) discovered something very, very concerning (which can be verified here):

Let’s quickly annotate that to put it into context:
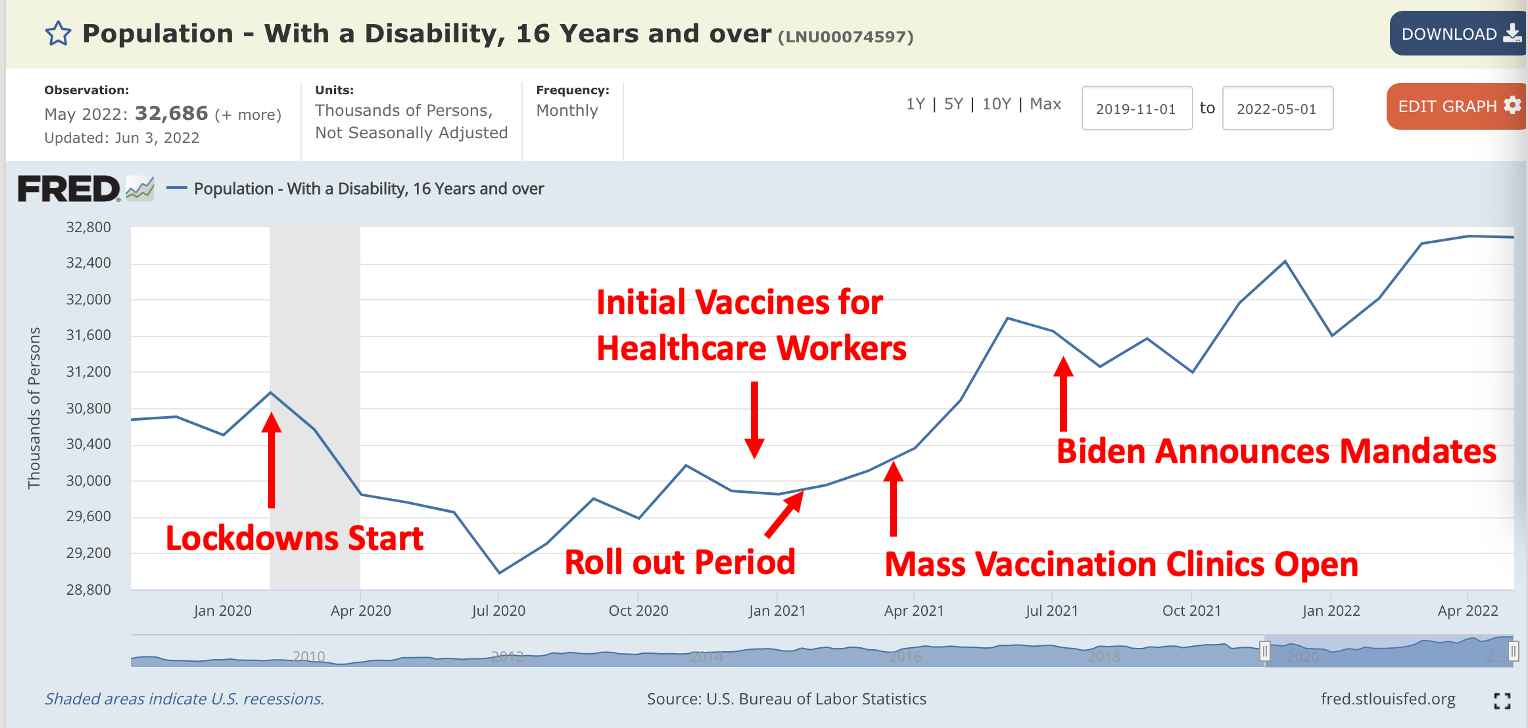
When I initially looked at this data I thought it referred to individuals on SSI disability, and I could only see a few possible explanations for it besides Vaccine Injuries (such as a temporary pause in disability examinations being done at the start of the lockdowns because they were "non-essential"medical services). Since this does not refer to the SSI disability, problems, I do not believe any of those alternative explanations could apply here and have removed them from the article. Based on this data it is abundantly clear the vaccines must be viewed as the primary cause of this spike in disability until another cause can be proven.
For reference, the BLS defines disability as follows:
How are people with disabilities identified in the CPS?
The CPS uses a set of six questions to identify persons with disabilities. A response of “yes” to any one of the questions indicates that the person in question has a disability. The disability questions appear in the CPS in the following format:
This month we want to learn about people who have physical, mental, or emotional conditions that cause serious difficulty with their daily activities. Please answer for household members who are 15 years old or over.
•Is anyone deaf or does anyone have serious difficulty hearing?
•Is anyone blind or does anyone have serious difficulty seeing even when wearing glasses?
•Because of a physical, mental, or emotional condition, does anyone have serious difficulty concentrating, remembering, or making decisions?
•Does anyone have serious difficulty walking or climbing stairs?
•Does anyone have difficulty dressing or bathing?
•Because of a physical, mental, or emotional condition, does anyone have difficulty doing errands alone such as visiting a doctor’s office or shopping?
Labor force measures from the CPS are tabulated for persons age 16 and older.
A more precise breakdown of this data can be viewed here (thank you to the reader who sent me this), and I would strongly encourage a data-minded individual on this platform to do a more detailed analysis of it. As there are a large number of graphs, I have included them with explanations of their findings as an appendix to the end of this article. Overall, each of these datasets indicate the increase in disability was independent of the lockdowns changing the employment opportunities for those in the workforce. This additional data greatly strengthens the argument this dataset is showing vaccine related disability occurring on a societal level, and that many people with vaccine injuries are nonetheless struggling to maintain employment (which matches numerous anecdotal reports I have heard).
Previously on here I published a log (which I periodically update) of the horrific number of people I knew who had most likely been severely injured or killed by the vaccines. Many of these individuals developed conditions that would result in disability. Two of these individuals were well below the retirement age (putting them in the demographic that can receive disability), were friends of mine, and developed a permanently disabling condition that despite their best efforts they were unable to address, which resulted in them being unable to work for over a year. I also had two acquaintances with a similar experience, one of whom was able to eventually mitigate her disability with a lot of integrative therapies and the other who was not. Lastly, I had a few close friends who developed reactions that could have been permanently disabling but that they ultimately recovered from.
I spent the day going over it, and I believe I have approximately 200 friends I am close to and periodically correspond with. I am unsure what percentage of those in my circle were vaccinated because my personal friends tend to belong to the demographic that tended to oppose the pandemic agenda, but many of my friends are also in healthcare (which has a higher vaccination uptake rate), so my guess is between 50-75% are vaccinated.
In short, using that sample size and dismissing the possibility a permanently disabling reaction occurred I was unaware of (which would inflate the figure), this means 1-2% of those vaccinated develop permanent disability.
In comparison, in 2017, there were 204,572,397 adults in the United States between the ages of 18-64 (I could not find this statistic for 2022, but there has been 2.2% population growth between 2017-2022, so the figure is essentially the same). There are also 54.1 million adults over 65, but many of them live in elderly care homes, and a small number between the ages of 16-17.
Assuming you take the number of people with disability in the USA at the time the lockdowns started (before the dip) and compare it to April 2022, there have been 2,800,000 additional individuals who became “disabled”, or 1.37% of the eligible population, and 1.76% of the U.S. population who had received at least one vaccination as of April 1, 2022 (note: the vaccination rate would likely be different for those aged 18-64 but I could not get that figure and these %s are between 5-20% too high since adults over 65 are not being included), but nonetheless all of this is within the 1-2% range of my sample.
As I thought it over while initially writing this article, I realized a sizable portion of the disability claimants I saw had conditions that had a significant overlap with the common permanent complications of COVID-19 vaccinations such as crippling autoimmune conditions, severe neurological disorders and heart failure, making them unable to perform basic tasks that would be required at a labor site. Most concerning, this increase has not yet leveled off, which is somewhat congruent with chronic COVID vaccine injuries worsening over time and often following successive booster shots.
I have read through reports in a variety of support groups for individuals with permanent injuries from the COVID vaccines and I believe many of them would qualify for disability if they were to pursue the case. Their conditions resemble a subset of the disability claimants I worked with, although in general their conditions are much more severe.
My general impression from working with a large number of patients with chronic illnesses (particularly iatrogenic illnesses) is that they typically file for disability at a much lower rate than individuals with other equally disabling conditions. These patients do not want disability and if they file for it, they only file for it as a last resort.
Unfortunately, as it is for all intents and purposes impossible to get compensated for a COVID vaccine injury. To my knowledge, despite thousands of claims being filed and a promise at the start of the pandemic that vaccine injuries would be taken care of, there has not yet been a compensation claim for a COVID vaccine reaction awarded in the United States. As a result, disability is often the only avenue these patients have.
At this point, I have seen some statistics indicating that disability payments have also gone up, but the Social Security Administration takes about 3 years to publish data for disability statistics (and it will likely be about 1-2 years from the time of vaccine injury to when disability is awarded), so it will be years before we find out if this increase in disability has translated to an increase in individuals on disability.
Many of the individuals who would qualify for disability within this criteria are not disabled enough to be given SSI (the government has everything they can to avoid having to put people on lifelong disability). However, pharmaceutical injuries almost always distribute on a bell curve, with less injuries being more common than severe ones. This means that if there has been an increase in this form of disability, there is almost certainly an in SSI qualifying disability, but the degree of this increase remains to be seen.
Many of our pandemic policies have had horrific implications for the long term economic viability and super power status of the United States. Curiously, very few people have yet recognized or fully appreciated their implications. Having an influx of millions of people developing permanent or partial disability is one such critical death blow for the economy and may become an unfolding catastrophe in the upcoming years. In my next article a few others potential catastrophes caused by the pandemic response will be also discussed.
At the time I initially wrote this article, I concluded with:
Lastly, I must admit I feel a bit nervous being the first person to advance the argument made here. I did my best to think this through and vet it, but I would sincerely appreciate if any other physicians who have worked with disability services or anyone who has a deep level of familiarity with the disability claims statistics can provide any needed critical feedback for this story.
As I made the initial mistake of thinking this was referring to the SSI payments, I have to own that and keep this here. Nonetheless, I still think this makes a valuable point as a large dataset tangibly showing the debilitating injuries being created within the population by the COVID vaccinations.
Many people have argued this is being caused by long haul Covid. That cannot be argued because the trend was not present for the initial year of the pandemic. If you remember not too far back, one of the primary reasons that was cited for why you had to get vaccinated was how terrible long haul Covid was and that the vaccines would prevent it.
I am also of the opinion that a large number of vaccine injuries are being erroneously classified as "Long Haul COVID.” It is extremely common in the unfalsifiable belief structure of Western Medicine to classify an injury from a medication as actually being due to a deficiency of that medication. One of the best (and sadly very common) examples detailed in a recent article is the withdrawal symptoms from SSRIs in previously healthy individuals causing individuals to develop severe psychiatric symptoms (including violent psychosis) then being interpreted as the individual having a pre-existing psychiatric condition they need the SSRI to treat. The same also occurs with SSRIs causing a variety of other psychiatric syndromes such as bipolar disorder, all of which are labeled as the SSRI "unmasking" a pre-existing mental illness, which ignores the fact that the illness would have never been "unmasked" if they had not taken the medication, and population level studies showing the adoption of these drugs directly correlates with the increases of their commonly cause mental illnesses.
The symptoms of long haul Covid and Covid vaccine injuries have a significant overlap and respond to similar treatments. To this point, the NIH was fully aware of this by early 2021, as they were using the same scale used to evaluate long haul Covid to evaluate vaccine injuries, which the NIH then classified as vaccine injuries in their scientific publication on the injuries.
Given the enormous political pressure to have a way to dismiss these injuries and continue incentivizing widespread vaccination, it is reasonable to assume this erroneous classification would be the default solution. The overlap in the symptoms between these two conditions make it very easy to trick gullible people. To that point, I and others have seen countless cases of individuals both online and in person reporting classic descriptions of vaccine injuries, admitting they have been repeatedly vaccinated, and citing their horrific experience with long-haul Covid as a reason why it is crucial for everyone to be vaccinated.
It is also possible the vaccines have dramatically increased individual susceptibility to COVID, as discussed in the previous article which shows this occurring was abundantly clear from the existing science on the mRNA vaccines before they entered the market. However, even if increasing long haul COVID is the primary cause, that still means the increase in disability is ultimately due to the vaccines as they increased the likelihood of long haul Covid occurring within the population.
Appendix:
From looking at the subdivisions of the labor force data, a variety of question about the data can be answered.
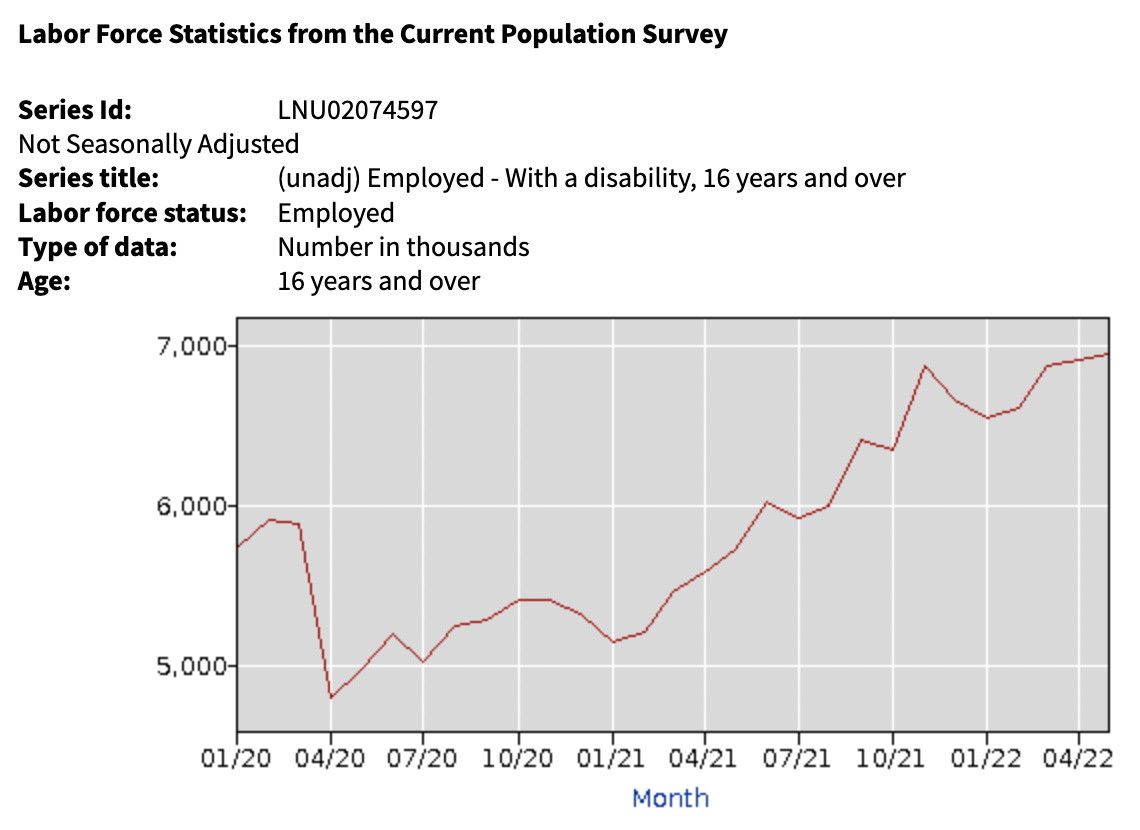
The above dataset shows that the lockdowns resulted in employed individuals with disability temporarily decreasing (most likely because they became unemployed due to the lockdowns), and then increasing by 18% (5,888,000 to 6,961,000). As vaccines are more likely to partially than fully disable and members of the labor force were the most likely to be required to vaccinate, it makes sense that the largest increase in disability would be seen in this subset of the data-pool.

“Unemployed” is defined as not having a job but seeking work. A reciprocal relationship is seen with the unemployed dataset (keep in mind this represents approximately 10% as many people as the above one). An initial spike was seen in unemployed with disability (since those who were employed and had disability lost their jobs due to the lockdowns), who then left this dataset once employment opportunities arose. Removing those who temporarily lost work, there was an increase from baseline in the number of unemployed individuals with disability, but it is much harder to discern the effect here. This is likely partly due to the fact unemployed individuals were not subjected to vaccination mandates.
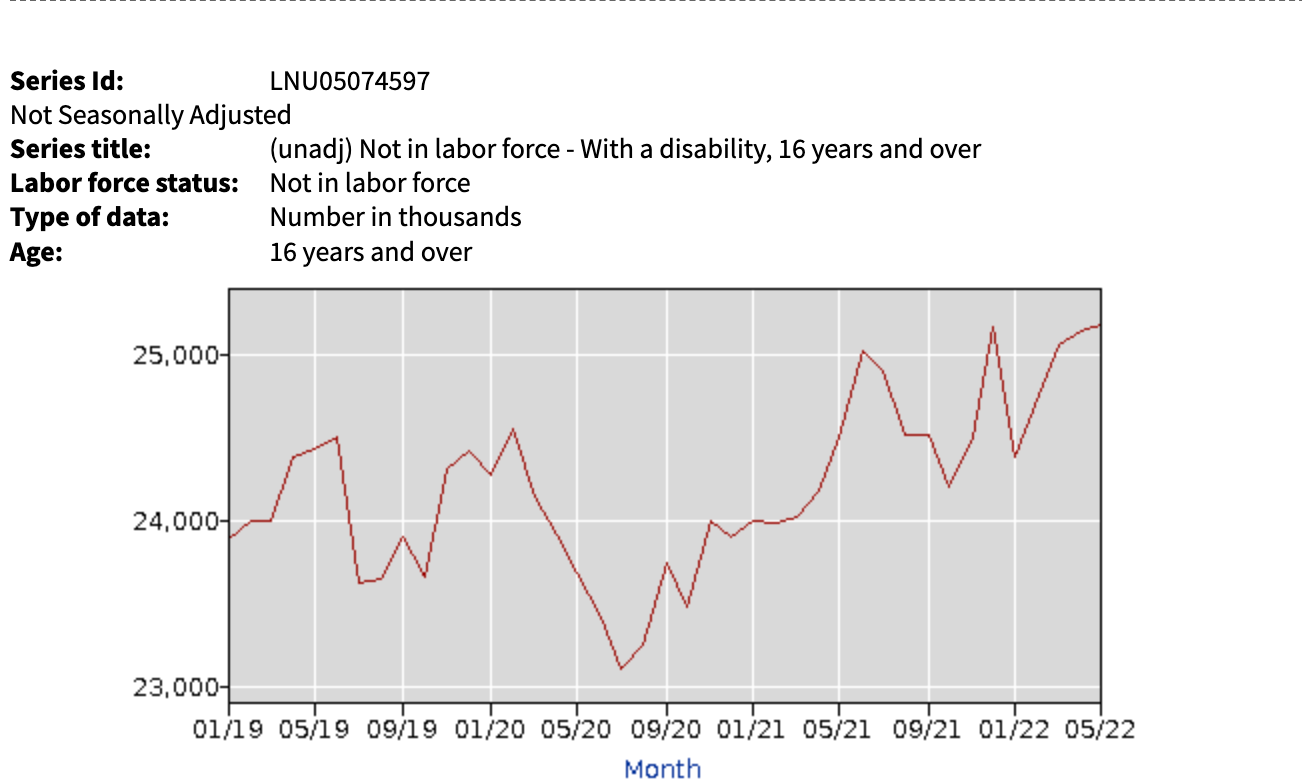
For those neither employed nor seeking work (classified as not in the labor force) and with disability, a clear trend appears. There was a brief drop in their numbers during the lockdowns (my best guess is that they either passed away during this period as this population is more susceptible to illness and stress or started looking for work because they realized the lockdown no longer made it viable for them to remain unemployed). These changes leveled out, and factoring in seasonal variations of those not in the labor force, returned to baseline. Once the vaccination started, there was a 4.9% in the numbers of individuals not in the labor force (24005 to 25189) developing disability.
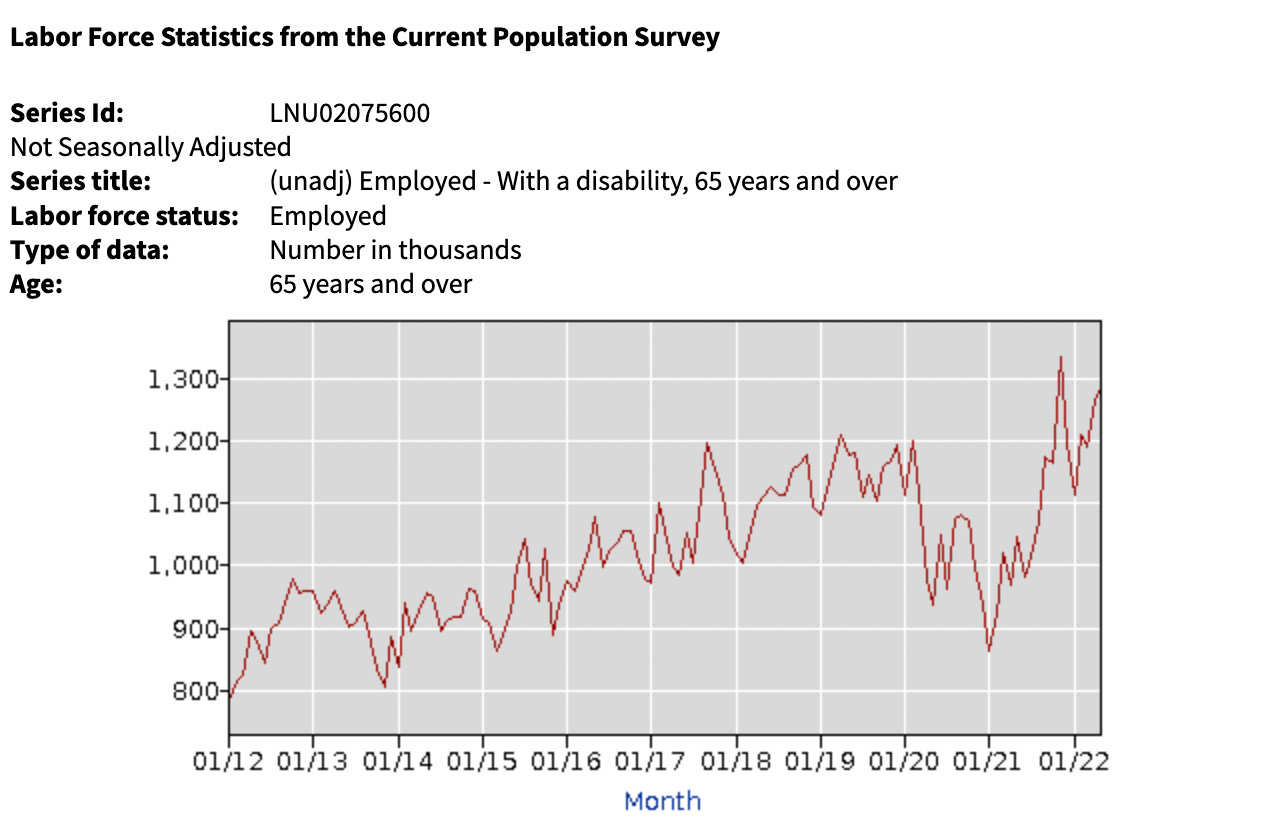
If we look at individuals over 65 who were employed, we see that there was an overall 15.5% increase (1,113,000 to 1,285,000) in disability. Additionally, this graph shows the sharpest trend in increases following the vaccine roll out, which makes sense since the elderly got the vaccines first and had high uptake rate. In the space of 10 months we saw a 54.4% increase (865,000 to 133600) in the rate of disability.
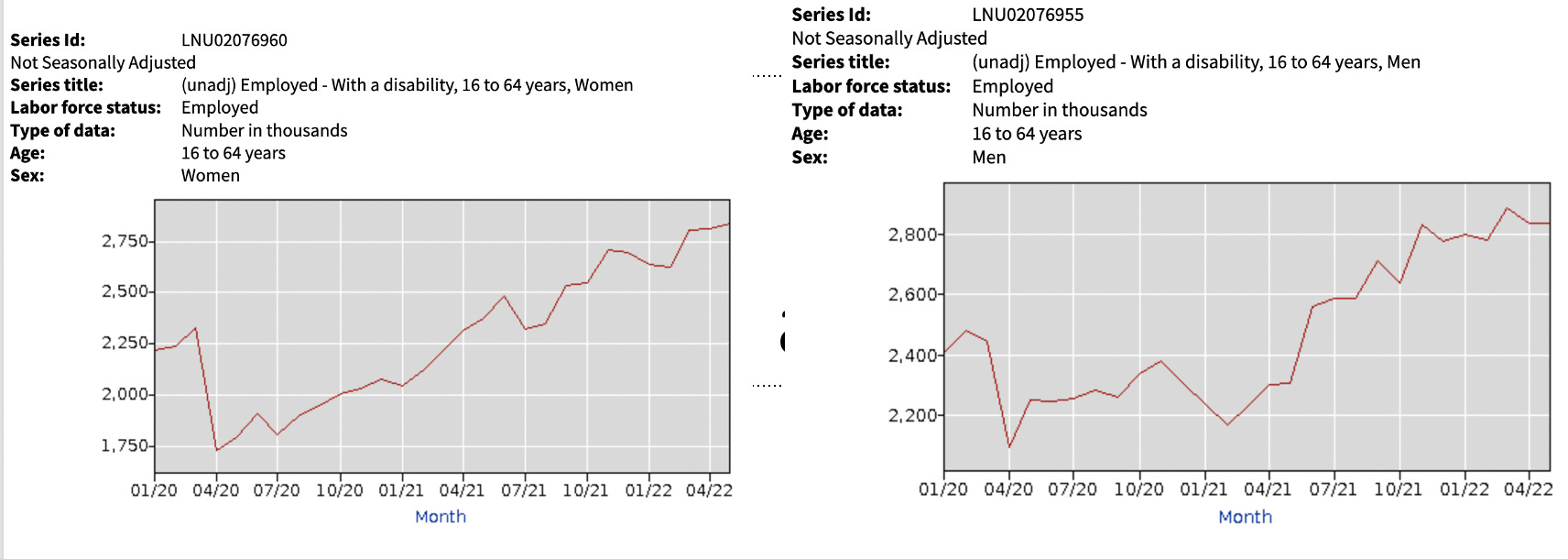
When we compare women to men, we see that women were faster to regain employment after the lockdowns (my best guess is they had a slightly easier transition to remote work, which ultimately resulted in a significant decrease in the employment gap between the sexes). Once the vaccines entered the market, from Feb 2021 to now, there was a 34.1% (119,000 to 2,842,000) in disability amongst working women and a 27.1% (2,236,000 to 2,842,000) increase from baseline of employed women with disability. For men, there was a 30.8% increase (2,166,000 to 2,834,000) after initiation of the vaccination campaign and a 14.1% increase from baseline (2,483,000 to 2,834,000
Now let’s compare the above trends in employment to the changes in employment status for non-disabled individuals.
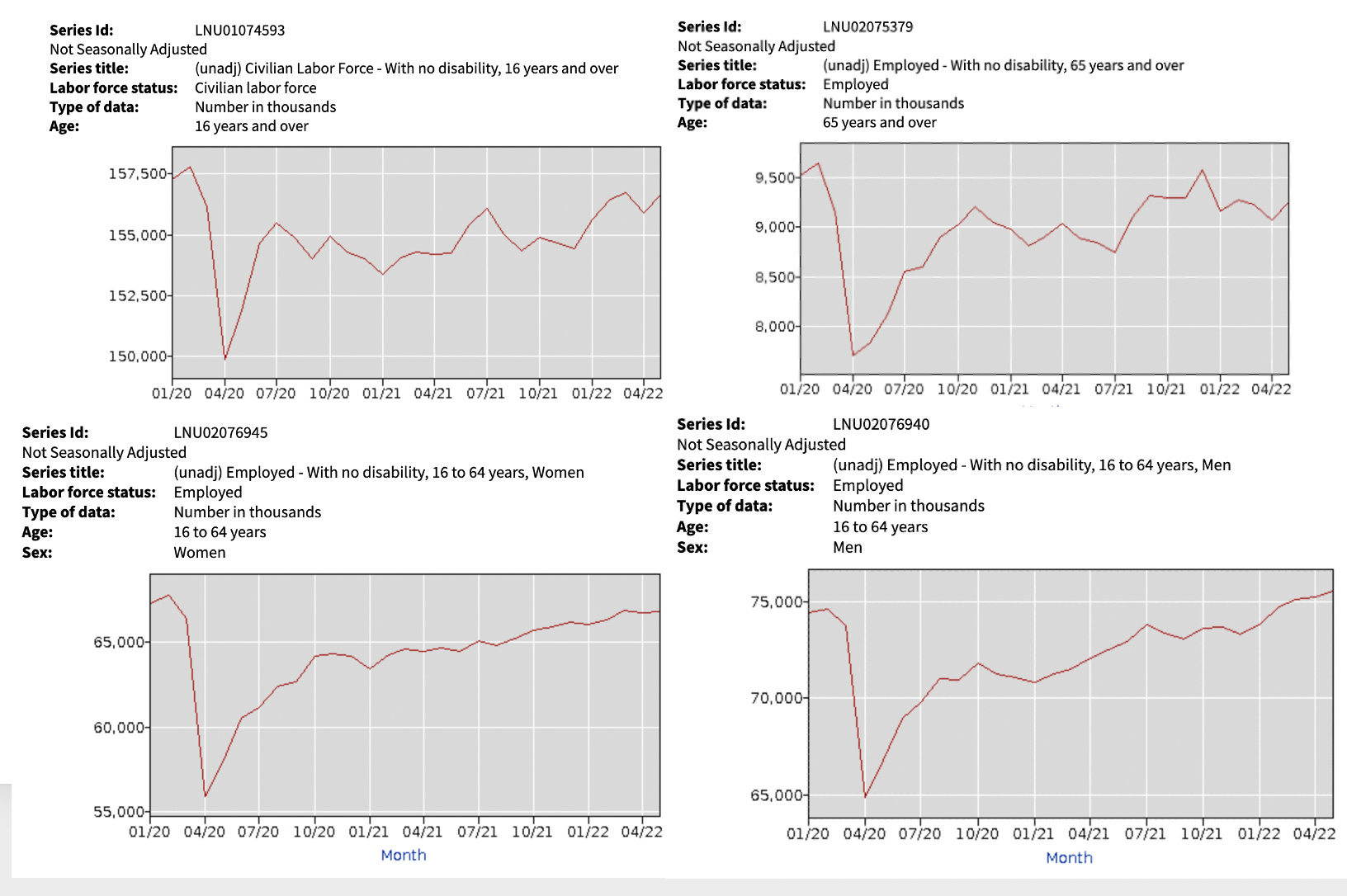
From this, we can see that while there was a reduction in employment due to the lockdowns, the overall rates of employment have remained relatively unchanged (except for a small decrease in those aged 65 and older). Additionally, the implementation of the vaccine campaign (except for men) did not affect employment rates. This means that it is highly unlikely a confounding variable from changes in employment opportunities could account for the marked increase in disability seen immediately following mass vaccination campaigns.
Note: When this article was originally written, I thought the dataset was referring to individuals on SSI disability, not individuals who met a different criteria of being disabled. The central point still holds true (this data set more directly shows the correlation to vaccine injury, but less clearly shows the economic impacts of that injury), but the information in this article has been heavily revised and I apologize for the initial error. I think the experience vaccine injured have with the disability process is important so I am keeping that within the article even though it is no longer directly relevant to this data.
Agree heavily with the first part of this article. As someone with CFS/ME I spent a number years arguing with myself over the need to get a disability allowance and the shame and embarrassment of it all. Which resulted in me most probably worsening my condition with the anxiety and extra activity which resulted. Along with damaging my finances and prior savings which could potentially have been spared if it was addressed earlier.
And secondly, if those with an iatrogenic injury were to claim it was something else. Eg spontaneos onset of lupus, CFS/M.E or FND etcetera and get disability on those grounds, would that help tie them over financially? At least somewhat.
Or could this just muddy the statistics making the vaccine mandates seem less damaging than they really are?
This is absolutely right. In addition, vaccinations disrupted immune systems of many people, and thus when they have Covid, or several, the infection results in a disability. The authorities simply blame Covid, but the disability would not have happened, had not the person been vaccinated prior.
This results in a complicated situation that authorities want to keep complicated and unresearched.
Thank you for clarifying what you are seeing in your practice.